
Abstract
Abstract
Severe obesity defined as an age- and gender-specific body mass index ≥120% of the 95th percentile in children younger than 5 years is well recognized as a significant challenge for prevention and treatment. This article provides an overview of the prevalence, classification of obesity severity, patterns of weight gain trajectory, medical and genetic risk factors, and comorbid disorders among young children with an emphasis on severe obesity. Studies suggest rapid weight gain trajectory in infancy, maternal smoking, maternal gestational diabetes, and genetic conditions are associated with an increased risk for severe obesity in early childhood. Among populations of young children with severe obesity seeking care, co-morbid conditions such as dyslipidemia and fatty liver disease are present and families report behavioral concerns and developmental delays. Children with severe obesity by age 5 represent a vulnerable population of children at high medical risk and need to be identified early and appropriately managed.
Introduction
Childhood obesity remains a significant medical and public health concern in the United States. While the prevalence of obesity seems to be leveling off in certain age groups, the prevalence of severe obesity has continued to increase.1,2 According to the NHANES data from 2015–2016, 6.0% of youth 2–19 years in the United States have severe obesity, defined as ≥120% of the 95th percentile for body mass index (BMI), with 1.8% of children aged 2–5 years affected. 2
This article provides a narrative review of obesity in children younger than 5 years with an emphasis on early-onset severe obesity. It examines the classification of severe obesity, patterns of weight gain, prenatal, genetic, and medical risk factors, and characteristics, which will be helpful in understanding the young child with severe obesity and developing potential subtypes for targeted interventions in the future. In recognition of the limited body of literature on severe obesity in the young child, we also highlight risks for obesity and emerging areas relevant for the clinical care of this vulnerable patient population.
Definition of Obesity and Severe Obesity
The US Center for Disease Control (CDC) recommends that growth charts should be used to monitor patterns of weight gain and growth. For children younger than 2 years, the recommendation is to use the 2006 World Health Organization (WHO) weight-for-length growth charts, with obesity defined as weight-for-length ≥97.7 percentile (as shown in Fig. 1A). 3 No further subclassification of obesity severity has been proposed for children <2 years. For children and adolescents 2–19 years of age, obesity is defined as BMI at or above the 95th percentile of the sex-specific 2000 CDC BMI-for-age growth charts. 4 The definition for severe obesity in children is still evolving, and several classifications have been proposed.5–10 Cole and Lobstein proposed using the extended international Obesity Task Force (IOTF) cutoff points, 6 which correlate with adult BMIs of 30, 35, and 40 kg/m2 and are based on the skewness, median, and coefficient of variation of the curves. 7 A BMI ≥the 97th percentile, which is the highest level shown on the CDC 2000 growth charts (as shown in Fig. 1B), and BMI ≥99th percentile have been used previously as a criteria to define severe obesity. This latter criterion identifies a cut point where children are at particularly high risk of biochemical abnormalities. 8
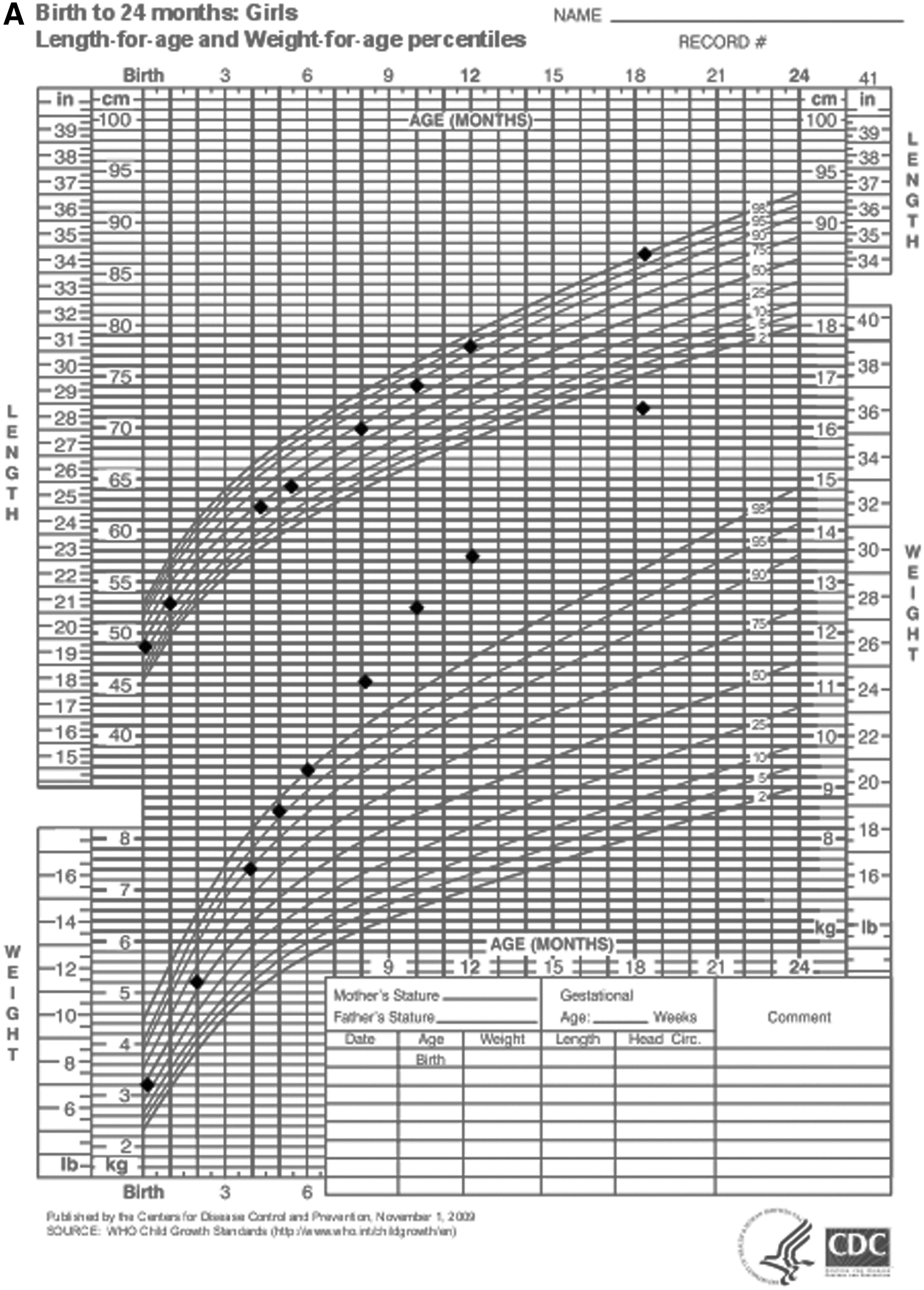
(A, B). Weight Trajectories. These graphs depict the weight trajectory of a child with early-onset obesity. Charts obtained from the U.S. Centers for Disease Control and Prevention (www.cdc.gov/growthcharts).4 *Note the child crosses percentile bands before 1 year of age (Fig. A), with continued accelerated BMI trajectory after 2 years of age (Fig. B). BMI, body mass index.
However, extreme percentiles extrapolated from the CDC-supplied lambda-mu-sigma (LMS) parameters do not match well to the empirical data for the 99th percentile. Because of concern for validity of estimates at BMI extremes, which are extrapolated from sparse data, it has been proposed that a more stable estimation of severe obesity may be to use BMI values above the 120% of the 95th percentile or an absolute value above 35 kg/m2 in children older than 2 years.8,9,11 The use of this criterion is supported by recent studies demonstrating a weak association of BMI z-score with measures of adiposity in children with severe obesity. 12 The American Heart Association endorses using this criterion as a definition for severe obesity, as it aligns with the criteria for Class II obesity in adults. 10 To approximate Class III obesity in adults (BMI at or above 40 kg/m2), an additional category using 140% of the 95th percentile BMI value has been suggested. 5 Table 1 shows a summary of the proposed definitions of severe obesity in children. For clinical and research purposes, use of 120% and 140% of the 95th BMI percentile criteria is helpful for categorizing and tracking severe obesity throughout childhood. However, lack of uniformity in the diagnosis and classification of obesity in children younger than and older than 2 years makes it difficult to follow trajectories from early infancy. Future studies are needed to standardize definitions and categorization of obesity throughout a child's lifespan.
Definition and Classification of Severe Obesity in Children
AHA, American Heart Association; BMI, body mass index; CDC, Center for Disease Control; IOTF, International Obesity Task Force; WHO, World Health Organization.
Comorbidities Associated with Severe Obesity
Childhood obesity is of concern because of short- and long-term health consequences. 13 Children at the highest levels of BMI are usually at the greatest risk of obesity-associated adverse health outcomes.10,14,15 Among 2–5 year old children with obesity or severe obesity, there is paucity of studies on the comorbidities; thus the information available is limited to retrospective studies from clinical programs.16–22
Cardiometabolic Abnormalities and Insulin Resistance
Much of the available evidence on cardiometabolic risk in preschool-aged children comes from a single cohort study of 219 children aged 2–6 years with overweight or obesity. 16 About 39% of these children had at least one metabolic abnormality. 16 Of these children, a third had a homeostatic model assessment for insulin resistance (HOMA-IR) level greater than 1.58, the threshold used to define insulin resistance in this population. Nonalcoholic fatty liver disease (NAFLD), a metabolic abnormality associated with insulin resistance, was identified in 31% of the children (mild NAFLD in 88% and moderate in 12%). 16 The diagnosis of NAFLD in this study was based on ultrasound detection of hepatic steatosis, and was graded as absent (normal liver echogenicity), mild, moderate, and severe depending on degree of parenchymal echogenicity and visualization of the diaphragm, portal vein borders, and posterior portion of the right lobe. Hypertension was seen in 13% and dyslipidemia in 25% of these children. 16 In another study of 140 children, aged 2–5 years, with severe obesity (defined as >99th percentile BMI), who presented to a weight management clinic, 88% had at least one laboratory value that was abnormal 17 ; hypercholesterolemia and hypertriglyceridemia were the most frequently identified abnormalities and they occurred more frequently in boys. 17
Pulmonary Disease and Sleep Disorders
Studies indicate a positive association between BMI and prevalence and severity of asthma among children.19,20,23,24 Among children aged 2–5 years with severe obesity, presenting to a weight management clinic, snoring was reported in 48% and shortness of breath/wheezing in 24% of the patients. 17 In a population-based study of 3–5 year old children, asthma was more likely to be reported as a concern by parents of boys who were overweight, had obesity or severe obesity. Boys with severe obesity were more likely to have had wheezing in the past year. 18 There are no published data on the prevalence of obstructive sleep apnea in children aged 2–5 years with severe obesity, or in the resolution of asthma or other respiratory symptoms with weight loss in this age group.
Orthopedic Complications
Orthopedic complications are rarely seen in young children with obesity. In older children and adolescents, obesity has been associated with musculoskeletal discomfort and/or impairment of mobility.25,13 There have been no studies on the prevalence or severity of musculoskeletal disorders in preschool age children with severe obesity.
Behavioral Problems, Developmental Delays, and Other Health Concerns
A population-based study of 3–5 year old children found increased parent reports of headaches and poorer general health among children with severe obesity. 18 Another study found that 28% of parents of 2–5 year old children with severe obesity presenting to a weight management clinic reported behavioral concerns in their children, 17 but only 9% of these children had a confirmed diagnosis of behavioral problems or developmental delay. 17 More studies are needed on behavioral and developmental concerns in young children with severe obesity.
Risk Factors for Early-Onset Severe Obesity
Social, Racial/Ethnic, and Environmental Risk Factors of Severe Obesity
Disparities in obesity prevalence exist among racial/ethnic minorities, 1 by sex, socioeconomic status,1,26 and parental educational attainment. 27 These disparities are also seen among children with severe obesity. Studies have consistently demonstrated a higher prevalence among Hispanic and non-Hispanic black youth,10,28–31 regardless of the criteria used to define severe obesity. A recent analysis of 7028 children aged 2–5 years in the NHANES cohort (1999–2014) 32 reported increasing odds (compared to a referent group of normal-weight peers) of being Hispanic (unadjusted OR 2.3) or Non-Hispanic Black (unadjusted OR 1.7) among children with severe obesity. 32
To date, the data are inconclusive regarding the association between socioeconomic factors among children younger than 5 years and severe obesity, partly because of varying definitions of severe obesity and the relatively low prevalence of severe obesity among 0–5 year old children.10,33,34 However, in a recent analysis of the NHANES data (1999–2014), 32 children aged 2–5 years with severe obesity (compared to normal-weight peers) had greater odds of being from a household that was below the poverty line (unadjusted OR 2.1), headed by a single parent (unadjusted OR 2.0), or characterized by lower educational attainment (unadjusted OR 2.4). These disparities were greater for children with severe obesity compared to children with obesity and highlight the need to better understand and address disparities in this patient population. 32 Further studies are needed to determine the effect of social, racial/ethnic, and environmental risk factors on prevalence of severe obesity in children younger than 5 years.
Timing and Rate of Weight Gain
Impact of weight gain in the first 2 years of life on later obesity
Three critical periods for development of obesity have been identified: gestation, the first 2 years of life, and adiposity rebound (around 5–6 years of age). 35 These periods have been correlated with patterns of weight gain, adult BMI, and risk for obesity. 36 Among children younger than 5 years, the primary focus has been in understanding weight gain in the first 2 years of life and impact on later obesity. A systematic review of 21 studies found a significant positive association between rapid weight gain in the first 2 years of life and increased subsequent risk of obesity. 37 In the Avon Longitudinal cohort study of 848 children, children who demonstrated postnatal catch-up growth within the first 2 years of life had higher levels of BMI and percent body fat by age 5. 38
Examples of rapid weight gain by different metrics
Studies have examined this rapid weight gain in the first 2 years of life using different anthropometric metrics. For example, a gain of greater than 0.67 standard deviation (SD) weight-for-length scores (equivalent to one centile band on the standard growth chart) between birth and 2 years reflects clinically significant catch-up growth, which is normal38,39; however crossing upwards of two or more weight-for-length percentiles in the first 24 months was associated with increased odds of obesity at ages 5 and 10 years, especially if the change occurred in the first 6 months of life as demonstrated in an epidemiological study of 44,622 children. 40 Two other studies, one in 19,397 children and the second in 300 children, defined rapid weight gain as an increase in weight-for-age >1 SD during the first 4 months of life and found this to be associated with an increased risk of overweight status at the age of 7 years and extending into young adulthood.41,42 Finally, in a birth cohort of about 1500 infants born between 1989 and 1990 and followed over 18 years, infants who had “early persistent obesity” gained an average of 6.14 kg (13.5 pounds) between birth and 1 year compared to children with normal trajectories who gained an average of 5.4 kg (11.5 pounds) during the same period.
Figure 1A and B show examples of weight trajectories plotted on CDC 2000 growth curves 4 to illustrate weight trajectories typically seen during infancy and early childhood in children with severe obesity, using two hypothetical patients.
Prenatal Risk Factors
Maternal factors
Systematic reviews have consistently linked maternal weight status, gestational weight gain, and abnormal maternal glucose metabolism to higher birth weight, an identifiable risk factor for early childhood obesity.43–45 High maternal prepregnancy weight is associated with increasing risk for childhood obesity.43,44,46–49 Excessive gestational weight gain (defined by IOM guidelines as 11–40 pounds of total weight gain depending on prepregnancy weight status) 50 and abnormal maternal glucose metabolism have an additive effect on the development of obesity in the offspring of women who have overweight or obesity,49,51–55 while gestational weight gain appears to account for more of the variance in obesity among offspring of women with normal prepregnancy weight status.49,51–53 There are consistent reports of a dose–response relationship between risk for childhood severe obesity and exposure to maternal smoking during pregnancy.43,56,57 There is conflicting evidence on whether timing of smoke exposure during pregnancy affects obesity risk. Many studies suggest an increased risk for obesity among children exposed to maternal smoking during the entire course of a pregnancy.
Epigenetic factors
Animal studies have shown that in utero exposure to inflammation, 58 specific nutrients, 59 high energy diets, 60 and hyperglycemia 61 can alter gene expression for energy regulation and metabolism. However, research is limited in humans.62–67 Emerging evidence suggests that prenatal factors may cause epigenetic changes (i.e., DNA methylation and histone modifications) to the fetal genome in utero, leading to developmental programming that affects offspring energy regulation and metabolism.68,69 These epigenetic changes are occurring at a period of developmental plasticity that may affect the infant's physiologic and metabolic risk for obesity.
Prenatal factors studied in young children with severe obesity
Given that severe obesity in young children has only recently garnered attention, few studies have directly examined prenatal determinants of severe obesity in children <5 years. One study of 6800 children in the Early Childhood Longitudinal Study Birth Cohort identified severe obesity in the mother (aOR 3.4, 95% CI; 1.9–5.8) and maternal gestational diabetes (aOR 2.9, 95% CI; 1.5–5.5) as risk factors for severe obesity in their offspring by the age of 5. 31 Tester et al., in analysis of data of 7028 children from 2–5 years of age in the NHANES database (1999–2014), found that maternal smoking increased the odds for severe obesity (OR 1.9, 95% CI; 1.1–3.3). 32 Another study of 111 children demonstrated a threefold higher prevalence of severe obesity in a group of offspring born to mothers before bariatric surgery compared to a group of offspring born to these same mothers after bariatric surgery. 70 Finally, two studies found differences in gene methylation among 317 young children exposed to different maternal dietary patterns (especially carbohydrate intake) 71 in utero and epigenetic changes of the brain-derived neurotrophic factor (BDNF) promoter gene among children with lower satiety responsiveness and obesity in a cohort of 64 African-American children. 72 This growing evidence suggests that additional studies will be helpful to provide further insight into prenatal risk factors that are potentially modifiable to reduce risk for severe obesity.
Genetic Mutations and Syndromes Associated with Severe Obesity in Early Childhood
Congenital leptin deficiency and specific mutations in the leptin signaling and melanocortin pathway such as pro-opiomelanocortin (POMC) and melanocortin-4 receptor (MC4R), which result in severe obesity, were first identified through case reports in the literature. 73 Pronounced hyperphagia, a complex behavioral condition that involves elements of overeating, lack of satiety, and food-seeking behaviors that cause functional impairment, 74 sometimes as early as infancy is often a primary symptom with these genetic conditions. 73 Children with MC4R mutations have been shown to eat roughly thrice as many calories as their unaffected siblings at an ad libitum meal. 75 To date, the most common monogenic cause of severe early-onset obesity appears to be deficiency or loss of function of the MC4R with an estimated prevalence of 1.8% to 5.8% of children with obesity.75,77 Children with MC4R deficiencies tend to have pronounced linear growth with lean muscle mass, making them notably tall when compared to family members without the defect. 75 Children with POMC mutations characteristically have pale skin, red hair, and symptoms of congenital adrenal insufficiency early in life. 73
Advances in technology-facilitated genome-wide association studies (GWAS) and combination of large cohorts of data have allowed further study into the associations of rare monogenic loci and common gene alleles that are associated with BMI. The FTO (fat mass and obesity associated) locus was the first to be identified as an area of interest from adult cohorts. A study that combined findings from 38,759 participants showed that this single-nucleotide polymorphism (SNP) at rs9939609 is associated with increased odds of obesity among adults, translating roughly to an additional 3 kg of body mass among those with two copies of this common allele. 77 This FTO allele has not been associated with birth weight.77,78 Interestingly, the association between FTO and obesity appears more apparent in older children. In the Twins Early Development Study (TEDS), longitudinal analysis of over 7,000 participants demonstrated an increasing association between FTO and BMI over time, with a heritability of obesity of 0.56 at age 4, which increased to 0.78 by age 11. 79 In the Special Turku Coronary Risk Factor Intervention Project for Children (STRIP) study, where 640 individuals were followed from 7 months of age, having two copies of this FTO allele was associated with 1.67 greater odds of obesity, but only after 7 years of age. 78
Of the 13 genetic loci known to be associated with obesity in adults, significant SNPs have been found for children aged 0 to 18 years in nine loci.
80
Based on these findings
There are several genetic syndromes associated with severe obesity in early childhood. Prader-Willi syndrome (PWS), caused by lack of expression of genes from an imprinted region of the paternally inherited chromosome 15q11–q13, is the most widely recognized syndrome. The prevalence of PWS is between 1/10,000 to 1/30,000. 82 Affected individuals have severe hypotonia with feeding difficulties in infancy. By the age of 2, they often present with hyperphagia, rapid weight gain, obesity, abnormal body composition (decreased muscular mass and increased fat mass), short stature, and behavior problems (food-seeking behaviors such as hiding food, taking food out of the trash can, and stealing food). 82 Treatment for children with PWS involve a reduced-energy diet with balanced macronutrient composition, restricted access to food, and growth hormone therapy. 83
Beckwith–Wiedemann syndrome (BWS) is an overgrowth syndrome occurring in 1 in 13,700 newborns, which is associated with neonatal macrosomia, abdominal wall defects and macroglossia, midface hypoplasia, hemihypertrophy, and embryonal tumors. These children are large newborns and tall children with eventual normal adult height. 84 A case report that identified BWS in two patients (out of 159 with severe obesity) because of genetic screening, who would have been otherwise missed using clinical criteria, suggests that BWS may be underdiagnosed in children with early-onset obesity. 85
ROHHAD syndrome (rapid-onset obesity with hypoventilation, hypothalamic dysfunction, and autonomic dysregulation) is a very rare disease identified in 78 patients to date. Patients with ROHHAD syndrome usually present between 2 and 4 years with hyperphagia and dramatic weight gain, although they are healthy before symptoms appear. Other characteristics of ROHHAD include hypothalamic dysfunction, autonomic dysregulation, adrenocorticotropic hormone deficiency, hypothyroidism, growth hormone deficiency, and alveolar hypoventilation, with early aggressive treatment necessary to prevent cardiorespiratory arrest.86–89
Leptin deficiency or leptin receptor defects are both extremely rare disorders inherited in an autosomal recessive pattern, and have been found in 3% of patients with severe, early-onset obesity. 90 These children typically present with early-onset hyperphagia, rapid weight gain, hypogonadism, and history of increased susceptibility to infection. A history of consanguinity between the parents may be present. Other genetic syndromes to consider include Bardet-Biedl, Albright Hereditary Osteodystrophy, and Fragile-X. These syndromes present with a triad of early-onset severe obesity, dysmorphic features, and intellectual disability. Bardet-Biedl syndrome, caused by a mutation in at least 14 different genes, is associated with visual loss, hypogonadism, polydactyly, and renal problems. Children with Albright Hereditary Osteodystrophy have short stature, round face, subcutaneous ossifications, and pseudohypoparathyroidism. In addition to intellectual disability, for children with Fragile X syndrome, behavioral problems such as autism-spectrum disorder symptoms are often present, along with seizures, an elongated face, prominent ears, and postpubertal macroorchidism in boys.
Medical Risk Factors
In addition to the above risk factors, obesity in infants and toddlers has been associated with exposure to broad-spectrum antibiotics, exposure to antibiotics during the first 6 months of life, steroid use, and diagnoses of asthma and wheezing.91,92 Structural pituitary abnormalities, smaller cerebellar volumes, and impaired general intellectual ability have been demonstrated in a small cohort of children presenting with early-onset severe obesity when compared to normal controls.93,94 However, the effect of these types of structural findings are not yet well understood and more studies are needed to understand the role of exposure to medications and medical problems like asthma and pituitary abnormalities on the development of severe obesity in children younger than 5 years.
Conclusions and Recommendations
Severe obesity in preschoolers is a concern because of the risk of tracking into adulthood, and the higher risk and severity for comorbidities. Young children with severe obesity represent a vulnerable population at high medical risk and therefore need to be identified early and appropriately treated. Sociodemographic factors, prenatal and genetic factors, early weight gain trajectory, and medical risk factors are all important contributors to development of severe obesity among young children. These children can often present with symptoms such as hyperphagia and excessive food-seeking behavior, in combination with developmental delay and physical examination findings such as short stature, abnormal facial features, hypotonia, and hypogonadism. Identifying these risk factors and phenotypical characteristics may be useful for clinical subtyping and early identification of children at risk for severe obesity, and development of effective, targeted, and timely prevention and treatment interventions. A limitation is paucity of existing literature. Further research is required to better characterize this population of young children at high risk for severe obesity.
Footnotes
Acknowledgments
The Expert Exchange Workgroup on Childhood Obesity was supported by the Children's Hospital Association (CHA), Washington, DC, and the American Academy of Pediatrics (AAP) Institute for Healthy Childhood Weight, Elk Grove, IL. Dr. Mirza is supported, in part, with Federal funds (P20MD000198) from the National Institute of Minority Health & Health Disparities. The National Institute of Minority Health & Health Disparities had no role in the preparation, review, or approval of the article. Dr. Phan receives support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number K23HD083439. Dr. Tester receives support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number K23HD075852. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.