
Abstract
Abstract
Objective:
This study examined the effect of pediatric obesity on executive function and reward-related decision-making, cognitive processes that are relevant to obesogenic behaviors, and evaluated their association with sample (e.g., age, gender, intelligence, and socioeconomic status, SES) and study/task (e.g., categorical/continuous variable, food stimuli) characteristics.
Methods:
A random-effects meta-analysis was conducted using Hedge's g effect sizes of published studies from 1960 to 2016, limited to children younger than the age of 21 years without medical comorbidities. Analysis included estimation of heterogeneity (τ2), publication bias (funnel-plot symmetry and fail-safe N), and sensitivity analyses for sample and study/task characteristics.
Results:
Across 68 studies with 70 samples, obesity was associated with worse functioning overall (−0.24; 95CI: −0.30 to −0.19; p < 0.001) and for each component process (attention, switching, inhibition, interference, working memory, reward, delay of gratification: −0.19 to −0.38; p's < 0.017), except trait impulsivity (−0.06; 95CI: −0.18 to 0.07). Deficits increased with age and female composition of the sample for inhibition (p = 0.002). No other characteristics moderated effect of obesity.
Conclusions:
Small-to-moderate negative associations with obesity were observed for executive and reward-related performance, but not on reported impulsivity in studies with children younger than the age of 21 years. These results were not moderated by IQ, SES, and study/task characteristics. Age and gender moderated association with inhibition, with a larger obesity-related deficit in older and predominantly female samples. These results suggest cognitive and demographic intervention targets for prevention and mitigation of obesogenic behavior.
The pediatric obesity epidemic began over 15 years ago, 1 with over 20% of adolescents and 17.5% of children currently obese in the United States (body mass index—BMI—above the 95th percentile). 2 In addition to increased risk for medical and psychopathological comorbidities during childhood 3 and later in adulthood,4,5 pediatric obesity is associated with worse social, 6 cognitive, 7 and academic outcomes.6,8 Models of obesity point to the centrality of executive and reward-related processes that may serve to promote and maintain obesity through their influence on obesogenic behavior (e.g., consumption of energy dense foods).9,10 In light of the growing literature examining these cognitive functions in pediatric obesity, we conducted a meta-analysis with the goals of drawing definitive conclusions about their status in children with obesity and moderating sociodemographic factors (e.g., socioeconomic status—SES, age, gender).
Executive function subsumes voluntary regulatory processes that enable flexible goal-directed behavior, which in conjunction with reward processing guides decision-making. 11 The meta-analysis takes a cognitive neuroscience perspective, which posits that a set of general-purpose control processes enabled by the prefrontal cortex serve to regulate complex cognition. 12 Three control processes have been revealed by latent variable analysis 13 : (a) attending to and holding contextually appropriate stimuli and responses in mind temporarily (indexed by assessments of attention and working memory); (b) inhibiting inappropriate responses (indexed by tasks of inhibition and interference and questionnaires of impulsive traits), and (c) flexibly shifting responses as context changes (indexed by assessments of cognitive flexibility or shifting). These control processes interact with implicit and explicit reward processes associated with affect (i.e., hedonic value or “liking”), learning of reward contingencies, and motivation (i.e., “wanting”) 14 in the context of decision-making. The behavioral outcomes of reward-related decision-making are typically measured by delay of gratification and delayed discounting tasks manipulating rewards. These tasks require the integration of control and reward-related processes subserved by connections of the prefrontal cortex with striatal regions. 15 Guided by this conceptual framework, our literature search included the italicized terms.
Executive and reward function is associated with both the promotion and maintenance of obesity by influencing both healthy and obesogenic behaviors.9,10 Better inhibitory control has been associated with increased likelihood of completing a planned physical activity or healthy food choice in adults 16 and was associated with more fruit/vegetable intake and engagement in physical activity in children. 17 Children with better executive function at the end of elementary school were also more likely to maintain a lean body weight at end of junior high. 18 Conversely, poor executive abilities in children have been associated with greater snack food intake and sedentary behavior 17 and increased risk for maladaptive food behavior (e.g., emotional overeating), 19 while increased reward sensitivity in children has been associated with greater intake of fast food and sweetened beverages. 20 In addition, worse delay of gratification and self-regulation in early childhood (2 and 4 years) were associated with higher BMIs in later childhood, 21 preadolescence, 22 and adulthood. 23 Prevention and intervention efforts would be served by knowing the magnitude of executive and reward-related decision-making deficits in children and adolescents with obesity and whether these deficits are moderated by sociodemographic factors.
The effect of obesity on executive function appears to be moderated by a variety of demographic factors. Variability in general intelligence, as measured by IQ, and SES are independently associated with risk for pediatric obesity 24 and executive dysfunction25–27 and, therefore, have the potential to attenuate or augment the association between obesity and executive deficits. In addition, it is possible that the effect of obesity on executive function changes across development with adolescence representing a particularly vulnerable period of development because the maturation of executive control lags behind gains in reward sensitivity. 28 Thus, obesity may further compromise executive abilities during adolescence, leading to a larger adverse effect of obesity on executive functioning in adolescents than in younger children. Understanding the moderating influence of developmental and demographic factors on the effect of obesity is necessary for identifying who is at risk.
The present study aims to comprehensively quantify the magnitude of impairment in executive and reward function in pediatric obesity by conducting a meta-analysis of studies published through December 2016 that examined those cognitive functions in children younger than the age of 21 years without other health comorbidities. Since the previously published meta-analysis 29 (inclusion July 2012) focusing on impulsivity in pediatric obesity (i.e., inhibitory control and reward-related decision-making), there have been more than twice as many additional studies that have been published. The present study examines whether their observed pattern of obesity-related deficits for inhibition and reward-related decision-making 29 are replicated and extend to other control processes (e.g., cognitive flexibility, working memory). In addition, we examined the effect of important moderators through sensitivity analyses, including sociodemographic factors (e.g., age and gender, SES), IQ, and study-design characteristics. Together, we sought to provide a comprehensive view of the status of executive and reward function in pediatric obesity.
Methods
This study followed the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 30
Literature Search
Our search used PubMed (from 1960 to 2016), PsychInfo (from 1978 to 2016), and Academic Search Premier (from 1975 to 2016) and included following search terms attention, executive function, cognitive control, inhibition, working memory, switching, cognitive flexibility, impulsivity, delayed discounting, reward, and delay of gratification in conjunction with obesity, obese, body mass index, overweight, weight, and adiposity. Search terms for cognitive functioning were derived from common terminology related to executive and reward processes in addition to the tasks used to assess them (examples of search terms are italicized in Introduction). The search used the limits youth, adolescents, child/children, pediatric, and human and yielded 9677 unique studies. Figure 1 presents a graphic of the decision process (Supplementary Data for an example of the electronic search strategy; Supplementary Data are available online at www.liebertpub.com/chi).
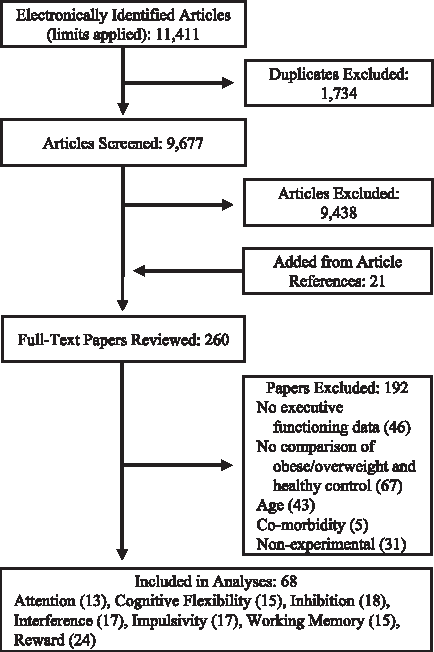
Flowchart depicting results and method the systematic review.
Titles of studies were screened according to the following exclusion criteria: (a) not written or translated to English; (b) participant older than the age of 21years; (c) inclusion of participants with genetic syndrome associated with obesity; (d) inclusion of participants diagnosed with psychopathological disorder (e.g., eating disorder or anxiety) or medical comorbidity (e.g., metabolic syndrome or type II diabetes); and (e) report of only latent variable for executive/reward function. Full texts were reviewed for both the exclusion criteria and the following inclusion criteria: (a) empirical study; (b) participant sample included both participants with healthy weight (>5% BMI percentile <85%) and overweight/obesity (BMI percentile ≥85%); and (c) executive or reward functioning and adiposity were assessed concurrently. A total of 68 studies met criteria for inclusion, many of which assessed multiple processes of executive and reward function (Table 1).
Study Characteristics
Value in parentheses after adiposity measure indicate cutoff used to identify overweight/obesity. Leading numbers indicate reference number.
Studies included in SES model.
Studies included in IQ model.
Studies also included in Thamotharan et al. (2013).
Measures combined to create an aggregated effect.
Interference score calculated by hand (incongruent scores - congruent scores).
Included in search as a study under submission and was later published.
BMI, body mass index; BMI.p, percentile; BMI.z, Z-score; BMI SDS, standardized; IOTF, International Obesity Task Force cutoffs used; Triceps, triceps skin-fold thickness; OW.p, percent overweight.
Coding and Data Extraction
All studies were coded by authors AP and CL with disagreements or errors resolved through discussion.
Data extraction
See Supplementary Data for description of study reported statistics. In the event that obese and overweight groups were reported separately, pooled means and standard deviations were used to create a single overweight/obese group. Effects were categorized into one of seven cognitive process: (a) Attention: performance on sustained attention tasks resulting in individual (e.g., Continuous Performance Test) or composite scores (e.g., Kauffman Attention Factor); (b) Cognitive Flexibility/Switching: performance-based measures of verbal fluency, perseveration (e.g., Wisconsin Card Sorting Task), and switching (e.g., Trail-Making Test B); (c) Inhibition: performance on response inhibition (e.g., Go-No/Go, Stop Signal Task); (d) Interference: performance on interference tasks (e.g., Flanker, Stroop); (e) Trait Impulsivity: parental or self-report questionnaires assessing everyday impulsivity (e.g., UPPS-P Impulsive Behavior Scale or Behavioral Activation Scale)–while these behaviors reflect inhibitory and reward function, they were separated due to evidence for the independence of impulsive traits from actions (i.e., inhibition) and choices (i.e., reward) 31 ; (f) Working Memory: performance on working memory tasks (e.g., span tasks, N-back task); (g) Reward: performance on delay discounting, delay of gratification, and reward-related risk taking tasks (e.g., Door Opening Task); (h) Other: tasks related to planning (e.g., Tower of London) or assessments of general executive functioning (e.g., Woodcock–Johnson Executive Processing). For study and task details see Table 1.
Data Analysis
All data analyses were completed using R.
32
Study results were converted to Hedge's g,
33
with negative effects indicating worse performance in the obese/overweight group or with greater adiposity. Random effect models, using a restricted maximum likelihood estimator and inverse variance weights, were used to estimate the effect of obesity on executive and reward function overall and for each component processes model.
34
Although Cochrane's Q and the I2 statistic are commonly used to classify heterogeneity, both have been shown to increase with the number and size of studies in the model.35,36 Therefore, this study used predication intervals, which estimate the variability of the true effect of obesity,37,38 to estimate heterogeneity because they are calculated from
Sensitivity analyses used mixed effects metaregression models for the following characteristics: (a) Mean age of the sample; (b) Gender composition of the sample (percent male); (c) the effect of adiposity on IQ (Hedge's g estimate); and (d) the effect of adiposity on SES (Hedge's g estimate); (e) Study Design, which was coded as continuous for studies assessing correlation with adiposity and categorical for studies assessing adiposity through group differences; (f) Experimental Assessments, which was included when clusters of studies used the same or similar tasks and was included for Cognitive Flexibility/Switching, Inhibition, Interference, Working Memory, and Reward-Related Decision-Making models; and (g) Food Stimuli, which was included for Delay of Gratification tasks that characterized the delayed rewards as food versus nonfood.
Results
A total of 70 unique samples, extracted from 68 studies, were used in these analyses. Twenty of the 68 studies were also included by the previous meta-analysis, 29 while three studies included in that article were excluded due to meeting our exclusion criteria (report of only latent variables, medical comorbidities, or existing conditions). The number of effects sizes extracted from each study ranged from 1 to 14, while study samples sizes ranged from 20 to 9415 participants (Table 2).
Model Characteristics
The Overall model contains all executive process and reward models in addition to studies falling in the Other category (Studies = 6; Participants = 3323).
Total sample size for models counts multiple measures from same study separately.
Random Intercept Models
IQ and SES
A total of 15 (22%) and 25 (37%) studies reported data on intelligence and SES, respectively (Table 3). Adiposity had a significant small negative effect for IQ and SES. Both models showed wide prediction intervals indicating nontrivial heterogeneity, likely due to differences in measurement across studies. There was no funnel plot asymmetry and both models showed the FSN's above the cutoff for high tolerance of unpublished null findings. Together, these findings indicate that greater adiposity was associated with lower intelligence and lower SES, however, the prediction interval indicates that the true effect varies substantially.
Model Results
p < 0.05.
p < 0.01.
p < 0.001.
CI, confidence interval; FSN, Fail-Safe N; PI, prediction interval.
Overall and component process models
There was a significant small negative effect of obesity in the Overall model, indicating worse functioning in children and adolescents with obesity, regardless of component process. Given the wide prediction interval, significant funnel plot asymmetry may not reflect true publication bias but rather systematic heterogeneity across studies, such as cognitive process assessed. The FSN far exceeded the cutoff, indicating that the model was robust to potential unpublished or null findings.
In light of evidence for heterogeneity of effects associated with obesity, separate models were used to assess each cognitive process. Given too few studies, the “Other” category was not examined in a separate model. All processes except Trait Impulsivity showed small negative effects of adiposity, indicating that greater adiposity was associated with worse functioning. Thus, Trait Impulsivity was not included in further analyses. Prediction intervals for Attention, Cognitive Flexibility/Switching, and Inhibition show a distribution of true effects that range from large/moderate negative effects of obesity to negligible positive effects. Interference, Reward-Related Decision-Making, and Working Memory, however, had prediction intervals that extended into small/moderate positive effects. Attention, Cognitive Flexibility/Switching, Inhibition, Working Memory, and Reward-Related Decision-Making all showed evidence of funnel plot asymmetry, however, heterogeneity seen in the predication intervals indicate that there may be study-level differences driving the asymmetry. The majority of the models were robust to potentially unknown null data with only Working Memory and Delay of Gratification showing FSN values that did not meet the cutoff, indicating that new or unpublished null results may affect the strength of the effect of adiposity on those processes. In sum, these models provide evidence for three important findings: first, pediatric obesity is associated with an overall deficit; second, pediatric obesity has a significant negative effect on all component processes except Trait Impulsivity; and third, the prediction intervals indicate that although the effect of pediatric obesity was negative, there may be important differences across studies that influence this effect.
Sensitivity Analyses
Sociodemographic, study design, and experimental assessment characteristics were independently examined to determine whether they moderated the observed significant negative effects of obesity (Table 4).
Sensitivity Results
p < 0.10.
p < 0.05.
p < 0.01.
p < 0.001.
Reference level is continuous.
Reference level is no food stimuli.
Attention
A marginally significant effect of Age indicated that higher mean sample age was associated with more negative effects of adiposity (Fig. 2A). Thus, deficits in attention increased for samples with older children with obesity. No other moderators were significant.

These plots depict significant moderators of the effect of obesity on executive abilities with the moderator Age shown in A and B, sample composition in C, Task Type in D, and Study Design in E. The size of the points on the graphs relate to the contribution or weight of that study in the model. The dotted lines reflect predicted marginal effects with 95% confidence intervals.
Inhibition
A significant effect of Age indicated that higher mean sample age was associated with more negative effects of adiposity (Fig. 2B). In addition, a significant effect of Gender indicated that a higher composition of males in a sample was associated with less negative effects of adiposity (Fig. 2C). Although Study Design was not significant, there was an effect of Experimental Assessment (Qmoderator (2) = 37.27, p < 0.001). Studies assessing response inhibition with performance measures (Go/No-Go task: n = 5; β = −0.32, SE = 0.08, p < 0.001 and stop signal task: n = 10; β = −0.47, SE = 0.08, p < 0.001; no difference between tasks, p = 0.129) showed greater negative effects than questionnaire-based assessments (Fig. 2D). Together, these results indicate that older children and females were more vulnerable to the negative effects of obesity and that task performance was more sensitive to the effect of obesity on inhibition than behavioral reports. No other moderators were significant.
Working memory
A significant effect of Study Design indicated that using a categorical rather than a continuous study design resulted in larger negative effects (Fig. 2E). No other moderators were significant, including differences in Experimental Assessments (span-based versus other tasks; p = 0.158).
Remaining models
No moderators were significant for Cognitive Flexibility/Switching, Interference, Reward-Related Decision-Making, or Delay of Gratification models. Similarly, there were no differences between Experimental Assessments in models for Cognitive Flexibility/Switching (trail-making test versus fluency or questionnaire measures; p = 0.102), Interference (Stroop versus Flanker or Simon tasks versus other tasks; p = 0.690), nor Reward-Related Decision-Making (delay of gratification versus risk-taking tasks versus delay discounting; p = 0.147). In addition, there was no effect of Food Stimuli for Delay of Gratification (p = 0.411), indicating that food rewards did not impact Reward-Related Decision-Making differently from nonfood rewards.
Discussion
Small-to-moderate impairments were associated with pediatric obesity for executive and reward-related performance but not trait impulsivity, with larger inhibitory deficits in older and predominantly female samples. Although obesity was associated with lower IQ and SES, these variables did not moderate the observed effects. Together, these findings replicate those of the previous meta-analysis 29 and extend the scope of the negative effects of obesity to include additional executive processes and potential moderators. Our results suggest cognitive and demographic targets for intervention and prevention of obesity.
The present findings provide a comprehensive view of the current status of executive and reward deficits in pediatric obesity. Our findings replicate inhibitory and reward-related decision-making deficits in pediatric obesity, but found no evidence for differences for parental/self-report measures of impulsivity. This indicates that obesity was associated with more impulsive actions and decisions, but not impulsive personality traits. 31 Beyond replication, our findings showed working memory and cognitive flexibility/shifting deficits associated with obesity. In addition, the present study showed attention deficits associated with obesity while the previous meta-anlysis 29 did not, perhaps due to increased power after including the seven studies published since 2012. Despite replication, the present effect sizes were slightly smaller than those reported previously, 29 potentially due to the inclusion of double the number of included studies, studies examining a wider range of executive functions, or the strict exclusion of samples with medical comorbidities. Nevertheless, largely consistent findings across these two meta-analyses underscore the stability of deficits for inhibitory and reward function and, therefore, their importance in mediating behaviors that promote obesity in children and adolescents.
Sensitivity analysis revealed age and gender as important moderators of the strength of the associations between obesity and executive and reward functioning, which has implications for intervention or prevention efforts. The performance gap between children with and without obesity was larger for older than younger children on inhibition tasks and marginally so for attention tasks. Developmental models have identified adolescence as a vulnerable period for reward-related decision-making due to the development of reward functioning outpacing the maturation of executive function. 43 Such a model predicts that adolescents ought to show a greater adverse effect of obesity on reward-related decision-making, which requires the interaction of executive and reward functioning. Contrary to this prediction, the effect of obesity on reward-related decision-making was not significantly moderated by sample age. Perhaps the dissociable effects of sample age on executive and reward-related function relate to differences in the sensitivity of measures or lack of controls for cognitive load or difficulty. They may also reflect a true dissociation in the effect of obesity on executive and reward processes, a ripe area for examination with experimental studies in the future. Nevertheless, it is notable that prevalence of severe obesity (BMI 120% above the 95th percentile) increases from 1.7% in young children to 8.7% in adolescence 2 and is associated with increased likelihood of experiencing multiple medical complications 44 and decreased quality of life relative to overweight and obese peers. 45 Disproportionately more severely obese children in adolescent samples may intensify the negative effect of adiposity, and therefore, adolescence should be more closely examined for identification of cognitive dysfunction and possible intervention efforts.
Gender moderated effects of obesity such that inhibitory deficits were larger in samples with a greater percentage of females. Although rates of pediatric obesity do not differ by gender, 2 worse quality of life due to health comorbidities and depression is seen at higher rates in females than males with obesity.46,47 These differences may result in worse response inhibition for girls with obesity as depression can lead to worse executive functioning, 48 however, one would also expect that higher rates of depression in females would also negatively affect reward functioning. In adults and adolescents, neural engagement during response inhibition has been seen to differ by gender with greater engagement of frontal-striatal regions in females and greater activation in parietal and motor regions in males. 49 Thus, it is possible that those brain-based gender differences underlie the observed moderation of the effect of obesity on response inhibition by gender. Thus, females should be targeted for early intervention and prevention efforts.
Caution is warranted in interpreting the present findings in light of two observations: first, there are sources of heterogeneity that cannot be controlled. Although statistically significant, some models were not robust against potential unpublished or unknown findings (e.g., Working Memory) and prediction intervals indicated substantial heterogeneity in the distribution of true effects ranging from moderate–large negative effects to small positive effects (e.g., Interference, Reward-Related Decision-Making, and Working Memory). Furthermore, cognitive load/task difficulty is an important source of heterogeneity for executive function. For example, cognitive load differs by the proportion of congruent to incongruent trials on Interference tasks and by the requirement to dynamically update what is maintained in working memory.50–52 Such features of study design could not be controlled because they were either not reported or manipulated in few studies.
Second, sociodemographic, study design, and experimental assessment moderators failed to explain heterogeneity for most component processes (except inhibition and attention), which may be due to measurement limitations. Greater adiposity was associated with lower IQ and SES, which is consistent with previous reviews, 24 however, they did not moderate association with obesity for executive and reward functioning. The large prediction intervals for these variables indicate substantial heterogeneity in the size of the true effect. Although assessment of IQ is standardized, the construct of SES is not and was assessed differently across studies, potentially contributing to the observed heterogeneity. Only a relatively small proportion of studies reported IQ or SES data, which also may have resulted in reduced power to identify moderation. Furthermore, the failure of included moderators to explain variability across studies highlights a need to include more fine-grained measurement of demographic variables (e.g., race and ethnicity) in future studies so that possible correlates of both obesity and executive functioning can be identified.
In sum, the present results provide a comprehensive view of the status of executive and reward-related functioning in pediatric obesity, which should motivate future experimental work. In addition, we identified potential moderators that should be further examined in prospective studies, to target intervention and prevention efforts. Whether the observed impairment is a cause or consequence of obesity cannot be discerned by the present results. Structural and functional neural differences in the prefrontal cortex, which subserves control processes, 12 and in fronto-striatal regions, which subserve reward related decision-making, 15 are observed between children with and without obesity, however, whether these differences lead to behaviors that promote obesity or are caused by obesity is yet unknown. Some mechanistic insight is provided by our preliminary findings showing a reversal of behavioral and functional neural differences in frontal-striatal regions following weight-loss surgery, 53 suggesting that adiposity has deleterious effects on neural function. Which metabolic factors may drive the observed plasticity remains to be examined in the future.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.