
Abstract
Abstract
Food addiction has become a popular notion in the media and scientific community, with many proposing that an addiction to food causes obesity. An article published in this journal in December 2017 by Tompkins et al. asserted that food addiction poses a barrier to the treatment of adolescent obesity. This review questions some of the methods, results, and perspectives offered by Tompkins et al. It also considers the extant evidence overall about this construct. The data about food addiction provide minimal support for the discriminant validity of this conceptualization relative to depressed binge eating. We believe that the evidence suggests that the potential harm outweighs the benefits of encouraging researchers, clinicians, and especially obese people to view food addiction as a cause of obesity or a barrier to effective weight management. Ultimately, this review concludes that the construct of food addiction does not serve the interests of those striving to lose weight permanently (i.e., weight controllers) nearly as well as an alternative perspective: weight controllers are athletes, not food addicts.
In the December 2017 issue of Childhood Obesity, Tompkins et al. 1 published a well-written article on the results of a detailed multiyear evaluation in their clinic at the University of Vermont. The authors clearly advocated for viewing food addiction as harmful to weight management, as reflected in both their title, “Food Addiction: A Barrier to Treatment for Obese Adolescents,” and their concluding comment, “Our study suggests that food addiction is a significant barrier to successful weight management for obese youth (p.468).”
Directly contrary to Tompkins et al.'s viewpoint, prior publications on this topic over the past two decades, including concluding comments from the editors and author of all three books published on it to date,2–4 either questioned the validity of the construct5–7 and/or argued for its potentially negative impact on weight controllers.4,8 For example, the editors of the most comprehensive book ever written on this topic, Drs. Mark Gold (a psychiatrist who has clearly favored the food addiction concept based on prior publications and the first author's personal experiences with him) and Kelly Brownell, concluded at the end of their 462-page book entitled, Food and Addiction, “Relatively small numbers of people might merit the label “food addict;” thus, intervention can be seen as helping those in need but not having a public health impact on large populations.” p. 439. 3
This article will show that the results of Tompkins et al.'s study, although undoubtedly well-intentioned, does not provide any meaningful support for the validity of the food addiction construct. We will examine notable flaws in the design, reveal a major statistical error, and discuss the perspectives in Tompkins et al., as well as recap why we favor conceptualizing weight control as an athletic challenge,3,8 instead of a quest to overcome food addiction.
Tompkins et al.
In a 2–3 year period at their clinic, Tompkins et al. 1 provided a 12-week intervention to 26 adolescents and at least one of their parents. The program consisted of physical activity (exercise sessions), as well as nutritional/behavioral instruction, delivered in small groups (at least five adolescents in each group, sometimes with and sometimes without parents in attendance). Extensive preassessments and postassessments included food addiction, weight/height (objectively measured), and quality of life, all completed just by the teenagers, not the parents.
Design Flaws
Treatment
When testing the impact of any factor on treatment, it seems imperative to provide an intervention that has an excellent chance of actually treating the problem. In two versions of a review published in 20139,10 on the treatment of obesity in children and adolescents, the first author and his colleague, Dr. Kristen Geirut, analyzed the recommendations of five expert groups. All five expert groups agreed that cognitive behavior therapy (CBT) was a key element of effective treatments of obesity. Also, two of these expert groups indicated that behavioral/nutritional instruction alone without such a CBT therapeutic intervention produced minimal results. For example, Wilfley et al.'s 2007 meta-analysis 11 explicitly tested the impact of instruction vs. waiting list controls. They found that instruction produced no benefits compared to the controls (see, also, a related meta-analysis of 46 long-term educational interventions by Stice et al. 12 ).
In another testimony to the inadequacy of instruction alone, Saelens et al. 13 randomly assigned overweight and obese adolescents to either an intervention group or a comparison group. The comparison group received one educational session; they became significantly more overweight 4 months later. The intervention group completed an elaborate computerized assessment and received an educational session to review an explicit plan for change; a detailed treatment manual; a family consultation; and 11 telephone counseling sessions. The intervention group did not lose weight initially or at a 3-month follow-up. If this elaborate educational intervention proved so ineffective with overweight teens, could we really expect other educational interventions to work?
In sharp contrast to education alone, CBT involves focusing first on forming positive supportive relationships with clients; then, within this therapeutic relationship, therapists and clients collectively pursue goal setting, planning, problem-solving, maximizing commitment, reducing stress, and facilitating consistent self-monitoring. CBT also gets administered or at least supervised by licensed behavioral health specialists, in part, to assess clinical issues, to ensure that strong positive relationships develop, and to focus on the more emotional aspects of making major life changes. Two of the expert groups also stressed the empirically demonstrated value of using intensive CBT, defined by the well-respected U.S. Preventive Services Task Force 14 as consisting of at least 25 sessions, based on the impressive results for such programs.11,15
The first author explicitly asked, through email, Tompkins et al. to describe who ran and supervised their groups and if they included CBT (i.e., an emphasis on explicit goals for self-monitoring, calories and fat). The corresponding author indicated that the program they provided did not include any licensed behavioral health providers. The corresponding author did not respond when questioned repeatedly through email about explicit goal setting and self-monitoring, that is, CBT (and their published article did not describe any such goals or CBT-related approach). This analysis indicates that the Tompkins et al.'s study provided a treatment that seemed very unlikely to treat obesity effectively. 16
So, Tompkins et al.'s 12-week exercise/educational intervention probably did not include CBT or any other scientifically based clinical approach to treating obesity (or decreasing binge eating or psychological distress). The program offered less than half the number of sessions recommended as a minimum for intensive CBT, the treatment of choice, and participants only attended about 58% of those sessions (on average), making the intensity of treatment about 28% of the recommended minimum. The emphasis on exercise and nutritional/instruction vs. CBT without having appropriate supervision and training in CBT may well have contributed to the high attrition rate observed (50%). The authors asserted that such attrition was common for weight-loss interventions for adolescents/families, but most published studies reported less than half of that rate.11,15,17
Convergent vs. discriminant validity
Another major design flaw was the focus on correlates of a measure of food addiction (e.g., quality of life and appetite—convergent validity) rather than testing the discriminant validity of food addiction relative to psychological distress and binge eating.18,19 In other words, the results of several prior studies and reviews have argued that the current measures of food addiction may actually only measure psychological distress and binge eating, in accord with some of the points the authors noted in their discussion section. Quite a few studies in recent decades have already demonstrated that psychological distress and binge eating can create barriers to effectiveness of treatment of obesity, in both adults20–23 and adolescents.24–27 For example, Figure 1 shows the results of a study completed on campers who attended a large CBT-based immersion program.28,29 The results revealed dramatic differences in campers identified before the start of camp as more distressed in various ways (“Red Flagged”) vs. nonflagged campers in percentages sent home prematurely (i.e., forced attrition, 26).
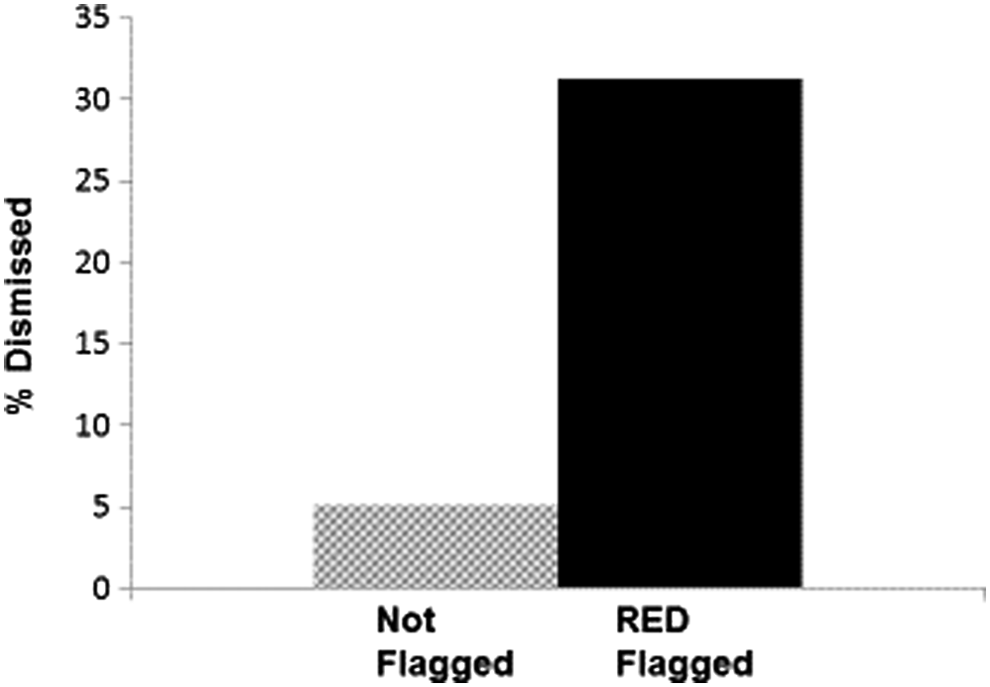
Percentages of participants in Wellspring Camps dismissed based on their Red Flag statuses before the beginning of camp. Based on data in Kirschenbaum et al. 26
Tompkins et al. 1 actually cited a study, Burmeister et al., 30 which testifies to the possibility that measures of food addiction may overlap tremendously with the much simpler construct of binge eating, a very different and less pathologically oriented construct. Unfortunately, the authors actually used that citation inaccurately; they asserted, “Studies in obese adult populations demonstrate that individuals with food addiction and a greater number of food addiction symptoms are less successful when enrolled in traditional weight loss programs 19 ”—that is, only citing Burmeister et al., referenced in this article. 30 Burmeister et al. 30 actually did not find evidence for the discriminant validity of the food addiction construct as a barrier to treatment. Burmeister et al. 30 evaluated 57 obese adults using the Yale Food Addiction Scale (YFAS). 31 Burmeister et al.'s 30 adults attempted to lose weight for just 7 weeks and were not evaluated beyond that. YFSA scores correlated to a low, but significant (one tailed) extent (accounting for 4.8% of the variance in reduction in body weight lost); however, the addiction measure did not predict outcomes any better than a simple measure of binge eating (also accounting for 4.8% of weight loss). When tested directly to see if food addiction accounted for any more variance in weight loss than binge eating in a regression analysis, Burmeister et al. 30 found that it did not. In other words, to a very small extent, some binge eaters did not lose as much weight as nonbinge eaters in this small study, but the YFAS scores [essentially perhaps just another measure of binge eating+distress] revealed nothing more than that. In another study cited by the authors Lent, Eichen, Goldbacher, Wadden, and Foster 32 emphasized this point about the Baumeister et al.'s findings by stating, “…FA [“food addiction”] symptomatology models were not significant when they also included binge eating (p.52).”
In that same Lent et al.'s 32 study, these researchers included, relative to Burmesiter et al., more than three times as many overweight and obese adults (n = 178) evaluated over an almost four times longer period of time (6 months). Based on their support for the food addiction concept, the authors expected their food addicts to struggle significantly more than the nonaddicts to stay involved in their CBT program and lose weight. That did not happen, once again something not mentioned by Tompkins et al. 1 The ostensible food addicts attended just as many sessions and lost just as much weight as the nonaddicts.
Finally, another study cited by the authors Pepino, Stein, Eagon, and Klein 33 examined the effects of bariatric surgery on those classified by the YFAS as food addicts vs. nonfood addicts. They found that symptoms of food addiction decreased dramatically by 9 months postsurgery for 93% of their participants. However, something not mentioned by the authors and yet most relevant to this article, Pepino et al. 33 also found that their food addicts lost just as much weight as their nonaddicts.
Why call something food addiction if it really just shows the same thing we have known for many years: psychological distress and binge eating can negatively impact the treatment of obesity? Asserting the validity of essentially a new name (food addiction) for old concepts (psychological distress+binge eating) can provide misleading direction for treatment, as well as cluttering the field with unnecessary constructs; as such, substituting food addiction for distressed binge eating may well be antithetical to the scientific ideals of parsimony and conceptual integration.18,19,34 As we will discuss in the next major section of this article, food addiction has implications that seem notably more detrimental to weight controllers than distressed binge eating—especially relative to a newer and more positive concept: weight controller athlete.
Sample Size
In their Discussion section, Tompkins et al. clearly acknowledge that their sample was too small (especially after the 50% attrition) to afford meaningful generalizability. This lack of generalizability is especially troubling given the author's stated purpose “…to explore the prevalence of food addiction and correlates of food addiction symptoms…” In addition to the lack of generalizability, the study lacks efforts to mitigate the limitations of a small sample. Before Tompkins et al. completed this evaluation, why did they not perform a power analysis or review other related evaluations to realize that an adequate sample size to detect differences in two groups of obese teenagers would be much larger than their initial sample size?
Wilfley et al.'s 11 meta-analysis showed an average sample size of 35 (vs. Tompkins et al.'s 26 ). Had the authors conducted an a priori power analysis, 35 they would have concluded that their t-tests required a sample of at least n = 128 participants (n = 64 participants in each group), assuming a medium effect size of d = 0.50, and n = 52 participants (n = 26 each group), assuming a large effect size of d = 0.80. This is the result of a power analysis for independent mean comparison using power tables (Table 2 in 35) with the conventional desired power of 0.80, an assumed effect size, and the standard α = 0.05. Even assuming the large effect size, the sample size requirement would have been double their initial sample size (n = 52 instead of n = 26) and quadruple their sample size after attrition (n = 13). The group classified as food addicted actually had n = 8 at baseline and n = 3 post-participation.
These power estimates are generous in assuming large effect sizes, which would not be likely given past meta-analytic results that revealed such relatively brief educationally oriented interventions often have smaller effects.11,12 Of course, the authors did find significant results that typically allow the assumption of adequate power. With the observed effect sizes, the sample size was adequate to detect a significant effect for several analyses. The authors actually found unusually large effect sizes, such as “Attendance with the weight management program was significantly lower in the adolescents identified as food addicted compared to the nonfood addicted (4.5 ± 2.3 vs. 8.0 ± 3.4, p < 0.05) (p.465).” This analysis reveals an effect size of d = 1.21, much larger than what is traditionally considered a large effect in the social sciences. 35 However, all statistical analyses, as well as effect size estimates and power analyses, include certain statistical assumptions. As is the case for most studies that use these analyses, these authors also reported no tests of statistical assumptions such as the normality of the distributions of the continuous variables. In this particular case, however, it seems possible, maybe probable, that the authors' unusually large effect sizes may not have been the result of real effects; instead, skew or unequal variance that commonly occur in such small groups (e.g., n = 8 food addicts) may have contributed substantially to such effects.
The current well-accepted gold standard for assessing treatment efficacy for obesity includes using intent to treat analyses 36 and a 1-year follow-up. 11 Tompkins et al. did not do intent to treat analyses or any follow-up. Also, the program itself did not produce clinically meaningful outcomes, as would be expected based on the nature of its design and high attrition rate. Even when examining the data obtained for active participants, on average adolescents' weight and BMIs stayed the same from pretreatment to posttreatment—just 12 weeks later. The slight decrease in ZBMI (BMI z-scores) gets even slighter when incorporating the projected no change in ZBMI from the dropouts. Prior research actually suggests that dropouts generally fare significantly worse than participants before dropping out, 37 making it conservative to project them as maintaining their weight at the same level from baseline to posttreatment. 11 Comparing mean ZBMIs pretreatment to posttreatment for participants may have eliminated the significance of the reported 2.06 ZBMI pretreatment to 1.99 posttreatment (no dropouts) vs. 2.06 pretreatment to ∼2.03 posttreatment (with dropouts). Translating the latter ZBMIs to % overweight would result in approximately (and quite possibly nonsignificant) 64.75% overweight pretreatment to 62.3% overweight posttreatment (−2.5%).
Wilfley et al.'s meta-analysis that included eight randomized controlled trials (RCTs) that used %overweight metrics showed an average reduction posttreatment more than three times that level: −8.2% and even better than that (−8.9%) at follow-up. Even these relatively favorable results were described by Wilfley et al. as “modest weight changes.” In studies of CBT plus immersion treatments, 17 average reduction in % overweight from pretreatment to follow-up (without intent to treat analyses, however) was 12 times the impact of Tompkins et al.'s results: −29.9%.
Major Statistical Error
Tompkins et al. based their assertion of the possible harmful effects of food addiction on treatment of adolescent obesity on one major finding: significantly higher attrition of the eight food-addicted participants (5/8 dropped out, 62.5%) vs. 8/18 (44.4%) dropouts of the nonaddicted participants, stating “…attrition was significantly higher in those identified as food addicted compared to the adolescents who did not meet criteria for food addiction (62.5% vs. 44.4%, p < 0.05),” p.465. The authors highlighted this finding in their abstract, discussion, and conclusions.
Although the authors clearly state their analysis plan for the majority of their tests, they do not indicate which statistical test they used to analyze differences in attrition between those meeting and not meeting criteria for food addiction. Presumably, a chi-square analysis was utilized as is appropriate for a categorical IV (meeting criteria for food addiction yes/no) and attrition (remained in study until the end, yes/no). Conducting this chi-square analysis does not reveal a statistically significant effect as the authors reported. Instead, it reveals no significant relationship between food addiction and attrition, χ2 (1, n = 13) = 0.722, p = 0.395.
Given that we do not know exactly how these data were analyzed, perhaps the authors conducted another test, possibly explaining the error. The authors may have performed a Z-test, a common test for two proportions. This would not be as appropriate given the small sample size, but it is a common analysis strategy. However, a Z-test of those proportions does not come close to achieving statistical significance. Comparing 62.4% attrition by the food-addicted participants (n = 8) to 44.4% attrition by the nonaddicted participants (n = 18) yields a Z-test value of 0.85, p = 0.395, two tailed (p = 0.20, one tailed).
This glaring statistical error negates a major finding in the study as well as the conclusion. Certainly, attendance at CBT programs does make a major difference in outcomes, 38 with dropouts generally showing poorer results before they discontinue than those who remain in treatment longer. 37 By dropping out, they also approximate the impact of information-only comparison groups, something that rarely produces positive outcomes. 11 However, in this study attrition rates did not differ between the addicted and nonaddicted groups of adolescents, contrary to the repeated assertion made by the authors about this key measure of the impact of their intervention.
Without any meaningful difference in process or outcomes in this research, it is very unlikely that this article would have been published in Childhood Obesity—or perhaps anywhere. More importantly, such clinically insignificant findings once again raise questions about the validity of the food addiction construct. We have taken those doubts about construct validity to the next level: food addiction may prove more harmful than helpful as a means of explaining barriers to weight control.4,8
Food Addiction: Questionable Validity and Potentially More Harmful than Helpful
Definitions
Some researchers have argued that the dramatic increases in obesity throughout the world over the past three decades correspond to increasing availability of cheap high-fat and high-sugar foods. 39 Could it be that people become addicted to such foods, and this powerful force has caused epidemic increases in obesity? Some parallels do exist between the brain chemistry associated with drug addiction and the effects observed (especially in animals) after consuming a lot of sugar. 3 This is particularly true for dopaminergic effects in the brain. However, parallels observed in the brain between addictive drugs and the intake of high doses of sugar make a very weak case for the usefulness of food addiction notion for the vast majority of weight controllers. Many stimuli, both chemical and behavioral, produce similar changes in brain chemistry. To meet a reasonable standard for addiction, researchers have argued that other criteria deserve consideration.
Gearhardt and Corbin
40
compared food addiction to the DSM-IV-TR criteria for substance dependence.
41
DSM-IV-TR defines substance dependence as the presence of serious degree of distress or impairment in functioning, and at least three of seven of the following criteria over the past 12 months:
Tolerance (physiological) to Increasing Amounts of the Substance Withdrawal Effects When Use of Substance is Discontinued Loss of Control Repeated Failed Attempts to Reduce or Stop Consumption Substantial Time Spent to Obtain, Use, and Recover from Use of the Substance Giving Up Important Other Important Activities Continued Use Despite Physical or Psychological Problems
Distress and impairment
The distress and impairment criterion creates the first problem for considering obesity to result from food addiction. Many overweight people do not view their weight status as a problem, nor are they impaired by it. Certainly most significantly overweight people work, maintain families, and do not show evidence of serious distress or impairment. 42 For example, Fitzgibbon, Stolley, and Kirschenbaum 43 found that overweight people who sought professional help showed more distress than those who had similar weight problems, but did not seek help. The latter group, employees at a major teaching hospital, reported the usual level of stresses and strains of everyday life, no more or less.
On the contrary, those who suffer from substance addiction tend to experience significant psychological distress and impairment in functioning. Greenfield and Crisafulli 44 found dramatically elevated levels of psychological distress among those who have substance use addictive disorders (SUDs) compared to population norms. They reported that about 30% of those with SUDs had mood disorders at some point in their lives compared to 8% in the general population. They also noted dramatically higher rates (3–20 times higher) among SUDs for a variety of other serious psychological disorders, including anxiety disorders, psychotic disorders, and personality disorders. In sharp contrast to people with SUDs, most studies show either no difference in psychological functioning or mild elevations of such problems among obese individuals—adults and teenagers.42,45
Tolerance and withdrawal
Tolerance, needing an increasing amount of the substance to produce the desired effects, is a common feature of addiction. People do not demonstrate tolerance toward foods. No scientific evidence exists to show tolerance to the enjoyment of eating in general, or to the enjoyment of specific foods.
Similar to tolerance, there is a complete lack of evidence for withdrawal symptoms from food. None of the researchers who contributed to the recent edited book by Brownell and Gold, 3 all of whom clearly favor the notion of food addiction, could find any evidence to support the existence of physical withdrawal from certain foods. At an anecdotal level, the authors can report on the incidences of withdrawal symptoms at the leading provider of treatment services for overweight young people in the USA for many years, Wellspring.28,29 In Wellspring's camps and boarding schools (designed and supervised by the first author), over its first 10 summers of operation (2004–2013), the directors (including the second author, the clinical director at Wellspring Florida in 2011) did not report a single case of physical symptoms of withdrawal among 10,000 participants. Both teenagers and young adults in these programs radically changed their diets (to a very low-fat reduced calorie diet) from the first day they begin their immersion experiences in the summer camps or boarding schools. Yet, none of them seemed to have evidenced flu-like symptoms or headaches, or any other sign of withdrawal, and none was brought to physicians or hospitalized accordingly. Actually, they generally reported feeling better physically almost immediately, with documentation from validated self- and parent-reported assessments of dramatic improvements in moods over an average length of stay of 5 weeks in the summer camps.28,45
Loss of control
As noted in a previous section of this article, some obese people do indeed report binge eating. However, if the food addiction construct is valid, then the majority of obese people would frequently lose control of their eating. However, the evidence does not support this position.30,32,46
The food addiction hypothesis also leads to the hypothesis that obese people who are prevented from binge eating, such as those who participate in intensive, immersion treatment, should exhibit considerable distress. There is evidence for this phenomenon in non-substance-related behaviors. Thaxton 47 found that requiring very consistent runners to stop running for a day made them quite distressed. Yet, in studies of cognitive-behavioral treatment of obesity, participants consistently feel much better as they participate in such programs.28,41,44 The loss of binge eating for the relatively few who binge regularly failed to cause the distress predicted by the food addiction hypothesis.
Repeated failed attempts to reduce or stop consumption
Unlike the situation in substance abuse, weight controllers clearly would not survive if they discontinued eating altogether. In contrast, research on the thousands of people who have succeeded at weight management shows that it is possible, although difficult, to reduce consumption of high-fat foods relatively permanently. 48
Substantial time spent to obtain, use, or recover from use of the substance
High caloric density foods do not require much effort to buy and consume, nor do they require any recovery after use. Consumption of calorie-dense foods does not meet this criterion, but neither do the use of common addictive substances such as cigarettes and caffeine. As in the prior example of repeated failures to succeed, this one also does not do well at discriminating dependence from independence regarding some substances.
Giving up important activities
The diagnostic criteria for SUD 41 involve the “failure to fulfill major role obligations” in work, school, or home. If food addiction were a primary cause of obesity, we would expect most obese people to have similar problems. Although obesity is associated with negative consequences, most obese people experience good functioning.42,43 They certainly do not frequently fail to fulfill obligations at work, school, or home due to their alleged food addictions. Also, many successful weight controllers avoid certain activities and situations, such as those that involve consumption of an excessive number of calories, to maintain successful weight control. However, is such restraint synonymous with a failure in obligations or worthy of a designation of dependence on food?
Relatively few obese people have binge eating disorders. 46 Of these few, some may also avoid others to continue their binges or to recover from binges, which could be classified as a failure of role obligations. However, the infrequency of such behavior, in contrast with the frequency of obesity, shows that this criterion for addiction does not match the experience of most obese people. This provides further evidence that the notion of food addiction fails to adequately explain the causes of obesity.
Continued use despite physical or psychological problems
People with common substance use dependences often continue using despite major legal, financial, interpersonal, and health problems. Some obese people certainly do continue consuming high-calorie foods despite increasing problems resulting from their obesity. However, many use such health problems to motivate themselves to seek treatment, too. Unfortunately, after failing to succeed using a variety of methods, a type of learned helplessness and lack of optimism about success probably contributes to sustained consumption of problematic foods. Self-efficacy and learned helplessness provide far better explanations than food addiction.49–51
Summary and conclusions
Table 1 summarizes the evidence comparing drug to food addiction on the distressed caveat and the seven criteria used to define substance dependence. The evidence and logic do not support the usefulness of thinking about the causes of obesity as a food addiction or defining most obese people as food addicts.
Drug Addicts versus Obese People Compared on the Eight Elements of the Diagnosis of Substance Use Dependence (Addiction)
Reprinted with permission from Kirschenbaum. 4
Binge Eating, Obesity, and Food Addiction: By the Numbers
In 2007, Hudson, Hiripi, Pope, and Kessler 46 conducted a large-scale study using a representative sample of adults in the USA to estimate, among other things, the prevalence of binge eating disorder. 41 If indeed food addiction were a primary cause of obesity, one would expect that the prevalence of binge eating would be near that of obesity. About 69% of adults in the USA today are either overweight or obese. 52 The Hudson et al.'s 46 survey revealed that only 2.8% of adults report any lifetime incident of Binge Eating Disorder. Figure 2 illustrates the percentage of obese people in the USA in contrast with the percentage of binge eaters, a stark contrast of 69% against 2.8%. Also, many of those observed to be binge eaters were not overweight or obese. Sixty-nine percent of the ∼235 million adults in the USA means that there are about 162 million overweight or obese people in the USA. The food addict explanation for obesity suggests that the vast majority should be binge eating, at least 100 million. However, Hudson et al. 46 did not find this. They found a 2.8% incidence of Binge Eating Disorder, equating to about 6.6 million of the total number of adults (235 million). Even if the vast majority of those 6.6 million people were overweight or obese, it would mean that only 5–6 million, not 100 million, reported this problem.

Percentage of American adults who are overweight or obese vs. % who were diagnosed with Binge Eating Disorder in the survey by Hudson et al. 45
Research Suggests Potentially Harmful Effects of the Food Addict Construct
Many people view those with mental/behavioral disorders in very negative ways.53,54 Those suffering substance abuse disorders, or “addicts,” are no exception. Labeling obese people as food addicts applies this stigma to this group, which already suffers weight bias. The food addiction construct may create far more problems for weight controllers than it is worth. Several lines of research support this conclusion.
Medical Model vs. Social Learning Model
In a study contrasting the medical and social learning models, Fisher and Farina 55 taught undergraduates from one of the two perspectives. The first was the classic medical model that views problems as symptoms of underlying disorders. Diagnosing these disorders is supposed to enable therapists to match treatments to the various types of disorders effectively. The food addict notion fits well with the medical model, viewing food addicts as diagnosed patients with additional underlying and abnormal mental problems. An alternative view, the social learning model, asserts that problems in living often occur because people learn maladaptive ways of handling challenges. As such, they can unlearn those patterns and change by setting new goals, problem-solving, and taking action. Participants who received the social learning messages actually viewed change more optimistically and worked on their own issues more consistently during the course. The medical model that oriented people to medical disease concepts, like the food addict perspective, can decrease active and effective efforts to change.
Optimism and Perceived Control
Viewing weight problems as caused by an addiction can lead to substantial pessimism about the prospect of changing. Scheier and Carver 56 defined dispositional optimism as the global expectation that good things will be plentiful in the future and bad things scarce. Peterson 57 summarized the research on dispositional optimism noting that optimism affects self-regulation when people face impediments to achieving their goals. Optimism leads to continued efforts to attain the goal, whereas pessimism leads to giving up. Studies on optimism56,57 viewed in this way showed that relatively optimistic people tend to feel happier and engage in challenges in more active and effective ways. If the food addict idea breeds pessimism, then it also leads to sadder moods and more difficulties with the process of changing lifestyles. Having control, or perceiving control, increases motivation, coping, and problem-solving. 58 The food addiction notion suggests that eating is beyond the control of those who are obese. 59 This view fosters an overly accepting attitude (i.e., something that cannot be changed) and, relatedly, pessimism about the prospect of change; that may impede coping with the many challenges of changing lifestyles.
The Weight Controller Athlete
People often view obese individuals, in very sharp contrast to athletes, as weak, neurotic, stupid, and slovenly.42,60 This weight stigmatization adds difficulty to the already great challenge of weight control. We offer a more useful, empowering view of people who are overweight and obese: they face the challenges of weight loss as athletes, not food addicts.4,8
Becoming a long-term weight controller is much like becoming a good athlete.4,29 People trying to lose or control weight experience tremendous resistance from their bodies from biological factors [e.g., excess fat cells; differential hormones and enzymes (insulin, lipoprotein lipase, leptin, ghrelin, and adiponectin); adaptive thermogenesis; and set points 4 ]. Weight controllers also face biological resistance in the form of fatigue, muscle soreness, and other physical sensations. Similarly, athletes must push their bodies beyond what is comfortable to achieve their goals. Athlete's bodies certainly resist practicing very intensely for the 4 hours+ per day required for maximum success, often pushing their bodies to the point of developing overuse injuries and then having to rehabilitate. 61
Learning to become a long-term weight controller also requires the learning and mastery of new skills (nutrition, exercise, and self-monitoring). Performance in sport requires similar mastery of new skills to maximize strength and speed, and perform best under pressure. Finally, success in both weight control and athletics requires a specific mental approach, a consistent and unrelenting focus to achieve a goal (a healthy obsession), often nurtured by others like coaches, sport psychologists, and CBT therapists.4,62,63
A healthy obsession is defined as “a sustained preoccupation with the planning and execution of target behaviors to reach a healthy goal”. 4 For example, a healthy obsession for a successful weight controller provides the focus to achieve consistency in self-monitoring food intake, choosing healthy low-fat foods, and staying very active every day. A healthy obsession for an athlete is similar, but instead of controlling weight, the goal is to sustain that daily preoccupation and execution to train the body and mind for maximum performance. The benefits of this mindset to athletes are obvious, but empirical evidence indicates the utility of it to weight controllers as well. For example, Kristen Gierut Caraher and her colleagues62,63 found that weight controllers who adhered to the Healthy Obsession Model 4 had much greater success than those who did not. They also found that successful weight controllers exhibited attitudes and sources of motivation that were remarkably similar to those of elite athletes.
Conclusions
There are at least two ways to conceptualize obese people who want to succeed at the great challenge of losing weight and keeping it off. The first is that these people are addicts, addicted to food like someone would be addicted to heroin or alcohol. This view probably fosters helplessness, pessimism, and inaction, ultimately increasing the probability of negative health outcomes. From a construct perspective, food addiction has to date failed to show evidence of discriminant validity beyond the simpler and less pathologically oriented concept of distressed binge eating. Also, as this review of Tompkins et al.'s study suggests, future research on the food addiction construct would serve science and clinical goals far better if it included four things: (1) assessment of distressed binge eating so that it might test for the discriminant validity of the construct; (2) treatment that meets widely recommended standards (intensive CBT) and at least a 1-year follow-up; (3) sample size large enough to provide adequate statistical power as well as generalizability; and, (4) intent to treat analyses.
We also offered a view of obese people who want to lose weight that provides a viable and more positive alternative to food addiction, weight control as an athletic challenge. The community of medical and psychological providers has a choice. We can accept the empirically unsupported view that many obese people develop and sustain their excess weight due primarily to addictions to food. If we accept such a construct (without tenable construct validation), we must also accept the consequences. However, we can, instead, reject the notion of food addiction as a primary cause of obesity at this time and promote and test a much more empowering view: weight controllers are athletes (i.e., weight controller athletes), not addicts.
Footnotes
Author Disclosure Statement
No competing financial interests exist.