
Abstract
Abstract
Background:
Maternal overweight/obesity during pregnancy increases offspring's risks of obesity and cardiovascular disease (CVD). A possible pathway is by reduced physical fitness and physical activity (PA) levels in children of overweight/obese mother. We assessed whether maternal prepregnancy overweight/obesity independently determines cardiorespiratory fitness (CRF), muscular strength, moderate-to-vigorous physical activity (MVPA), and sedentary behavior (SB) in 8- to 9-year-old children. We also assessed whether child's fat mass (FM) mediates these associations.
Methods:
One hundred ninety-four children of Dutch ethnicity aged 8.6 (± 0.4) years were randomly selected from a prospective birth cohort, the Amsterdam Born Children and their Development (ABCD) study. CRF was assessed by the 20-m multistage shuttle run test (20-m MSRT), muscular strength by hand dynamometry, and MVPA and SB by accelerometry. The association of prepregnancy body mass index (BMI) ≥ 25 kg/m2 with these outcome measures was assessed by multivariable linear regressions.
Results:
Mean (± standard deviation) attained 20-m MSRT stage was 5.3 (± 1.7). Compared with children from normal weight women, children of women with prepregnancy overweight/obesity attained a 0.80 (95% confidence interval: 0.15–1.50) lower stage, adjusted for child's sex and MVPA. This association was not mediated by birthweight or child's FM at age 5 years. Maternal prepregnancy overweight/obesity was not associated with child's muscular strength, MVPA, or SB.
Conclusions:
Maternal prepregnancy overweight/obesity was associated with reduced childhood CRF, but not with muscular strength, PA, or SB. Birthweight and FM at age 5 years did not mediate this association. Reduced CRF may partly explain the increased CVD risk in children of overweight/obese women.
Introduction
Lately, many studies have focused on the deleterious effects of maternal overweight (BMI 25.0–29.9 kg/m 2 ) or obesity (BMI ≥30 kg/m 2 ), since it affects up to 50% of women of reproductive age. 1 Numerous studies have shown strong relationships between maternal BMI and the health of their offspring. 2 Children from overweight or obese mothers have a higher risk of obesity, adverse fat distribution, increased blood pressure, increased insulin levels, and adverse lipid levels. 3 A combination of genetic, pre- and postnatal environmental factors is likely, and epidemiological studies indicated that the prenatal environment has sustained effects on the health of the offspring. 4 Furthermore, animal studies in which the intrauterine environment was manipulated unmistakenly show programming effects on offspring's health. 5
Poor physical fitness, low levels of physical activity (PA), and increased sedentary behavior (SB) are independent risk factors of obesity, cardiovascular disease (CVD), metabolic disease, and all-cause mortality later in life. 6 Physical fitness, PA, and SB are closely related, since high levels of PA and less SB lead to improved physical fitness. 7 However, PA is not the only determinant of physical fitness, as individual response to exercise training differs substantially, and familial, genetic, and environmental influences might be stronger determinants. 8
While evidence is scarce and exact mechanisms remain poorly understood, a potential explanation for the development of physical fitness, PA, and SB is through developmental programming. 9 For example, children with low birthweight, a proxy of poor in utero circumstances, have reduced cardiorespiratory fitness (CRF) and muscular strength.9,10 Preliminary animal evidence also links prepregnancy overweight or obesity to diminished childhood CRF and muscular strength. Animal studies show reduced muscle quality in offspring of obese ewes and disturbed metabolic processes in offspring of obese rats.11,12 Furthermore, studies on rodents show that offspring of over- and undernourished mothers during pregnancy were less physically active and had increased fatness during postnatal life. 13 These studies suggest that reduced physical fitness and PA and increased SB might partly explain how an adverse intrauterine environment leads to the development of noncommunicable disease.
This study aims to assess the association of maternal overweight or obesity before pregnancy with physical fitness, PA, and SB in the offspring. Therefore, we studied whether maternal prepregnancy BMI (ppBMI) ≥25 kg/m 2 is an independent determinant of childhood CRF, muscular strength, moderate-to-vigorous physical activity (MVPA), and SB at age 8–9 years. In addition, we assessed the potential mediating effect of birthweight and fat mass (FM) at age 5 years in these associations.
Methods
Participants
This study was conducted within the Amsterdam Born Children and their Development (ABCD) cohort. This prospective multiethnic community-based birth cohort was established to assess prenatal and early-life influences on future health. The ABCD cohort profile and study design have been previously described. 14 In summary, 8266 pregnant women from Amsterdam, the Netherlands, participated by completing questionnaires during and after their pregnancies. These surveys covered sociodemographic information, dietary habits, lifestyle, psychosocial factors, medical and specific obstetric history, and perinatal details. A total of 6575 mothers provided follow-up growth data on their child. A total of 3321 children participated in the 2008 health check at the age of 5 years. The collected data include height, weight, body composition, blood pressure, and parent-reported information on child's health and development.
In 2012, a weighted random sample of 400 children, aged 8–9 years at the time, from the ABCD cohort was contacted. Inclusion criteria were as follows: (1) participated in the age 5 years health check; and (2) Dutch ethnicity, that is, both parents born in the Netherlands to exclude confounding by ethnicity. Due to the original purpose of the study, low birthweight children had twice the chance of being selected to ensure enough power to assess the association of (low) birthweight with fitness. 15 Of the 400 children, 194 consented to participate in this study on physical fitness. A flow chart of the participants is presented in Figure 1. The Ethics Committee of the Academic Medical Centre in Amsterdam, the Netherlands, approved this study. Informed parental/caregiver consent was obtained from all participants.
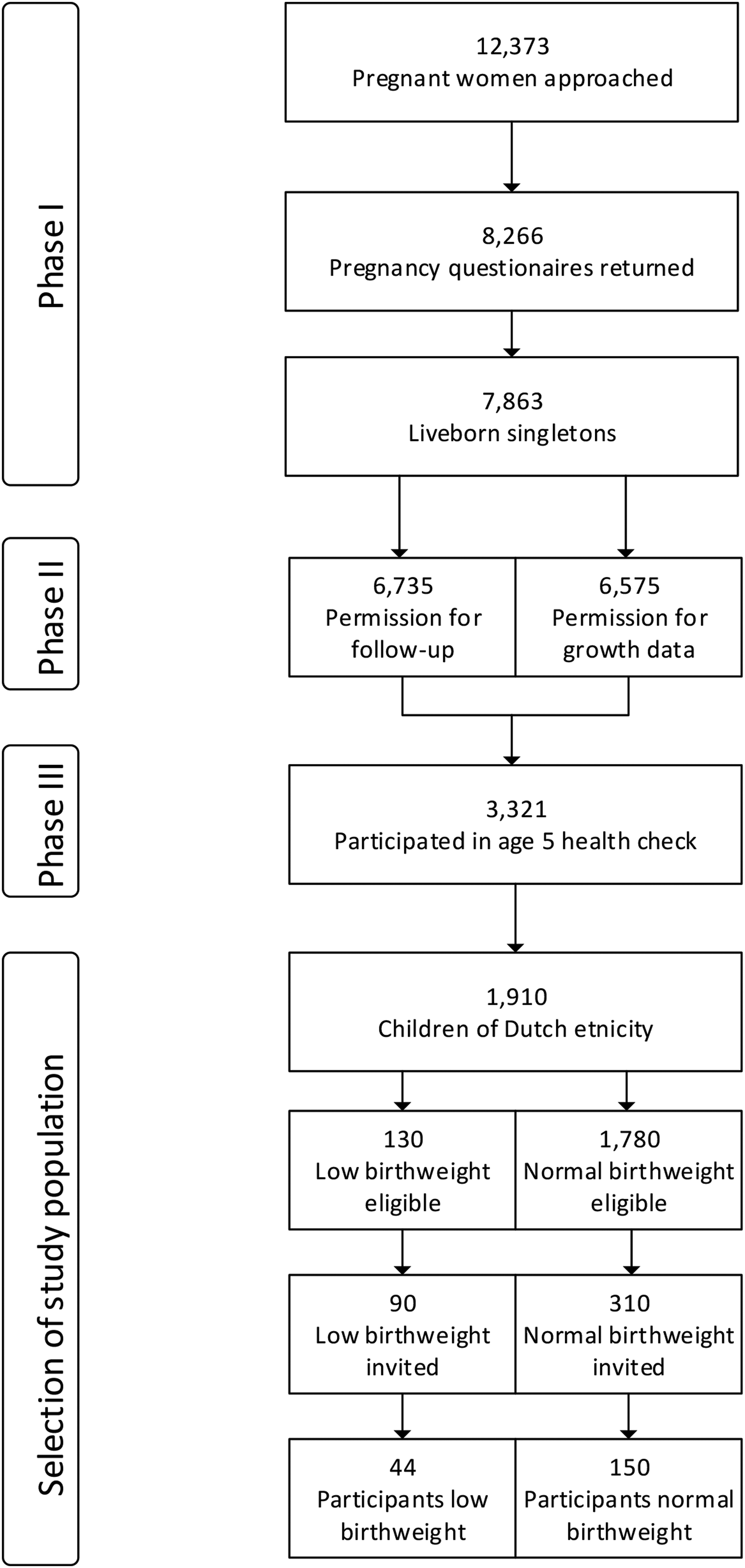
Study flow chart.
Anthropometry
Child's anthropometry was assessed by trained researchers during one of three identical test days between September and October 2012. According to standardized protocols, height was measured to the nearest 0.1 cm by a Leicester portable height measure (Seca, Hamburg, Germany). Weight was measured to the nearest 0.1 kg using a Marsden MS-4102 weighing scale (Oxfordshire, UK). Children were dressed in light clothing.
Fitness Testing
All children performed physical fitness testing on the same day as anthropometry measures were taken. Children were motivated to perform to the best of their abilities. CRF was measured by the 20-m multistage shuttle run test (20-m MSRT) as described by Léger et al. 16 The last completed half stage at voluntary exhaustion was defined as outcome. For supplementary analyses, maximum oxygen uptake (VO2 max) per kilogram was calculated from the last completed stage based on validated equations. 16 Isometric muscular strength was assessed using hand grip strength with a hand dynamometer (Jamar® Hydraulic Hand Dynamometer; J. A. Preston Corporation, Clifton, NJ). The device was adjusted to the appropriate age- and sex-specific grip span. 17 The 20-m MSRT and hand grip strength measures are noninvasive, simple, valid, and internationally used field test to assess CRF and upper body maximal strength in this age group.18,19
PA and SB
Omnidirectional accelerometers were used to objectively measure child's PA and SB. Triaxial Actigraph® accelerometers (Actitrainer or GT3Xs, Pensacola, FL) were worn on the right hip for 7 consecutive days, starting the day after the physical fitness tests. Devices were not worn during sleep, bathing, or swimming. Accelerometer data were processed as previously described. 15 Data were collected in 15-second epochs to accurately collect short bursts of PA. Cutoff values for MVPA and SB were set at >3000 and <100 counts per minute, respectively.20,21
Potential Mediators and Confounders
As a potential mediator, birthweight was obtained from the regional municipal health administration. Body composition was measured during the age 5 years health check and not simultaneously with fitness testing. We assessed body composition by arm-to-leg bioelectrical impedance analysis (BIA) with the Bodystat 1500MDD machine (Bodystat, Inc., Douglas, UK). BIA measurements were done in a standardized fashion; that is, in fasting state and after urinating. FM was derived from electrical impedance with equations validated for use in children. 22 Various potential confounders relating to either child's fitness or PA were considered, including sex, gestational age at birth, mode of conception, age at time of fitness measurements, MVPA and SB (when appropriate), socioeconomic status, exclusive breastfeeding ≥ 3 months, maternal smoking during pregnancy, maternal PA at time of pregnancy, and paternal BMI at time of pregnancy. The latter variables were collected by parent report in earlier phases of the ABCD study and were not available at time of fitness testing.
Statistical Analysis
Descriptive statistics are presented as means and standard deviations (SDs) for continuous data and as frequency distributions for categorical data. We stratified ppBMI using a cutoff value of 25 kg/m 2 , based on the World Health Organization criteria for overweight and/or obesity, because of the nonlinear relation between maternal BMI and offspring's health. 3 We compared characteristics of the normal and overweight/obese groups by Student's t-test for continuous variables, and by Fisher's exact test or Fisher–Freeman–Halton test for categorical variables.
There were < 5 (2%) missing values for gestational age, breastfeeding, FM, MVPA, and SB, and for paternal BMI there were 14 (7%) missing values. A nonresponse analysis revealed no significant differences in baseline characteristics between responders and nonresponders. Therefore, we concluded that missing values were probably missing at random. We performed single stochastic imputation and multiple imputation with the multivariate imputation by chained equations method. 23 Sensitivity analyses were done to assess substantial varying results depending on the imputation method. These showed comparable results for the primary analysis between these imputation methods. Therefore, the use of the single imputed dataset was deemed appropriate.
Primary Analysis
We assessed associations of ppBMI ≥ 25 kg/m 2 with the outcome measures (20-m MSRT, muscular strength, MVPA, and SB) by univariate linear regression analysis. Potential confounders were added stepwise by means of the change in estimate criterion. We included all confounders that changed the linear regression coefficient >10% in the adjusted model. To address the potential issue of multicollinearity, we computed the variation inflation factor (VIF) of all possible pairs of variables. This indicated that there was no concern for multicollinearity (VIF range 1.0–1.5). A correlation matrix of the potential confounders and outcome variables is presented as Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/chi). The linear regression model for ppBMI ≥ 25 kg/m 2 and 20-m MSRT was adjusted for child's sex and child's MVPA. The model explaining the association between ppBMI ≥ 25 kg/m 2 and muscular strength was adjusted for child's sex, gestational age, conception method, duration of exclusive breastfeeding, SB, maternal PA, and maternal smoking during pregnancy. The association between ppBMI ≥ 25 kg/m 2 and MVPA was adjusted for child's sex, gestational age, conception method, duration of exclusive breastfeeding, SB, maternal PA, and maternal smoking during pregnancy. Finally, the association between ppBMI ≥ 25 kg/m 2 and SB was adjusted for child's sex, MVPA, conception method, maternal PA, maternal smoking during pregnancy, and paternal BMI. Because of the limited number of overweight or obese women (n = 22), stratification for child's sex was not feasible.
Secondary Analyses
In a secondary analysis, we analyzed the association of maternal ppBMI as a continuous variable with childhood fitness. This helps evaluate whether childhood fitness has a continuous association over the full range of maternal ppBMI. For adequate comparison, we adjusted our models for the same set of confounders as in our models with ppBMI ≥ 25 kg/m 2 .
To assess whether birthweight or FM at 5 years mediated the association of ppBMI ≥ 25 kg/m 2 with any of the outcomes, we performed a multiple mediator analysis. A multivariate extension of MacKinnon's product-of-coefficient method for multiple mediators was used, and we applied 5000 bootstrap samples to compute confidence limits of the mediated effects using the PROCESS macro. 24
All statistical analyses were done with IBM SPSS version 22.0 for Windows. A significant statistical difference was defined as having a p-value < 5% (p < 0.05).
Results
Descriptives
One hundred ninety-four children participated in this study (response rate 48.5%), of whom characteristics are shown in Table 1. Mean age (± SD) of participating children was 8.6 (± 0.4) years, and 54% were boys. Nineteen (9.8%) children were overweight or obese (BMI z-score ≥ 1) at time of fitness measurements, but BMI and prevalence of overweight or obesity were not different between children of mothers with a ppBMI ≥ 25 kg/m 2 and children of mothers with a ppBMI < 25 kg/m 2 . Children of overweight/obese mothers before conception more often had overweight or obese fathers and were more often conceived through assisted reproduction techniques. Compared with eligible nonparticipants of the ABCD cohort, participating children had a lower birthweight and higher infant growth rates, which was the result of the recruitment strategy. 15
Characteristics of Study Participants by Maternal Prepregnancy Weight Group
Values are mean (±SD) or number (%).
Fisher's exact.
Fischer's exact with Freeman–Halton expansion.
20-m MSRT, 20-m multistage shuttle run test; FM, fat mass; GA, gestational age; METS, metabolic equivalent of tasks; MVPA, moderate-to-vigorous physical activity; ppBMI, prepregnancy body mass index; SB, sedentary behavior; SD, standard deviation.
Primary Analysis
Mean (± SD) attained 20-m MSRT stage was 5.3 (± 1.7). Table 2 shows the results of the univariate and multivariable linear regression analyses of ppBMI ≥ 25 kg/m 2 with the outcome variables 20-m MSRT stage, muscular strength, MVPA, and SB. In univariate analysis, a ppBMI of ≥ 25 kg/m 2 was associated with a 0.80 lower 20-m MSRT stage [95% confidence interval (CI): −1.56 to −0.04] in the offspring, compared with normal prepregnancy weight. There were no significant associations of maternal ppBMI ≥ 25 kg/m 2 with muscular strength, MVPA, or SB in the offspring. After adjusting for child's sex and MVPA, maternal prepregnancy overweight or obesity remained significantly associated with a 0.80 lower 20-m MSRT stage (95% CI: −1.50 to −0.15) in the offspring.
Associations of Maternal Prepregnancy BMI ≥25 kg/m 2 with Childhood Cardiorespiratory Fitness, Muscular Strength, Physical Activity, and Sedentary Behavior
20-m MSRT, 20-meter multi-stage shuttle run test; BF, ≥ 3 months of breastfeeding; BMI, body mass index; CI, confidence interval; conception, natural, or assisted method of conception; GA, gestational age; MVPA, moderate-to-vigorous physical activity; PA, physical activity; ppBMI, prepregnancy body mass index; SB, sedentary behavior.
Secondary Analyses
The results of our secondary analyses, with maternal ppBMI as a continuous variable, are presented in Supplementary Table S2. In univariate regression analysis, each kilogram per square meter increase in maternal ppBMI was associated with a 0.08 stage decline in childhood 20-m MSRT stage (95% CI: −0.16 to −0.01). After adjustments for child's sex and MVPA, maternal ppBMI was associated with a 0.07 (95% CI: −0.14 to −0.01) lower 20-m MSRT stage in the offspring. Increased ppBMI was also associated with reduced MVPA in the offspring, with 0.63 (95% CI: −1.18 to −0.09) minutes per day less MVPA in the offspring for each kilogram per square meter increase in maternal ppBMI. The latter association was adjusted for childhood sex, gestational age, age at measurement, conception method, at least 3 months of breastfeeding, child's SB at measurement, maternal smoking in pregnancy, and maternal PA. The results of our analysis of child's CRF expressed as VO2 max per kilogram are shown in Supplementary Table S3.
Mediation Analyses
Figure 2 shows the results of the mediation analyses of birthweight and FM at age 5 years on the significant association of maternal ppBMI ≥25 kg/m 2 with child's 20-m MSRT score, corrected for child's sex and MVPA. The mediation analyses revealed that birthweight and FM at age 5 years had very small indirect effects of 0.01 (95% CI: −0.02 to 0.13) and −0.02 (95% CI: −0.14 to 0.02), respectively (A and B paths in Figure 2). This indicates that birthweight and FM at age 5 years, as proxy for childhood fatness, were no mediators in the association of maternal overweight or obesity with childhood CRF.
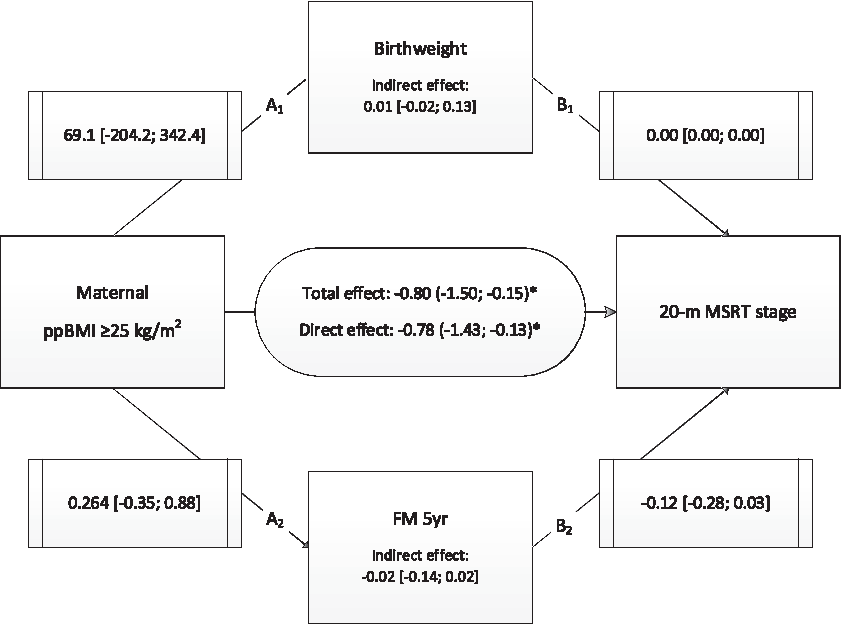
Mediation analyses of birthweight and FM at age 5 years. Results of the mediation analyses of birthweight and FM at 5yr on the association of ppBMI ≥25kg/m 2 with 20-m MSRT (regression coefficients with 95% CI in brackets). Total effect: association between ppBMI ≥25 kg/m 2 and 20-m MSRT without mediation. Direct effect: Association between ppBMI ≥25 kg/m 2 and 20-m MSRT with mediation. Indirect effect: Mediating effect of birthweight (A1 and B1 path) or FM at 5yr (A2 and B2 path). Analysis adjusted for child s sex and child's MVPA. *p < 0.05. CI, confidence interval; 20-m MSRT, 20-meter multi stage shuttle run test; FM, fat mass; MVPA, moderate-to-vigorous physical activity; ppBMI, prepregnancy body mass index.
Discussion
In this cohort of Dutch children aged 8–9 years, we found that maternal overweight or obesity before pregnancy was associated with reduced CRF in the child. This association remained significant after correcting for confounders, and was not explained by child's birthweight or FM at age 5 years. Prepregnancy overweight or obesity was not associated with reduced muscular strength, lower PA levels, or more SB in these children. A secondary analysis indicated that maternal ppBMI as continuous variable was inversely associated with CRF and MVPA levels. Since low CRF is a strong determinant of later CVD, 6 the results of this study are in line with our hypothesis that the unfavorable effect of prepregnancy overweight or obesity on offspring's future CVD risk might partly be explained through reduced CRF in childhood.
Various factors influence CRF in children. Body composition is one of the strongest determinants of CRF. 25 Therefore, we examined the mediating effect of FM as assessed by BIA at age 5 years. Although FM was not assessed simultaneously with fitness testing, FM shows significant tracking during childhood and corresponds with changes in BMI. 26 As BMI at age 5 years showed a strong correlation (r = 0.76) with BMI at age 8 years (data not shown), changes in FM are probably small and not expected to affect the outcome of the mediation analysis. The mediating effect of birthweight and FM was small and not significant, indicating that child's adiposity did not explain the negative association between ppBMI and CRF. MVPA is also strongly associated with higher CRF, 7 but adjusting for MVPA did not attenuate the results of our analysis. This suggests that maternal prepregnancy overweight/obesity has a direct inverse association with CRF at age 8–9 years, independent of child's adiposity or activity level.
Similar to our study, Hagnäs et al. 27 found that high maternal ppBMI was associated with lower CRF in 508 military recruits aged 19–20 years, although after adjusting for maternal and subjects smoking the association disappeared. 27 Tikanmaki et al. 28 also found a negative association of maternal and paternal BMI before pregnancy with adolescent CRF and PA levels. 28 In contrast to our study, correcting for childhood BMI, as a measure of body composition, attenuated the results of the study of Tikanmaki et al., 28 while in the study by Hagnäs et al. 27 the association was largely mediated by offspring's BMI. During adolescence and early adulthood the relation of BMI with physical fitness and PA might predominate, as BMI increases and physical fitness decreases during adolescence. 29 BMI, physical fitness, SB, and PA are closely related, and associations might be bidirectional. Prospective studies reported an inverse longitudinal association between fatness and subsequent PA, SB, and fitness, but the reverse might also be true; that is, lower PA and fitness and increased SB might lead to increased adiposity. 30 Although our analysis did not show a mediating effect of child's adiposity at birth and 5 years of age, the association between maternal ppBMI and offspring's physical fitness might be mediated by adiposity at various degrees during the life course. 9
Many potential pathways relating maternal obesity to diminished child health have previously been explored. 31 Our study suggests a potential new pathway: an obesogenic environment in utero may induce early adaptations during fetal development resulting in lower CRF in the offspring's later life. Possibly, this pathway is explained by exposure to high fetal leptin levels. Cord blood leptin is higher in obese mothers, and leptin regulates fetal growth and development. 32 While birthweight of children from overweight/obese mothers was not statistically significantly higher in our sample, leptin might affect fetal muscle growth and/or other parameters, since high levels of leptin are associated with lower CRF in adults. 33 Another potential underlying mechanism might be altered muscle function. In animal studies, expression of myogenic differentiation 1 and glucose transporter type 4 genes was reduced in the offspring of overweight or obese dams. 12 Also, muscle biopsies of obese ewes' offspring showed increased fibrosis, lipid accumulation, and insulin resistance. 34 In humans, the effects of maternal obesity on offspring's muscles are much less studied, and other mechanisms could potentially play a role. 35
While muscle quality of children might be impaired by maternal overweight or obesity, we did not find an association of prepregnancy overweight/obesity with muscular strength. This might be due to the limited sample size. Another explanation is that the higher birthweight seen in children of overweight/obese mothers also reflects a higher muscular mass. 10 This might counteract the hypothesized detrimental effect of maternal obesity on muscle strength. We found no association of prepregnancy overweight/obesity with child's MVPA level in our primary analysis. However, our secondary analysis showed a negative association of maternal ppBMI as a continuous variable with child's MVPA. This is probably due to the higher statistical power of the analysis with the continuous ppBMI than with the dichotomous normal versus overweight/obese mothers. While we adjusted our analysis for the slightly higher reported PA level around pregnancy by overweight or obese mothers compared with normal weight mothers, maternal PA was not assessed at the same time as the child's fitness and MVPA measurements, and current maternal (or family) PA could potentially be more strongly related to the outcomes examined in our study.28,36
Strengths of this study are that data on the ABCD cohort were prospectively collected from pregnancy onward, and include reliable information on health, growth, and development of the children. Data on many potential confounders were collected, and included in the analyses. The used fitness tests are well known, widely accepted, considered valid for use in school-aged children, and in line with international recommendations. 18 Furthermore, we used objective measures to assess body composition, MVPA, and SB, using BIA and accelerometry, respectively.
There are several limitations that merit discussion. First, we could only include a small number of healthy children from the ABCD cohort who actively chose to participate. This might have induced a selection of more active and healthy children. However, levels of MVPA and SB were similar to a large European cohort. 37 Furthermore, by design, children with a low birthweight were overrepresented in the sample, since the initial aim of the study was to assess the association of low birthweight with childhood fitness. 15 While in this study there were no significant differences in birthweight between children from normal or overweight mothers, this selection did result in fewer overweight or obese mothers participating compared with the whole ABCD cohort (11% vs. 25%). 14 These factors might have resulted in limited power to detect associations of prepregnancy overweight/obesity with muscular strength, MVPA, or SB.
Second, BIA measurements were not done simultaneously with fitness testing, as addressed before. Furthermore, BIA assessment can only provide estimates of body composition. Since previous work within the ABCD study has validated the BIA measurement in (pre)school children, we consider it valid to rank children. 22 Third, to exclude confounding by ethnicity children selected were of Dutch ethnicity only, which limits the generalizability of the findings, although we expect similar associations to be present in children of different ethnicities. Fourth, maternal prepregnancy weight and height were self-reported. This possibly led to underestimation of the associations, as underreporting is common in higher BMI categories. 38
Conclusion
Maternal prepregnancy overweight or obesity was associated with reduced childhood CRF, but not with reduced muscular strength, PA, or increased SB. Birthweight and FM at age 5 years were no mediators in this association. The strong relation of childhood CRF with future (adult) cardiovascular health warrants intervention studies to assess a possible causal relation between maternal prepregnancy overweight or obesity and CRF in the offspring.
Footnotes
Acknowledgments
We express our gratitude to all participants of the study. Furthermore, we thank Martijn W. Heijmans for his statistical guidance. S.M. and A.W.v.D are supported by a Dutch Heart Foundation grant (Grant No. 2013T085). A.W.v.D. is funded by a grant from Netherlands Organization for Health Research and Development (ZonMw, Grant No. 40-00703-98-11627), The Hague, the Netherlands.
This study was approved by the Ethics Committee of the Academic Medical Centre, Amsterdam, the Netherlands. the study is registered with reference number 02/039. Informed parental/caregiver consent was obtained from all participants.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.