
Abstract
Abstract
Background:
Biological rhythm is the daily metabolic cycle of mammals that involves the sleep-wake cycles, hormone release, eating habits and digestion, body temperature, and other important bodily functions that are repeated daily. Thus, greater difficulty in maintaining the circadian rhythms may be involved in the increased risk of obesity. This study assessed the association between biological rhythm disruption and childhood obesity among school children.
Methods:
This is a cross-sectional study with 7–8-year-old school children enrolled in a public school in the city of Pelotas-RS. The sample was drawn through multistage sampling. The Biological Rhythms Interview of Assessment in Neuropsychiatry-Kids (BRIAN-Kids) was used to assess the degree of difficulty maintaining the biological rhythm. BMI was calculated as weight/height2 (kg/m2).
Results:
A total of 596 children and their caregivers participated in this study. The prevalence of obesity was 24% among school children, 28.9% for girls, and 19.4 for boys (p = 0.009). Obese children had greater difficulties in maintaining the biological rhythm compared to nonobese children (p = 0.007). Some of these difficulties included sleep (p = 0.008), overall activities (p = 0.027), social rhythm (p = 0.033), and eating (p = 0.032) pattern.
Conclusion:
Approximately one-quarter of children were obese. This finding was associated with the caregiver characteristics and some difficulties in maintaining the biological rhythm.
Introduction
Obesity is a chronic disease with a multifactorial etiology, including genetics, environment, metabolism, lifestyle, and behavioral components. Childhood obesity has increased dramatically in the past three decades and has become a major public health problem. 1 The management of obesity is complex and difficult. It is linked to numerous chronic medical conditions, including pulmonary, cardiometabolic, and psychosocial diseases. Prevention and early intervention strategies are the key to reversing the obesity epidemic. 2 Obesity in children may have negative psychosocial consequences. 3 A sedentary lifestyle and unhealthy eating habits may cause excess body weight, which is a marker of negative energy balance, 4 and may also lead to the disruption of circadian rhythms. 5
Biological rhythm is the daily metabolic cycle of mammals that involves the sleep-wake cycles, hormone release, eating habits and digestion, body temperature, and other important bodily functions that are repeated daily. Biological processes repeat every 24 hours and are called daily or circadian rhythms. It is the result of the interaction between endogenous time markers, such as hormones, and the exogenous ones called zeitgeber (time synchronizers such as social rhythm, temperature, feeding, and exercise).6,7 There has been evidence of the association between changes in circadian rhythms and negative health outcomes. A recent study showed that the circadian cycle can be a crucial factor in the development of obesity and metabolic diseases.5–8 Moreover, studies show that social behavior, ability to relate to each other, demonstrating synchronization, social organization in daily life, added changes in sleep-wake cycles, overall activities, food intake pattern, and social behavior may influence the weight of individuals.9,10
Previous studies have suggested that many factors can increase the BMI, among them, the duration of sleep. 8 Circadian rhythms also regulate appetite and food intake pattern. Sleep deprivation affects the energy balance and may increase the risk of obesity and weight gain. 11 Roenneberg et al. demonstrated that living “against the clock” may be a factor contributing to the epidemic of obesity, and suggested that improving the correspondence between biological and social clocks will contribute to the management of obesity. 12 Recent studies link energy regulation to the circadian clock at the behavioral, physiological, and molecular levels, emphasizing that the timing of food intake itself may play a significant role in weight regulation. 13 Physical activity also plays an important role in obesity, as demonstrated by previous studies.4,14,15 However, the traditional theory that associates physical activity and obesity may not fully explain weight gain. Thus, our hypothesis is that the biological rhythm disruption and all domains (sleep, social, eating pattern, and activities) can contribute to weight gain. Therefore, this study aimed to verify the association between biological rhythm disruption and obesity among school children in a southern city in Brazil.
Methods
Sample
This is a cross-sectional study nested in a larger study entitled “Healthy Childhood in Context: a multidisciplinary investigation”, conducted between August 2015 and November 2016 in the city of Pelotas-RS. This study was approved by the Research Ethics Committee of the Universidade Católica de Pelotas (UCPel), under Protocol number 843.526.
The sample selection was performed by probabilistic sampling, with municipal elementary schools as primary sample units. 16 Twenty schools were selected by systematic random sampling, from a total of 40 in the urban area. Inclusion criteria were to be a regular student at the selected school and to be born in 2008, and one of their respective caregivers. Exclusion criteria were inability of the child or the caregiver to understand or answer the instruments due to a medical condition or severe disability.
Data collection began after the free and informed consent was signed by the parents. It was divided into two parts: (1) the assessment of children during regular school classes and (2) at their homes where the parents (or caregiver) answered a questionnaire.
Instruments
The economic classification was assessed using the Brazilian Economic Index. The economic classification was assessed using the National Economic Index. This classification is based on the accumulation of material goods and the schooling of the head of the household. 17
BMI, height, and weight were obtained as follows: the child's height was measured in the standing position using a Cardiomed stadiometer (1 mm accuracy) with an easily moveable horizontal headboard that can be brought into contact with the most superior part of the head. The weight was obtained by a properly Tanita calibrated digital scale (100 g accuracy), considering a decimal digit of accuracy. The BMI for children was classified according to the World Health Organization (WHO) standards, which determines the use of an age- and sex-specific percentile for BMI. 18 Therefore, the children were classified considering a dichotomous variable that indicates whether they were overweight (≥ z-score +1 and < z-score +2) or obese (BMI z-scores >2). The z-score means the number of standard deviations that the obtained data are far from its reference median. 18
The nutritional status of the caregiver was classified according to the criteria used by the WHO. 18 It is defined as a person's weight in kilograms divided by the square of the person's height in meters (kg/m 2 ). The nutritional status of the caregivers was classified in three categories—eutrophic (BMI <25 kg/m 2 ); overweight (BMI ≥25 kg/m 2 ); and obese (BMI ≥30 kg/m 2 ). 18
The Biological Rhythms Interview of Assessment in Neuropsychiatry-Kids (BRIAN-Kids) was used to measure the degree of biological rhythm disruption and sleep, which corresponds to the difficulty that the child presents to maintain a standard (habitual routine), reported by caregiver. The BRIAN-Kids scale is a validated measure and evaluates exposure to exogenous cues, called zeitgebers (time synchronizers such as social rhythm, temperature, feeding, and exercise). The assessment scale consists of 20 items; of these, 17 items are added to generate a quantitative measure, with greater scores indicating more biological rhythm disruption. The final score can also be divided into four subscales: sleep, social rhythm, eating pattern, and overall activities. Parents or a caregiver answered the items of the scale corresponding to the difficulties maintaining the biological rhythm in the last 15 days. The score ranges from 0 to 3 on a Likert scale (0 = not at all; 1 = just a little; 2 = quite a bit; and 3 = very much). For sleep, the scores range from 0 to 15; for social, activity, and food pattern, the scores range from 0 to 12. Examples of items included the following: “What is the degree of difficulty of the child in completing activities related to the school? How much difficulty does the child have in completing the usual activities (completing a joke, and organizing the toys and the room)? How difficult is the child's ability to maintain rhythm and persistence in physical activities (such as playing a sport and doing physical activity at school)? How difficult is it for the child to complete his or her duties at the usual time? How difficult is the child to maintain meal times (breakfast, lunch, snack, and dinner)? What is the degree of difficulty of the child in making all meals (breakfast, lunch, snack, and dinner)? How difficult is it for the child to maintain the same amount of food eaten regularly? How difficult is it for the child to consume moderately stimulants (such as chocolate and cola) or sweets?” 9
Statistical Analysis
Double data entry was performed using EpiData software (version 3.1) to check for consistency and validation. The statistical analysis was carried out with the SPSS version 22 for Windows (SPSS, Inc.; Chicago, IL). Categorical data were expressed as absolute and relative frequencies. BRIAN-Kids total score and its subscales did not have a symmetrical distribution (Gaussian curve); thus, it was described with the median and interquartile ranges (IIQ). The analysis was performed by chi-square, Mann-Whitney U test, and Spearman correlation. Mann-Whitney U test takes into account the distribution asymmetry (interquartile range).
A multivariate model analysis was performed. For this purpose, confounding factors were considered variables associated with both outcome (obesity) and exposure (biological rhythms) at a significance level of 20% or less. Poisson regression was used to test the difference in the BRIAN-Kids scores and obesity; thus, a model was created for each subscale. The following variables were considered for total Brian-Kids scores: family socioeconomic status and caregiver nutritional status. For sleep domain: sex, family socioeconomic status, and caregiver nutritional status. For overall activities domain: age, family socioeconomic status, and caregiver nutritional status. For eating pattern: sex and family socioeconomic status. Social rhythm did not present confounding factors. Moreover, multiple linear regression was performed to investigate the association between BRIAN-Kids and BMI scores, adjusted by family socioeconomic status. Statistically significant associations for all tests were p ≤ 0.05.
Results
A total of 723 children, 8 years of age, were selected from 20 schools. Among these, 609 completed the evaluation, 34 (5%) were losses, and 80 (11%) were refusals. About caregivers, 596 completed the evaluation and 13 (2%) were losses. Therefore, the total sample consisted of 596 children and their caregivers, and 493 (82.7%) were mothers. Those 493 mothers who completed the evaluation and their respective children were included in this study. Finally, the total sample comprised 609 children and 596 caregivers. Dyadic data analysis simultaneously evaluated 596 dyads.
Boys (51.8%) and girls (48.2%), between 7 (44.3%) and 8 years (55.7%) of age were included in similar proportion. Most of them had white skin color (63.4%). The socioeconomic status of the families was presented by terciles. With regard to caregivers, most respondents were mothers or biological parents (91.1%), and had completed up to 11 years of education (84.7%). For the nutritional status of the caregivers, 38.9% were eutrophic, 31.1% were overweight, and 30% were obese (Table 1).
Sample Distribution and Factors Associated with Obesity among School Children in the City of Pelotas, RS-Brazil, 2015–2016
The prevalence of obesity among children was 24% (n = 143), 28.9% for girls and 19.4% for boys (p = 0.009). There was an association between childhood obesity, the family socioeconomic status (p = 0.001), and the caregiver nutritional status (p < 0.001) (Table 1).
In this sample, there was greater difficulty maintaining the biological rhythm pattern between the obese children [median = 12 (IIQ 6–21)], when compared to nonobese children [median = 9 (IIQ 4–17); p = 0.007], that is, the rhythm is more variable among obese. When the difference between the medians of the BRIAN-Kids subscales between obese and nonobese children was tested, it was found that there was greater difficulty in maintaining the sleep pattern (p = 0.008), overall activities (p = 0.027), social rhythm (p = 0.033), and eating pattern (p = 0.032) among obese children (Fig. 1). The differences in biological rhythms and subscale scores among obese children were observed even after adjusted analysis: biological rhythms [p = 0.005; 95% confidence interval (CI): 1.01–1.04]; sleep pattern (p = 0.008; 95% CI: 1.02–1.10), overall activities (p = 0.050; 95% CI: 1.00–1.10), and eating pattern approached the level of significance (p = 0.068; 95% CI: 0.99–1.10).

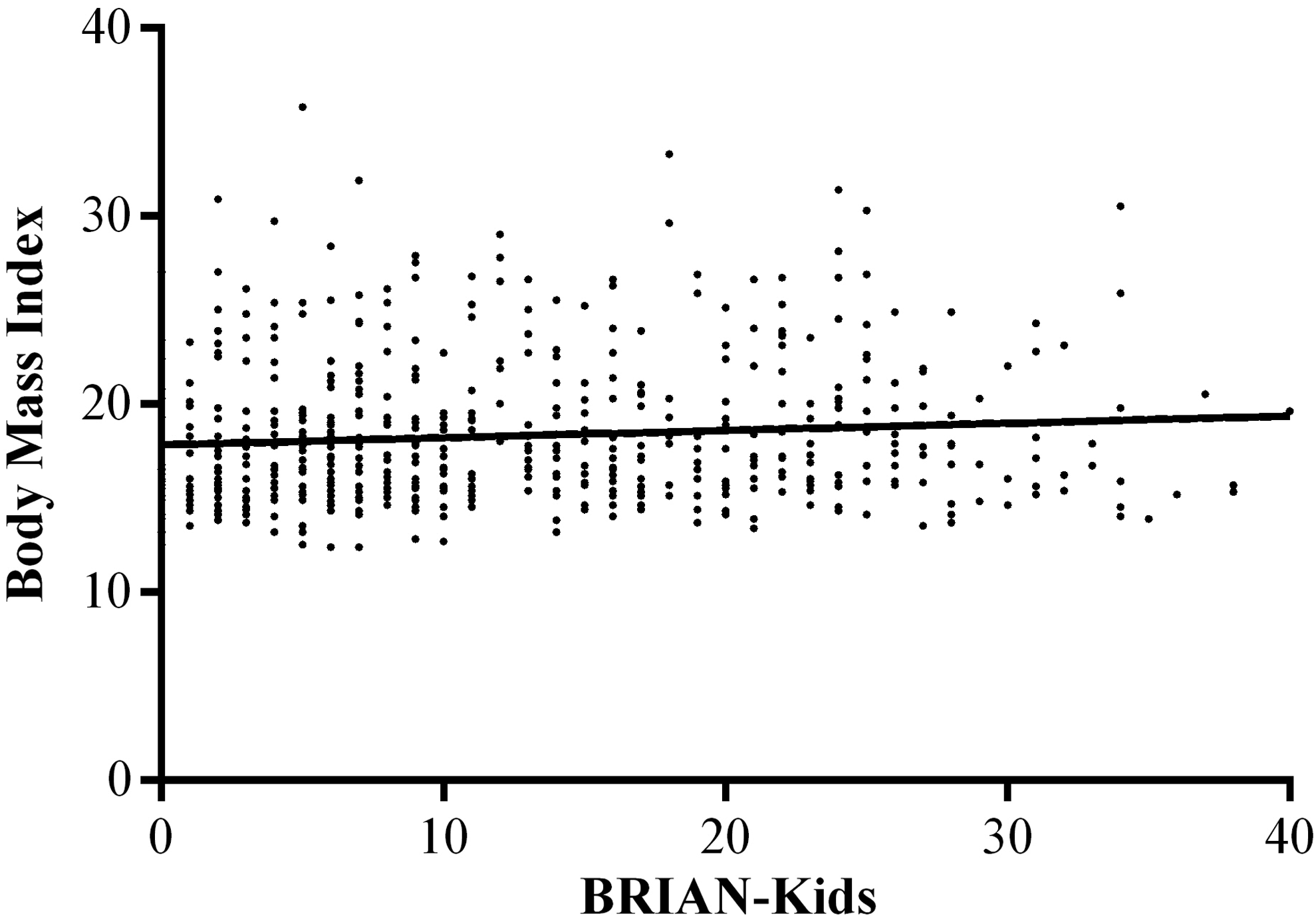
Nevertheless, there was a positive correlation between the BRIAN-Kids scores and the BMI scores of children, that is, the higher the degree of difficulty in maintaining the biological rhythm, the higher their BMI (r = 0.106; p = 0.010) (Fig. 2). After adjusting for potential confounders, the BRIAN-Kids and the BMI scores of children remained associated (B = 0.05; 95% CI: 0.015–0.080; p = 0.003).
Discussion
Obesity is based on an imbalance of energy intake and energy expenditure, in which the maintenance of the biological rhythm contributes to the energy homeostasis. A biological rhythm disruption, which includes changes in the sleep-wake cycle, eating pattern, overall activities, and social rhythm, would consequently be associated with childhood obesity. It is known that a great number of children do not participate in any physical activity recommended for children, 19 have a high level of sedentary behavior, 15 and also consume energy-dense foods (fast foods and sweetened drinks), which probably contribute to levels of obesity. 20 A study conducted in Brazil with 4–6-year-old preschool children showed a low level of physical activity (65%) with less than 1 hour of daily outdoor exercises. 21 With regard to social relations and activity, Ferrari et al. observed that the presence of computer in the child's bedroom is associated with higher BMI and lower level of physical activity. 22 Nevertheless, Dutra et al. reported a 70% prevalence of physical inactivity among children and that both the sedentary behavior and overweight were higher among children who spent more time watching television. 23
Recent evidence indicates that the duration and quality of sleep contribute to children obesity. 24 Children and adolescents, who sleep for a shorter period, especially with greater variability on weekends, are twice as likely to be obese compared to those who sleep for the recommended time.5,25 A possible explanation for this situation result would be the influence of sleep on hormones that control hunger and satiety, bad eating habits food to suppress hunger (caused by sleep deprivation) or domestic routines that decrease the desire to sleep and increase the consumption of palatable foods. 26 Among the hormones, ghrelin and leptin are potential candidates. Ghrelin plays a role in stimulating hunger, while leptin is responsible for the modulation of satiety. A systematic review showed that experimental reduction of sleep duration downregulates the satiety hormone—leptin—and upregulates the appetite-stimulating hormone, ghrelin, and increases hunger and appetite in adults. However, further studies with school age sample should focus on this topic, given that most studies have reported divergent results or no effects whatsoever. 27 Lack of domestic routines, such as eating regularly the evening meal with the family, having adequate sleep time, and limiting TV viewing habit, also seems to be associated with children obesity. 28 In contrast, the daily light exposure has also been associated with increased waist circumference, an important measure of central adiposity. 29 A study performed with mice has showed that long daily light exposure increased adiposity by decreasing caloric expenditure rather than increasing caloric intake. 30 Although the possible causes between the change in pattern and obesity are inconsistent, good sleep quality and an adequate amount of sleep for children (10–13 hours per night) are recommended to prevent the development of childhood obesity. 20
In this study with school children 7–8 years of age, it was observed that approximately one quarter of children were obese, according to the WHO criteria. The literature demonstrates that, although there are variations in prevalence estimates by age and geographical location, childhood obesity is a major public health problem. However, the sociodemographic factors associated with childhood obesity have generated contradictory results. In this study, children obesity was more prevalent among children from families with high income, and whose caregiver had higher education level. Schuch et al. observed an association between childhood obesity and maternal education among children in the state of RS, Brazil. 31 Another study evaluated abdominal obesity in children 3–10 years of age and found that it was associated with a higher socioeconomic status. 32 However, Barbosa et al. evaluated children 6 to 11 years of age and found no association between obesity and sociodemographic factors. 33 Nevertheless, we have observed that the nutritional status of children was associated with the nutritional status of their primary caregiver. The study carried out by Melzer et al. observed that the accumulation of abdominal fat was associated with maternal nutritional status. 34 In a review conducted by Davis et al., the factors related to obesity in children were associated with frequency of family meals, physical activity, and parental control. 35 In our study, childhood obesity was most prevalent among children who belonged to families with higher income and among those whose caregivers were also obese and with high education level. Family behavioral approaches that include parents and/or caregivers of children aiming to introduce healthier eating habits to their children have better results when compared to child participation only. 36
Although previous studies in literature have suggested that some measures of biological rhythm, including sleep adjustment, maintenance of meal schedules, and practice of physical activities, are independently associated with obesity, so far no studies have evaluated the biological rhythm or the difficulty in maintaining the biological rhythm, and the presence of childhood obesity. The main finding of our study was to determine that obese children have greater difficulty in maintaining the biological rhythm than those nonobese. We also found greater difficulty in maintaining sleep pattern, overall activities, social rhythm, and eating pattern among obese children. In addition, it was observed that the higher the degree of difficulty in maintaining the biological rhythm, the higher the BMI of children.
This study presents some limitations and strengths. The exclusion of private schools from the sample, which limits a potential comparison between private and public findings, can be considered a limitation of this study. Another limitation is that the prevalence of childhood obesity may have been underestimated for being evaluated in public schools, considering that children whose caregivers with higher education levels and high income showed a higher prevalence of obesity. The BRIAN-Kids is a subjective scale that investigates how subjects perceive themselves with regard to sleep pattern, activities, food, and social rhythms. Despite this relevant limitation regarding the prevalence of obesity, the findings related to the biological rhythm pattern may not allow for a broader generalization on this sample feature. However, there are also strengths as this study uses the BRIAN-Kids scale to verify the association between childhood obesity and biological rhythm. This association has not been previously found in published articles, using the referred scale. This study complements prior literature on the relationship between biological rhythm and childhood obesity because no study has specifically examined the biological rhythm in both obese and nonobese subjects.
Childhood obesity was observed in approximately one quarter of the children evaluated. This condition was associated with the caregiver characteristics and the degree of difficulty in maintaining the biological rhythm. Our findings are limited to behavioral issues, regarding a synchronization of rhythm between the child and his or her primary caregiver. An intervention for both children and caregivers to emphasize the importance of sleep, social rhythm, activities, and eating patterns could help prevent childhood obesity. Standardized sleep, wake time, and meal schedules should be encouraged.
Further studies are needed to support the findings of this study. Longitudinal studies are suggested since this research design is suited to assess whether children with difficulty in maintaining the biological rhythm have a higher risk for obesity or whether obese children display greater difficulty in maintaining the biological rhythm pattern.
Footnotes
Acknowledgments
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), and Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS).
Author Disclosure Statement
No competing financial interests exist.