
Abstract
Abstract
Background:
A comprehensive approach involving both environmental and individual strategies offers opportunities to strengthen school-based interventions for childhood obesity.
Objectives:
To evaluate a theory-based comprehensive intervention implemented within primary schools for childhood obesity in China.
Methods:
A 1-year, cluster randomized controlled trial was conducted in twelve primary schools (7–11 years old) in Beijing, China. Environmental and individual factors were improved in the intervention group (6 schools, 930 children) to promote knowledge and behaviors related to energy balance. The control group (6 schools, 959 children) did not receive any intervention. The primary outcome was body mass index (BMI) and its Z-score at 12 months. Generalized linear mixed models were used controlling for the cluster effect of school.
Results:
No significant differences were found between groups on BMI (0.07 kg/m2 [95% confidence interval (CI) −0.16 to 0.31, p = 0.54]) and its Z-score (0.02 [95% CI: −0.08 to 0.11, p = 0.73]) at 12 months. Self-reported knowledge, daily consumption of sugar-sweetened beverage, and frequency of moderate to vigorous physical activity improved at 12 months.
Conclusions:
The intervention did not mitigate excess weight gain, but did improve children's knowledge and several behaviors related to energy balance.
Introduction
Globally, child overweight and obesity is a significant public health concern. Although the rising trends in children's body mass index (BMI) have plateaued in many high-income countries, these have accelerated in low- and middle-income countries. 1 This is especially true among Chinese children with the annual increase rate of obesity during 2010–2014 greater than any other periods from 1985 to 2010. 2
Childhood obesity is associated with a wide range of adverse health consequences, including cardiovascular risk, sleep disorders, neurological difficulties, as well as psychosocial complications.3–5 From an economic perspective, lifetime costs have been shown to be significantly greater for men (or women) who were overweight or obese during childhood (3.7–5 times) versus normal weight children. 6 Collectively, these data highlight the urgent need to find effective ways to combat the obesity epidemic during childhood.
Schools are attractive settings to develop interventions, given their potential to influence students' knowledge and behavior. Previous school-based interventions, however, have largely focused on educational or behavioral strategies, and their effect sizes on adiposity-related measures (e.g., BMI and its Z-score or body weight) have been mixed, ranging from +0.17 (−0.38 to 0.72) to −0.29 (−0.45 to −0.14).7–9 From an ecological perspective, environmental and individual factors can simultaneously influence behavior and adiposity-related outcomes. 10 It is therefore important to consider environmental factors (e.g., the physical surroundings, social and cultural environment, or obesity-related policies) within interventions to achieve sustained behavior change. 11 Observational studies did show positive associations between school environmental factors (e.g., the availability of soft drinks at school) and BMI. 12 Moreover, a study using a twin design (hypothesizing that children's physical activity can be affected by both heritable and environmental factors) showed that the shared environment within sibling twins promisingly dominated the influence on children's daily activity levels (after controlling the genetic effects), and thus supporting the value of interventions focused on environments. 13
With the dramatic economic development in China, children are now growing up in an increasingly “obesogenic” environment. For example, the availability and ubiquity of computers and smartphones promote sedentary time and access to energy dense food and sugar-sweetened beverages is now widespread. Among the school-based interventions in China, few have focused specifically on environmental strategies.14,15 Given the burgeoning childhood obesity epidemic, we implemented a theoretically grounded, school-based intervention involving both environmental and individual strategies to promote healthy eating, physical activity, and reduction of sedentary behaviors among Chinese school children. The study aimed to evaluate the effectiveness of a school-based comprehensive intervention for childhood obesity in China, including (1) whether the school-based intervention would be effective for reducing excess weight gain among children and (2) whether the intervention would be beneficial for improving healthy eating, physical activity, and reducing sedentary behaviors among children.
Methods
This study has been reprinted in accordance with the Consolidated Standards of Reporting Trials (CONSORT).16–18 The checklist is provided in the Supplementary Data (available online at www.liebertpub.com/chi).
Study Design
A cluster randomized controlled trial (RCT) was conducted between October 2013 and September 2014 in primary schools in Beijing, China. The study was approved by the Ethic Committee of Peking University Health Science Centre (IRB00001052-12069).
A convenience sample of twelve schools (clusters) were selected from Dongcheng District, one of the central districts located in the east of Beijing. Participating schools fulfilled our eligibility criteria: school managers agreeing to implement this program; having at least 200 children from Grade 3–5 per school; not boarding schools; not schools solely for children with special skills; not schools of minor ethnic groups; and no similar program (a focus on weight gain prevention) that would be conducted during the following year after enrolment.
Within each school, ∼150 (142–185) students aged 7–11 years from Grade 3–5 were recruited. Eligible schools were randomly assigned (1:1) to either the intervention or the control group using computer-generated randomization sequences. After randomization, schools were informed of their experimental group allocation and took baseline measures. Given the nature of the intervention, it was not possible to blind participants or teachers at the schools. All data collectors were trained before investigation; however, they were not blinded to group allocation due to practical reasons.
Eligibility Criteria of Participants
Eligible children were those whose primary caregivers provided written consent to participate the program. After collecting students' medical history from their parents, we excluded individuals suffering from or having a history of any cardiovascular and metabolic diseases, asthma, and disabilities that could limit their ability to perform physical activity.
Intervention
We applied the ANGELO framework (“Analysis Grid for Environments Linked to Obesity”) in developing the intervention elements. 19 We underwent four stages: (1) First, we reviewed previous literature to identify intervention approaches potentially effective in the context of China 15 ; (2) Then we conducted focus group discussions and interviews with key informants (children, parents, teachers, school principals, local health, and education officials) to further revise and refine the intervention approaches; (3) Taken information from previous stages, we prioritized a list of environmental elements in implementing the ANGELO framework as shown in Figure 1. The key components were classified into three types: the political (“policies or rules introduced by the intervention”), the physical (“physical elements introduced by the intervention”), and the sociocultural (“ways introduced by the intervention to promote healthier attitude and beliefs”). We did not include the economic type of environmental components, which was originally designed in the ANGELO framework, for it was not feasible in this study; and (4) To test feasibility of the proposed intervention, we also undertook a pilot study at one school among 156 students aged 8–10 years before this cluster RCT. 20 Based on all the works mentioned above, we finally developed the intervention elements according to the ANGELO framework (Fig. 1), which are described in detail below.
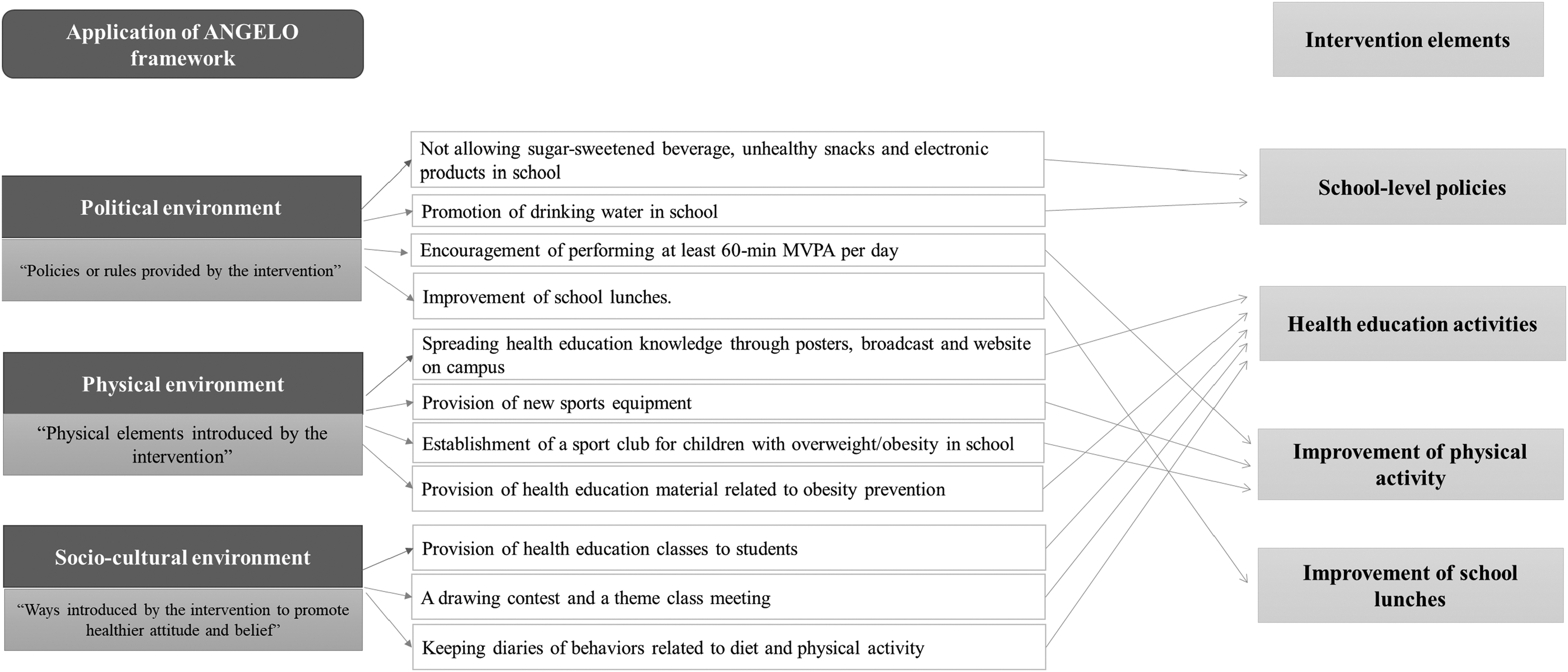
Environmental elements of this school-based intervention under ANGELO framework. ANGELO, Analysis Grid for Environments Linked to Obesity.
School-level policies
Throughout the intervention period, students were told not to drink sugar-sweetened beverage or eat unhealthy snacks in schools, and drinking water was advocated. They were also told not to play electronic products (e.g., smart phones and tablet computers) in schools. Children were encouraged to perform at least 60 minutes of moderate to vigorous physical activity (MVPA) each day.
Health education activities
Delivery personnel (class teachers) of health education activities had been trained by study team members. Emphasis was put on participatory teaching method (i.e., case discussions, brainstorming, practices, scenario analyses, game playing, and singing songs) and interaction between teachers and students. A total of four health education lessons were delivered to children in the first semester, with one 40-min lesson delivered once every 2 weeks. Key messages of these health education classes are outlined in Table 1. These key messages were developed based on social cognitive theory. Students acquired not only knowledge of health risks and benefits of different health practices but also practical skills related to obesity prevention. For example, they could judge their nutritional status by using “nutrition evaluation turnplate for Chinese students.” To strengthen application of the knowledge, a drawing contest and a theme class meeting (the theme was “healthy eating and physical activity”) were held in the second semester. Health education knowledge was also spread through posters, broadcast, and website on campus.
Key Messages in Four Health Education Classes
BMI, body mass index; MVPA, moderate-to-vigorous physical activity.
Students were asked to keep diaries of behaviors in relationship to diet and physical activity for a week (from Monday to Sunday) once a month. Self-reported behaviors included whether they were (1) eating five portions of vegetables and fruits; (2) eating no more than 1 portion of meat; (3) not consuming sugar-sweetened beverage; (4) spending no more than 2 h/day on screen viewing; (5) spending no less than 1 h/day spent on MVPA; (6) not bringing unhealthy snacks or sugar-sweetened beverages to school; (7) drinking more than 800 mL water at school; and (8) not playing smart phones or tablet computers at school. If they actually achieved one of the eight target behaviors, they could draw a smiling face [for “(1)”–“(5)” behaviors mentioned above] themselves or received a sticker from their group leaders [for “(6)”–“(8)” behaviors mentioned above].
Improvement of physical activity
Schools were required to provide at least three 45-minute physical education (PE) classes per week, with at least 30-minute MVPA in each class. We trained PE teachers how to design PE courses according to national PE criteria in China, ensuring sufficient time and intensity of physical activity in PE course. We also provided students with small sports equipment to support the various extracurricular activities that children were interested in (e.g., rope jumping and shuttlecock kicking). In addition, students were encouraged to perform exercise at home and instruction manuals were distributed to them, which provided suggestions on types of activities they could engage in. Moreover, the extracurricular activities for children who were overweight/obese were encouraged by their parents, after the head teacher told their parents that the sport club (named as “Xiao Zhuangzhuang” in Chinese) was offered. PE teachers organized the club at weekdays, which consisted of 30-minute activities at moderate to vigorous intensity. Although this program was not compulsory, children with overweight/obesity were encouraged to participate for at least 3 days per week.
Improvement of school lunches
We collected recipes of school lunches and analyzed the total energy intake and ratio of energy supply from carbohydrates, proteins, and fats of these recipes. According to nutritional standards, trained investigators then assessed the recipes of school lunches and provided practical suggestions to the managers of school lunch to improve children's dietary intake at school three times during the intervention (at baseline, midpoint, and end of the intervention).
Schools in the control group continued usual practice without involvement in any intervention during the 12 months' follow-up.
Main Outcomes and Measures
The primary outcome of this trial was children's BMI (and its Z-score) at 12 months. BMI (kg/m2) was calculated as body weight (kg) divided by height (m) squared, and its Z-score was then obtained according to the World Health Organization reference. 21 Secondary outcomes included the children's BMI and its Z-score at 6 months, the prevalence of overweight and/or obesity at 6 and 12 months, children's knowledge and behaviors related to energy balance at 12 months. Children's BMI status (underweight, normal, overweight, and obese) was defined according to the cutoffs among Chinese children and adolescents. 22
All measurements were conducted by a team who had received standardized training on anthropometric measurements or questionnaire survey. Children's height and weight were assessed at baseline, 6-month, and 12-month follow-ups. Children were required to measure their weight and height without shoes and wearing light clothes to the nearest 0.1 kg or 0.1 cm by using a lever scale or stadiometer, respectively. Knowledge and behaviors related to energy balance were reported using a self-administered questionnaire. Questions in relationship to knowledge were designed to test whether students mastered the key messages of health education. A total of 12 items in relationship to diet, physical activity, and sedentary behaviors were included. For example, participants were asked to judge “drinking sugar-sweetened beverage is healthier than water.” Three choices were provided: “right,” “wrong,” or “unknown.” Participants who chose “right” or “unknown” would be given 0 score, and those chose “wrong” obtained 1 score. The possible total score of knowledge is 12. Questions related to dietary intake were designed based on the validated Block Kids Food Screener (BKFS; correlations between BKFS and 24-h recalls ranging from 0.53 to 0.88), 23 and those related to duration of MVPA were based on a validated 7-day physical activity questionnaire (PAQ; correlations between PAQ and Caltrac motion sensor ranging from 0.38 to 0.46). 24 To be culturally adaptive, minor revisions were made on these original questionnaires according to our previous experiences. 25 To facilitate quality control of the questionnaire, students finished the questionnaires in the classroom in the presence of trained investigators, who were available to answer questions as needed.
Process Evaluation
Process evaluation was assessed in relationship to delivery of the following intervention components: (1) school-level policies, (2) health education activities, (3) improvement of physical activity, and (4) improvement of school lunches. Data were collected primarily via researchers' records of field work and direct observation. Scores for quantity and quality of delivery for each intervention element were given using a 10 point scale ranging from 1 (nearly no sessions delivered or low-quality delivery) to 10 (the number of sessions delivered exactly as proposed or high-quality delivery). Scores for each item were given by two independent investigators based on the unified and concrete scoring standard. Discrepancies between the two investigators were further discussed with the third investigator. The total scores of intervention delivery per school were then calculated and the schools in the intervention group were categorized into medium-to-high (the first two-thirds according to rankings in the total scores) or low (the last one-third) compliance.
Statistical Analyses
We aimed to recruit a total of 1800 students from 12 schools with an average cluster size of 150 students per school. This sample size would provide 90% power at 5% significance level (two-sided) to detect a between-group difference of 0.8 kg/m2 in BMI at 12 months, assuming a standard deviation (SD) of 1.8 kg/m2 and an intracluster correlation coefficient of 0.05. 15
Statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC). All statistical tests were two-sided at 5% level of significance. Baseline characteristics at both school and individual participants' levels were reported using descriptive statistics. Continuous variables were presented as mean and SD, and categorical variables were presented as frequencies and percentages.
The primary analysis was based on the intention-to-treat principle, including all randomized schools and students recruited from each school. Generalized linear mixed models were used to evaluate the intervention effect on primary and secondary outcomes measured at 6 and/or 12 months postrandomization, adjusting for baseline outcome value, age, and sex. The cluster effect of school and repeated measures on the same participant were taken into account in the multilevel modeling, and missing data were treated in the maximum likelihood estimates assuming they were missing at random. The intracluster correlation coefficient was also estimated. Sensitivity analysis was considered on the primary outcome using the last-value-carry-forward (LVCF) imputation on missing data. Model-adjusted mean group difference was reported on continuous outcomes (i.e., BMI, BMI Z-score, the total score of obesity-related knowledge, and the number of days doing ≥1 hour MVPA/week). Adjusted odds ratio (OR) was reported on binary outcomes (i.e., whether or not overweight/obese, the percentages of children consuming no less than 1 portion of vegetable/day, no less than 1 portion of fruit/day, no less than 1 portion of meat, sugar-sweetened beverage, and the percentage of children viewing screen for no more than 2 h/day) using a logit link. The 95% confidence interval (CI) and associated p-value were calculated.
Results
Characteristics of Participants
Of 12 eligible schools, 6 schools (930 children) were randomly assigned to the intervention group and the remaining 6 schools (959 children) to the control group. Participants (N = 1889) were on average 9 years old (SD = 0.67) at baseline, and 48.3% were girls. The mean BMI-Z of these children at baseline was 0.29 kg/m2 (SD = 1.22), and over one-third of them were classified as overweight (15.6%) or obese (19.6%). Baseline characteristics between the intervention and control groups were similar, except that children in the control group reported more frequent consumption of vegetables than in the intervention group (Table 2).
Baseline Characteristics of Randomized Schools and Participants
IQR, interquartile range.
All 12 schools completed the trial. At the individual level, measurements of weight and height were available for 1837 (97.2%) and 1839 (97.4%) participants at 6- and 12-month follow-up. Study flow is shown in Figure 2.
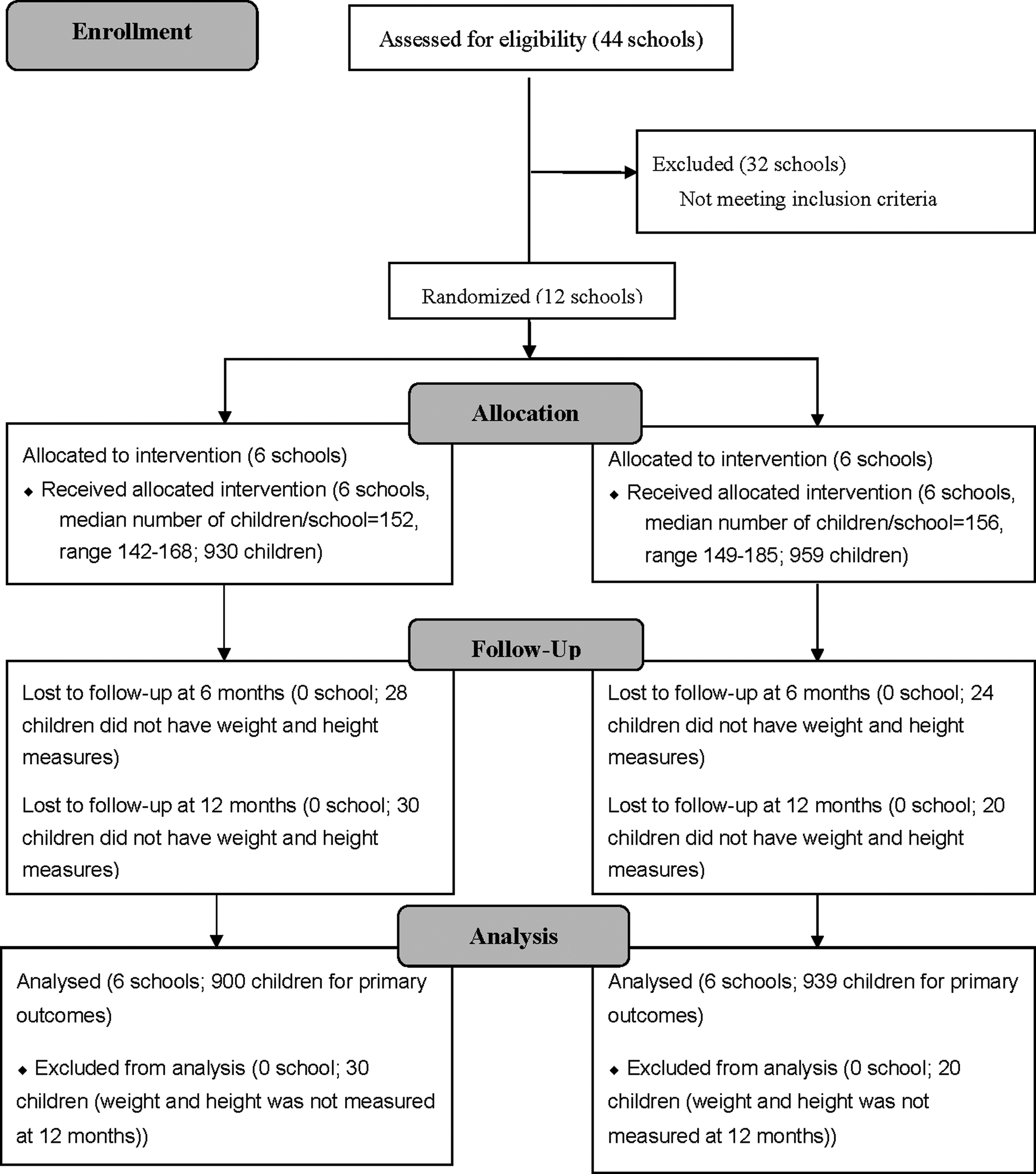
Trial profile.
Effectiveness of Intervention
Mean BMI (kg/m2) and BMI Z-score at 12 months were 18.57 (SD 3.60) and 0.31 (1.19) in the intervention group and 18.46 (3.76) and 0.28 (1.23) in the control group (Table 3). The model-adjusted group differences (intervention vs. control) in BMI and its Z-score at 12 months were 0.07 (95% CI: −0.16 to 0.31; p = 0.54) and 0.02 (95% CI: −0.08 to 0.11; p = 0.73). The estimated intraclass correlation coefficients were 0.04 and 0.05, respectively, consistent with the initial assumption. Sensitivity analyses using the LVCF imputation on missing BMI measures at 6 and 12 months showed consistent results with the primary analyses (not reported).
Continuous Outcomes at 6 and 12 Months Follow-up (Intention-to-Treat Analyses)
Linear mixed models have adjusted for baseline outcome value, age, and sex. The cluster effect of school and repeated measures on the same participant were taken into account in the multilevel modeling.
SD, standard deviation; CI, confidence interval.
Although the proportion of children with obesity was significantly lower in the intervention group than that in the control group at 6 months (OR: 0.50, 95% CI: 0.26 to 0.96; p < 0.05), no significant differences were seen between two groups in other anthropometric outcomes at 6 months or 12 months (Tables 3 and 4). For knowledge and behavior-related outcomes, significant effects in favor of the intervention were seen on obesity-related knowledge (mean differences: 0.19; 95% CI: 0.06 to 0.33; p = 0.005), the percentage of children consuming sugar-sweetened beverage (OR: 0.56; 95% CI: 0.42 to 0.74; p < 0.0001) and number of days conducting more than 60 minutes of MVPA per week (mean differences: 1.37; 95% CI: 1.49 to 1.60; p < 0.0001). No significant intervention effect was found on self-reported consumption of vegetable, fruit, meat, and sedentary behaviors related to screen viewing, watching TV, or doing homework (Table 4).
Categorical Outcomes at 6 and 12 Months Follow-up (Intention-to-Treat Analyses)
Generalized linear mixed models have adjusted for baseline outcome value, age, and sex. The cluster effect of school and repeated measures on the same participant were taken into account in the multilevel modeling. A logit link was used to estimate the OR.
OR, odds ratio.
Adherence to Study Protocol
The quantity of intervention delivery was 80%–100% for intervention elements among most intervention schools. Variability exist for the quality of intervention delivery, which was highest for the sport club for children with overweight/obese, followed by school-level policies, health education activities, improvement of PE classes, and improvement of school lunches (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/chi).
As a post hoc subgroup analysis, the effect of intervention was compared between participants in medium-to-high compliance schools (ranking in the first two-thirds for intervention delivery; 4 schools, 596 participants) versus those in control group (6 schools, 959 participants). Although BMI indices were not significantly reduced (adjusted mean differences on BMI and BMI Z-score: −0.12 (95% CI: −0.34 to 0.10); −0.05 (95% CI: −0.14 to 0.03)), prevalence of overweight or obesity and prevalence of obesity decreased in these medium-to-high compliance schools compared with those in the control group (adjusted ORs for prevalence of overweight or obesity, prevalence of obesity, respectively: 0.58 (95% CI: 0.37 to 0.92); 0.57 (95% CI: 0.35 to 0.94)).
Adverse Events
After the intervention, the percentage of children with underweight was comparable between two arms (4.9% in intervention vs. 5.3% in control, p = 0.75). We were not aware of adverse events reported by teachers, parents, or children.
Discussion
Summary of the Findings
Our study assessed whether a 1-year school-based comprehensive intervention was effective for the prevention of childhood obesity. Results showed that the intervention did not have a significant effect on body mass indices at either 6- or 12-month postrandomization. Concerning the secondary outcomes, prevalence of obesity at 6 months was significantly lower among children in intervention than that in control, but not at 12 months. While children's obesity-related knowledge, consumption of sugar-sweetened beverage, and frequency of MVPA significantly improved at 12-month follow-up, there were no group differences in other secondary outcomes.
Interpretation of the Findings
To date, while the majority of childhood obesity programs have been conducted within schools, most have targeted individual rather than environmental factors associated with obesity. 11 This is particularly true in China. 15 Our study emphasized the establishment of a school environment as well as individual strategies in supporting an active lifestyle (facilitation of children's healthy eating, physical activity, and reduction of sedentary behaviors). On the whole, more favorable changes were observed in self-reported obesity-related knowledge and behavior than anthropometric measures at postintervention.
There are several potential interpretations for this pattern of findings. We would like to explain the lack of trial success based on the mediating-moderating variable model. 26 To successfully prevent childhood obesity, the behaviors targeted potential mediating and moderating variables of behavior change need to be strongly and causally related to adiposity outcomes. As an example of the behaviors targeted, this study might have benefitted from targeting dietary patterns (i.e., aggregates of food groups) rather than single food groups (i.e., vegetables or fruits). 27 We were also likely missing promising mediators of behavior change such as stress management procedures, which has shown promise in improving dietary change in adult population. 28 Concerning moderators, the influence of peers should be paid adequate attention considering its increasingly important role for children approaching early adolescence. 26 In addition, the risk of childhood obesity is related to a complex interaction of factors at the individual-, family-, school-, and societal level. It is possible that a school-based obesity prevention program may be insufficient to counteract out-of-school influences on children (e.g., family or social environment). 29 Last but not the least, it is of interest to note that our intervention, to some extent, did work for schools with relatively satisfactory compliance. This indicates that cooperation with schools and quality control for the implementation of intervention are essential for the success of a school-based intervention for childhood obesity. More important, improvement of PE classes and school lunches had been shown greater difficulties than delivery of other intervention components. Future interventions in China should consider other feasible ways to combat childhood obesity within the school context.
Comparison with Other Studies
Two previous studies have demonstrated a significant decrease in BMI Z-score among children in a school-based intervention (incorporating the environmental components) compared with those in control; however, causal effects could not be determined due to their nonrandomization design.30,31 Randomization is mandatory to overcome possible selection bias. Our trial was among a few that have targeted environmental factors in school-based interventions using an RCT design.32–34
Two recent school-based environmental programs reported similar results as ours, with significant effects on behavioral outcomes but no significant differences on weight gain prevention.33,34 One project (modification of eating habits and physical activity) conducted in the United States was a pilot study including four schools only, and the sample size was unlikely to provide sufficient statistical power as stated by the authors. 33 The other program (incorporating school environment support) was conducted in 8 urban primary schools (1182 students) in Nanjing, China, but did not find a significant reduction in BMI among students in intervention group versus control group. 34
In contrast to results mentioned above, another 4-year randomized trial (promotion of physical activity by integrating environmental changes) conducted in France showed that adjusted BMI among children in the intervention group was significantly lower at 3 and 4 years relative to those in the control group. 32 Success of this intervention may be attributable to the duration that was longer than ours as well as other studies.33,34 Nevertheless, this interpretation should be treated cautiously as a previous systematic review, and meta-regression did not identify a clear relationship between “dose” of intervention (defined as intervention duration, the number of sessions, and the length of sessions) and weight-related outcomes. 35
Strengths and Weaknesses of This Study
Our study was among the first to develop and evaluate the effectiveness of a cluster RCT at both environmental and individual level in Chinese primary schools using a theoretical framework. Strengths of our study included the robust study design, an intervention developed on robust formative work and a pilot study, sample size achieving statistical power, high participation rate in the surveys, and the inclusion of sensitivity analyses. Nevertheless, the following limitations cannot be neglected. First, we did not measure whether environmental or other changes occurred at control schools during the trial period, which may attenuate the effect of intervention. Second, data collectors were not blind to group allocation, although they were trained according to the standard protocol. Third, we conducted a number of tests of secondary outcomes, increasing the risk of type 1 error. Fourth, we did not use accelerometers to objectively measure physical activity of all study population because we have insufficient accelerometers.
Conclusions
China faces both great challenges and opportunities to reverse the epidemic of childhood obesity. Findings from this study suggest that a 1-year school-based comprehensive intervention did not mitigate excess weight gain, but did improve children's knowledge and several behaviors related to energy balance.
Footnotes
Acknowledgments
We thank all the students and teaching staff who took part in the trial. We thank all the members in our research team, including investigator, cooperators, fieldworkers, computing, and data management researchers. H.J.W., R.M., C.N.M., and Y.J. designed the study. Z.L., Q.L., and Y.J. analyzed and interpreted the data. D.M.W., L.C., Y.C., and D.W. collected data. Z.L. is a major contributor in writing the article. R.M., C.N.M., Y.J., and H.J.W. revised and improved drafts of the article. All authors read and approved the final article. Funding: This study was funded by a grant from China Medical Board (Project No. 11-064). Trial Registration: ChiCTR, ChiCTR-TRC-13003509, registered on July 15, 2013, ![]() .
.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.