
Abstract
Abstract
Purpose:
The aim of our meta-analysis was to explore whether advanced maternal age (AMA) is regarded as an important risk factor for predicting macrosomia or not.
Methods:
Three databases were systematically reviewed and reference lists of relevant articles were checked. Meta-analysis of published cohort studies was done comparing whether AMA was associated with macrosomia and adjusting for potential confounding factors. Calculations of pooled estimates were conducted in random-effects models. Heterogeneity was tested by using chi-square test and I2 statistics. Publication bias was estimated from Egger's test (linear regression method) and Begg's test (rank correlation method).
Results:
Twelve cohort studies met the inclusion criteria. The meta-analysis showed that AMA was associated with macrosomia as an important risk factor. The adjusted odds ratio calculated for 12 studies (compared aged 35–39 years to aged <30 years) was 1.42, 95% confidence interval (CI) (1.25–1.60) for random-effect model and 6 studies (compared aged ≥40 years to aged <30 years) was 1.40, 95% CI (1.02–1.78) for random-effect model. There was no indication of a publication bias either from the result of Egger's test or Begg's test.
Conclusion:
Regardless of the underlying mechanism, our finding indicated that AMA should be considered as an important risk factor for macrosomia. To adequately evaluate the clinical evolution of AMA, the effect of AMA on macrosomia need to be carefully assessed and monitored.
Introduction
Advanced maternal age (AMA), defined as age 35 years and older at estimated date of delivery, has become increasingly common and related to a wide spectrum of adverse pregnancy outcomes. 1 Effective birth control, advances in assisted reproductive technology, delayed marriage, increasing rates of divorce followed by remarriage, and women's pursuit of higher education and career advancement all contribute to this trend.2,3
The number of two-child families has substantially increased because of the change in the family planning policy of the Chinese government in 2015. This increase will create new challenges in the field of obstetrics, and methods for dealing with these challenges should be urgently explored. 4 Currently, many families with only one child are planning to have a second child, which will result in a significant increase in the proportion of elderly parturient women, in other words, the mean age of pregnant women became significantly higher than before the policy. AMA is related to a wide spectrum of adverse pregnancy outcomes, such as macrosomia, low birth weight (BW), miscarriage and gestational diabetes. 5
However, there is no meta-analysis of relevant studies. Therefore, we carried out a meta-analysis of the literature focused on the association between AMA and macrosomia and this is the first meta-analysis on this issue applying a systematic identification of relevant studies and a prospective study protocol with a focus on careful adjustment of potential confounding factors.
Methods
Search Strategy and Study Selection
We performed a detailed search on studies that examined the association between AMA and macrosomia. A search of the literature was made using Medline (PubMed, www.bdpubmed.com/), EMBASE (www.embase.com) and Cochrane library (www.thecochranelibrary.com) from their inception to May 2018 to identify relevant articles. References in key studies were reviewed to identify additional studies not indexed by Medline, EMBASE or Cochrane library.
We used the following search terms: (“advanced maternal age” OR age OR “elderly parturient”) AND (“neonatal outcomes” OR “obstetric factors” OR macrosomia).
Cohort studies and case-control studies were included, irrespective of sample size. In addition, a hand search of reference lists of relevant and related articles was made to ensure a complete collection. Studies included in the meta-analysis had to meet the following inclusion criteria: focused on humans; published in English; reported effect of AMA on macrosomia; reported definition of macrosomia; reported adjusted odds ratio (aOR) and 95% confidence intervals (CIs).
Screening and Data-Extraction Form
All search hits were exported to Endnote X4 (Thomson Reuters), which was used to organize the references and eliminate duplicates. Initially, two investigators (X.J.H. and R.X.D.) independently screened the articles according to the predetermined criteria and the results from the electronic searches to select potentially relevant citations based on titles and abstracts, Potential disagreements were resolved through consensus. For articles with relevant citations or with titles/abstracts that were not sufficient for deciding on inclusion criteria, the full-text articles were retrieved and evaluated. The following characteristics were extracted from the articles: author, publication year, country, sample size, effect of AMA on macrosomia (compared macrosomia in women aged 35–39 years and ≥40 years with women aged <30 years), definition of macrosomia (macrosomia was defined as a BW ≥4000 g), potential confounding factors adjusted for.
Assessment of Study Quality
We assessed the methodological quality of included studies based on Newcastle–Ottawa Scale (NOS) for quality of cohort studies. 6 Eight questions were assessed, and each satisfactory answer received one point, resulting in a maximum score of 9. Only studies for which the majority of the questions were deemed satisfactory (i.e., with a score of 8 or higher) were considered to be of high methodological quality. Two authors (X.J.H. and R.X.D.) evaluated the quality of each study. A third reviewer (C.L.H.) was designated to make a final decision if the initial two reviewers were unable to reach consensus.
Statistical Analysis
aOR were pooled for dichotomous outcomes from each study, and the 95% CI for each outcome was estimated to reflect the uncertainty of point estimates. We examined heterogeneity in results across studies by using chi-square test and I2 statistics. 7 The null hypothesis that the studies are homogeneous was rejected if the p value for heterogeneity was <0.10 or I2 was >50%. When substantial heterogeneity was detected, the summary estimate on the basis of the random-effects model by using the method of Der Simonian and Laird 8 was presented. Otherwise, the pooled estimate that was based on the fixed-effects model by using the inverse variance method was presented. 9 Subgroup analyses were carried out by quality grade (high compared with low), definition of macrosomia (BW ≥4 kg compared BW >4.5 kg), number of confounding factors adjusted for (<5 compared ≥5). To assess the effect of individual studies on the pooled result, we conducted a sensitivity analysis by excluding each study one by one and recalculating the combined estimates on remaining studies. We used Egger's test (linear regression method) 10 and Begg's test (rank correlation method) 11 to evaluate potential publication bias. Meta-analysis was performed with Stata/SE, version 9 (Stata Corp., College Station, TX).
Results
Identification of Studies
Electronic and manual literature searches yielded 470 results. No additional article was found in the citations of the relevant studies by manual search and 195 were excluded because of duplicates (Fig. 1); 92 articles were excluded on bias of titles, 16 studies were meta-analysis and 25 were systematic reviews, so they could not be included. The remaining 142 full text articles were selected and scrutinized. We excluded 34 articles because they were reviews and 96 studies were not met the inclusion criteria of meta-analysis. In total, 12 observational studies remained for the analysis.1,3,5,12–20
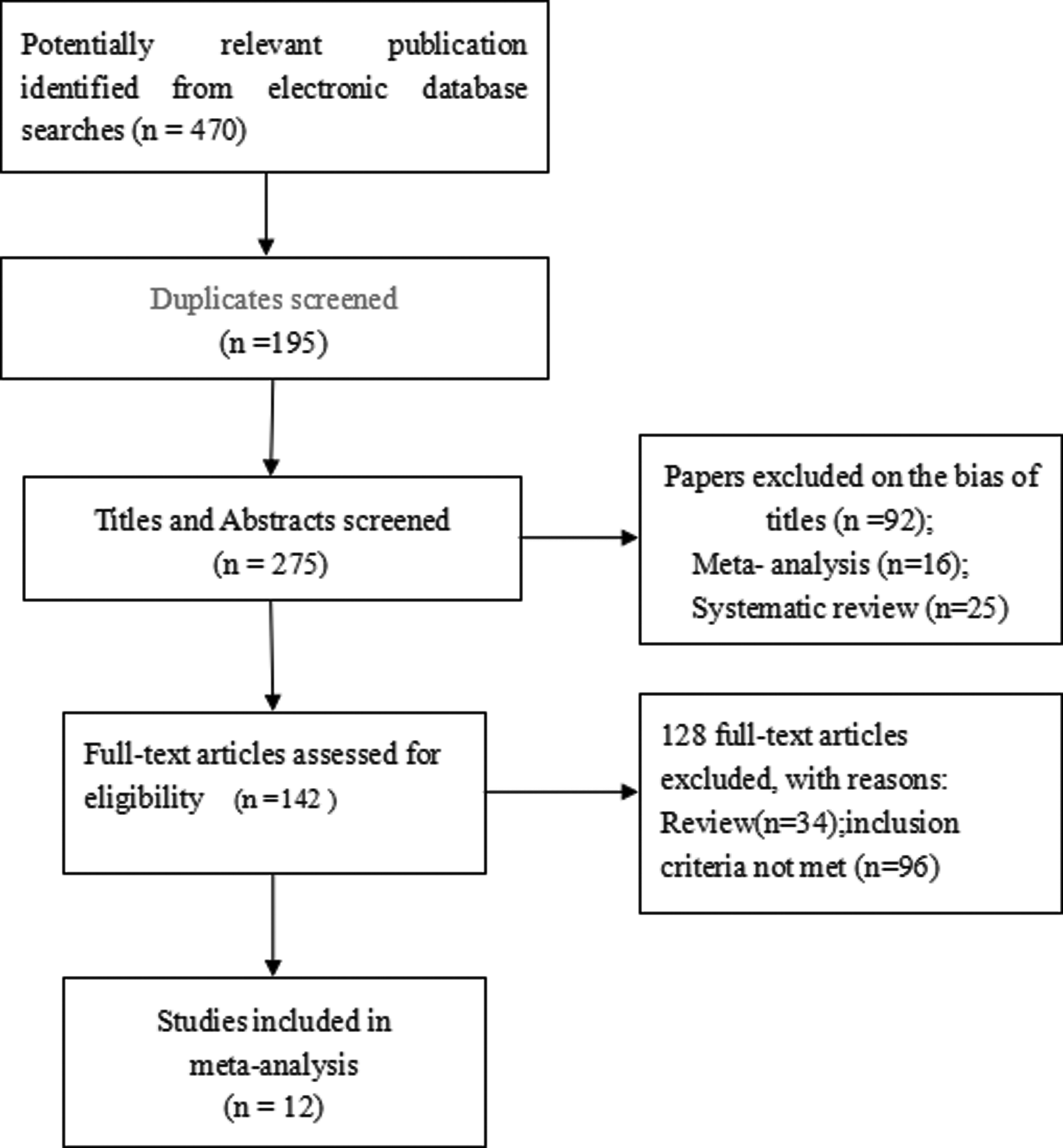
Identification and evaluation of the studies for meta-analysis.
Study Characteristics and Quality Assessment
Table 1 shows characteristics of these studies and potential confounders, for which adjustment was made. There were 12 cohort studies. Four studies were from U.S., 1 from Ireland, 1 from Malaysia, 1 from Turkey, 1 from Sweden, 1 from U.K., 1 from Norway, 1 from Israel and 1 from Cameroon. The effect of AMA on macrosomia and definition of macrosomia were also presented in Table 1.
Characteristics of the Studies That Met the Inclusion Criteria for the Meta-Analysis
AMA, advanced maternal age; aOR, adjusted odds ratio; BW, birth weight; COR, crude odds ratio.
Quality of each study, in terms of selection, comparability and exposure, is summarized in Table 2. Eight studies received scores of 8 or higher on the Newcastle–Ottawa Quality Assessment Scale and were considered to be of high methodological quality.
Quality Assessment (Grade) of Reviewed Cohort Studies
Overall Analyses
The aOR for AMA and macrosomia could be calculated for 12 studies. The homogeneity hypothesis was rejected by chi-square test (p < 0.10, I2 = 97.3%), thus the random-effect model was selected. The aOR calculated for 12 studies (compared aged 35–39 years to aged <30 years) was 1.42, 95% CI (1.25–1.60) for random-effect model (Fig. 2) and 6 studies (compared aged ≥40 years to aged <30 years) was 1.40, 95% CI (1.02–1.78) for random-effect model (Fig. 3). There was no indication of a publication bias either from the result of Egger's test (p = 0.115) or Begg's test (p = 0.115).
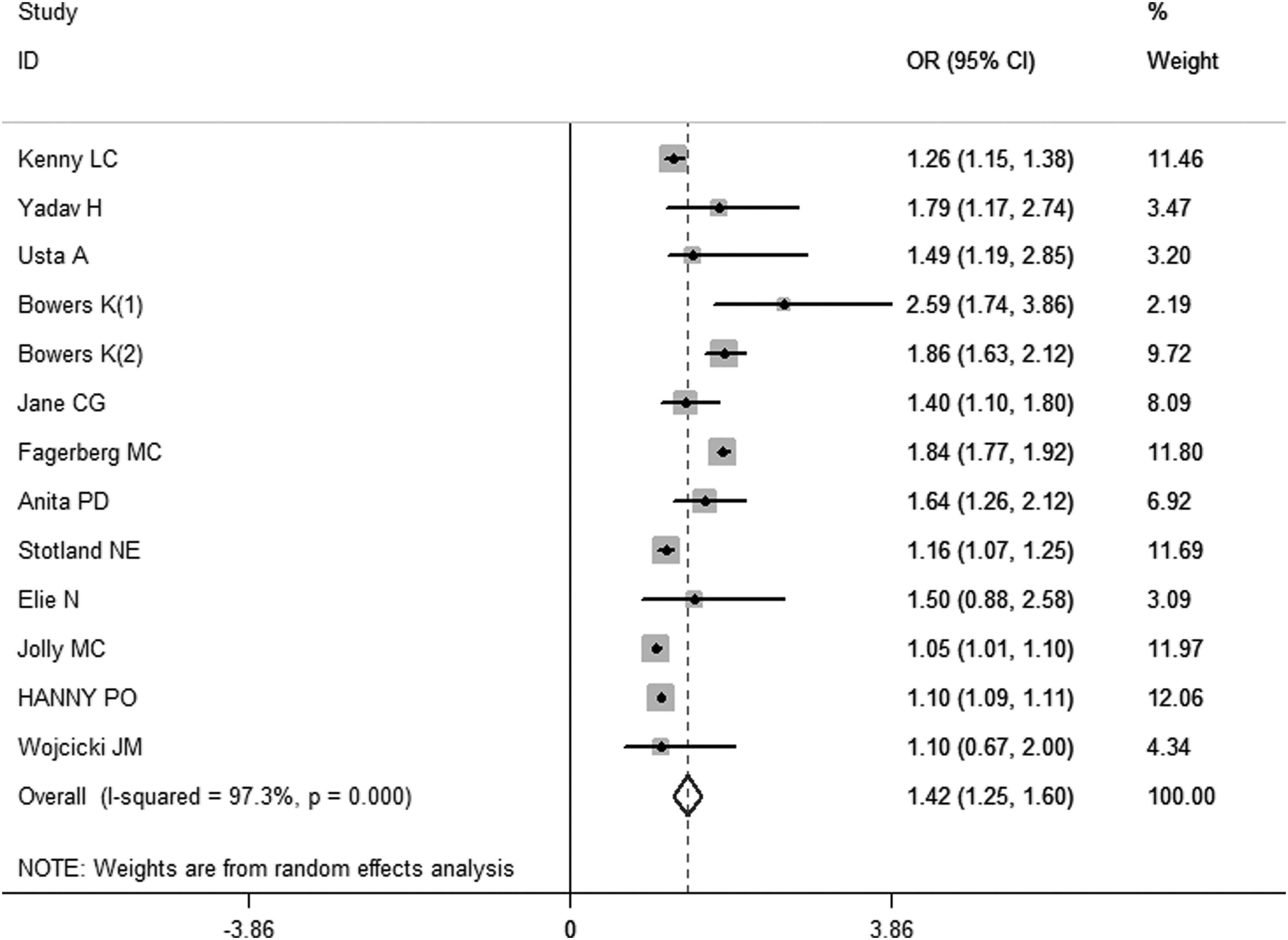
Effect of AMA on fetal macrosomia (compared macrosomia in women aged 35–39 years with women aged <30 years): covariate-aORs of 12 studies. The summary estimate on the basis of the random-effects model, aOR calculated for 12 studies (compared aged 35–39 years to aged <30 years) was 1.42, 95% CI (1.25–1.60). aOR, adjusted odds ratio; CI, confidence interval.
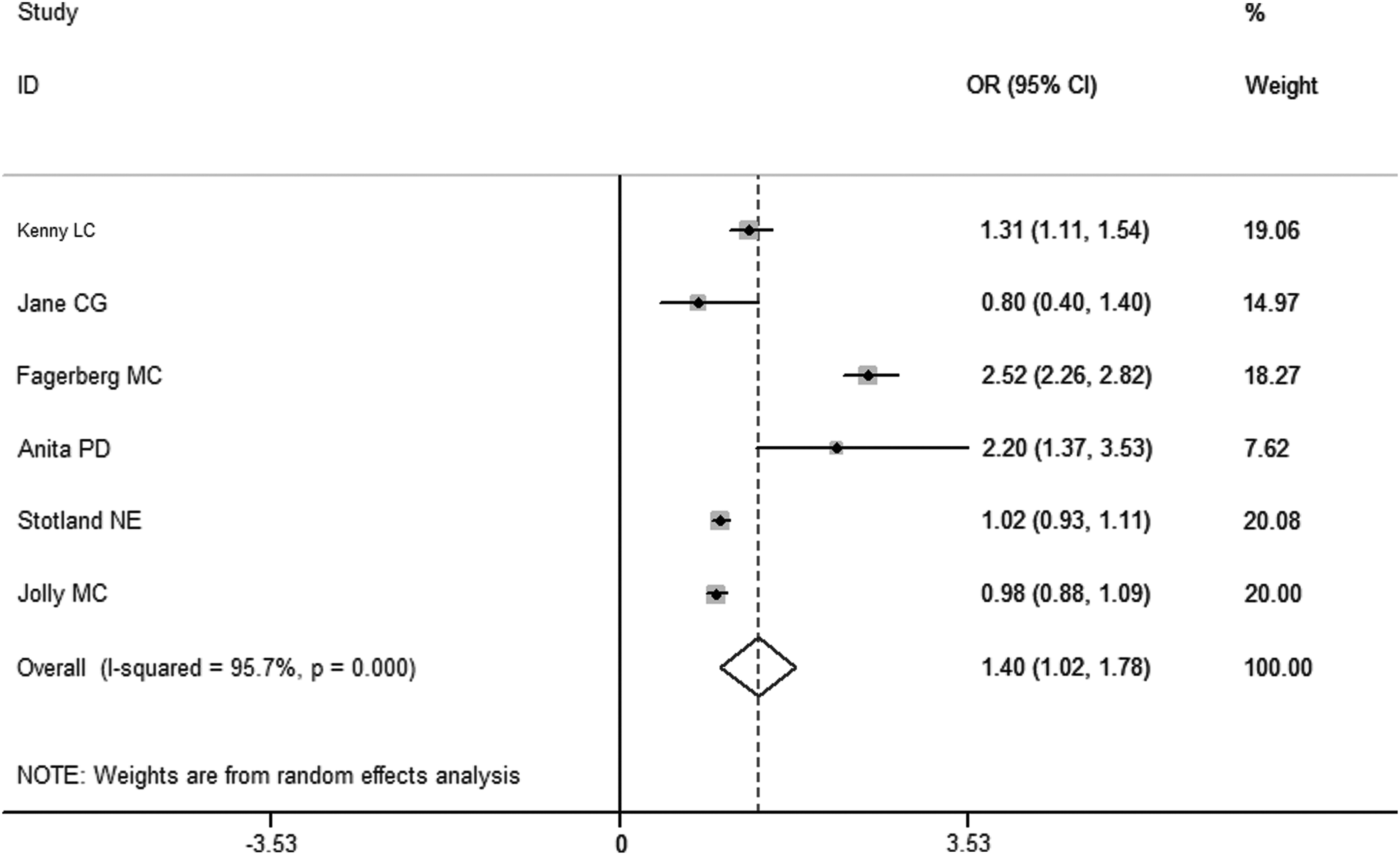
Effect of AMA on fetal macrosomia (compared macrosomia in women aged ≥40 years with women aged <30 years): covariate-aORs of six studies. The summary estimate on the basis of the random-effects model, aOR calculated for six studies (compared aged ≥40 years to aged <30 years) was 1.40, 95% CI (1.02–1.78).
Subgroup Analysis
The effects of prepregnancy obesity on macrosomia in subgroup meta-analyses are shown in Table 3. The results didn't change substantially after the analysis were stratified by some confounding factors (quality grade, definition of macrosomia, number of confounding factors adjusted for).
Subgroup Analysis of the Relationship between Advanced Maternal Age and Macrosomia
CI, confidence interval.
Sensitivity Analyses
In sensitivity analyses, we recalculated the combined results by excluding one study per iteration. The 12 study-specific aOR ranged from a low of 1.40 (95% CI: 1.22–1.57) to a high of 1.50 (95% CI: 1.25–1.74) and were similar without great fluctuation.
Discussion
A total of 12 cohort studies were included and they met the inclusion criteria of the meta-analysis. This is the first meta-analysis on this issue applying a systematic identification of relevant studies and a prospective study protocol with a focus on careful adjustment of potential confounding factors, including weight gain during pregnancy, parity and race/ethnicity. The aim of our meta-analysis was to explore the association between AMA and macrosomia. The result showed that AMA was associated with the increased risk for macrosomia.
The exact age at which adverse outcome for older mothers becomes significant is unclear. Some studies have reported that the association only becomes significant at age greater than 40 years 21 while others suggest that age 35–39 years is the cutoff for increased risk. 22 By comparing outcomes aged ≥35 years with women aged <30 years we were able to demonstrate that the association of adverse outcome with increasing age is a threshold effect, but the exact mechanism underlying the pathogenesis of adverse pregnancy outcome in older mothers is unclear. We estimated that the risk of adverse maternal and neonatal outcomes would be greater in advanced age due to placental physiological changes of aging. With advancing age, uterine blood flow decreases and utero placental under perfusion increases. Therefore, having a less efficient uterus in advanced age may independently contribute to higher risks of adverse pregnancy outcomes.
Macrosomia is most often defined in the obstetric literature using crude BW, with varying cutoff points. Four kilograms is used most frequently, which approximates to the 90th centile at 40 weeks of gestation. Definitions based upon crude BW are most appropriate when considering the effects of size on parturition. In our study, subgroup analyses were carried out by definition of macrosomia (BW ≥4 kg compared BW >4.5 kg), the results did not change substantially after the analysis were stratified by definitions of macrosomia.
The generalizability of the results should be interpreted with caution. The majority of the studies included in this meta-analysis were completed in North America and Europe, only a few studies examined the role of AMA on fetal overgrowth in women from Asia. As there are fundamental differences in nutrition, socioeconomic and educational status, and prenatal care in these regions, results may not be applicable.
Although there has been ongoing controversy as to whether or not fetal macrosomia is related to AMA, there is no meta-analysis of relevant studies, so this is the first meta-analysis on this issue. Broad search terms and multiple bibliographic databases were used in the searches to capture as many relevant articles as possible, and a robust systematic approach was used to select the final articles. In our meta-analysis, we have already suggested that AMA is associated with macrosomia, what is more, after having adjusted some potential and important confounding factors, such as pregnancy weight gain and parity, AMA is still related to macrosomia.
Conclusions
Regardless of the underlying mechanism, AMA appears to play a significant role in the development of fetal overgrowth. This finding has implication for maternity service providers, particularly as trends of AMA continue.
Footnotes
Author Disclosure Statement
No competing financial interests exist.