
Abstract
Abstract
Background:
Short sleep duration in childhood has often been linked with obesity in later childhood or adolescence. However, whether infant sleep duration affects body composition trajectories and cardiovascular health through to mid-adolescence remains unknown.
Methods:
Participants were 336 adolescents from a community-based prospective birth cohort in Melbourne, Australia. Mothers completed 24-hour time diaries, including infant sleep in 5-minute intervals at ages 2, 4, and 12 months. BMI and body composition outcomes were measured 6-monthly between 4 and 6.5 years and at 10 and 14 years. Cardiovascular outcomes at 14 years comprised blood pressure, pulse wave velocity, retinal arteriole-to-venule ratio, and carotid intima-media thickness. We used multivariable linear regression and multinomial logistic regression analyses adjusted for sex, age, BMI at birth, gestational age, ethnicity, maternal education, maternal BMI, and neighborhood socioeconomic position.
Results:
At 2 months, infants slept on average 14.1 hours [standard deviation (SD) 1.9], decreasing to 13.4 hours (SD 2.0) by 12 months. We observed no associations between the different sleep duration time points in infancy and later BMI or body composition. Moreover, a shorter sleep duration did not increase the odds of being on a high body composition trajectory compared with longer sleep (e.g., odds ratio per hour of sleep at 4 months is 0.85, 95% confidence interval 0.65–1.11). Infant sleep duration was also not associated with cardiovascular function or large or small artery structure at 14 years of age.
Conclusions:
We found no evidence that sleep duration very early in life affects adolescent body composition or cardiovascular health.
Introduction
Links between short sleep duration and obesity have been extensively studied in children and adolescents.1–3 A recent meta-analysis of prospective studies showed that short sleep duration increased the risk of later obesity by 45% in children and adolescents. 4 Mechanisms proposed to underlie a relationship between inadequate sleep and increased weight include an increased appetite, less physical activity due to tiredness, and parents possibly offering extra food when children are awake.1,4,5
Results of studies on sleep duration in very early life (i.e., infancy) on later weight development are, however, partially inconsistent. Several studies showed an association between short sleep in infancy and higher BMI up to 7 years of age,6–12 while other studies found no association.13,14 Chaput et al. concluded in a systematic review that despite this negative association in most studies, the quality of evidence remained low. 15 Studies generally used parent-estimated mean sleep duration per day, which is considered less accurate than prospective diary-reported sleep duration or sleep duration as measured with actigraphy. 16 Moreover, none of these studies has followed up beyond 7 years of age, so whether effects of short sleep duration in infancy on obesity development persist into late childhood or adolescence remains unknown.
Short sleep duration might also affect later cardiovascular health outcomes, potentially through central sympathetic mechanisms and inflammation 17 and/or the early cardiovascular health impacts of sleep-associated obesity itself. In children, the few articles that have examined relationships between sleep duration and cardiovascular health are mostly cross-sectional. A review of cross-sectional studies in children and adolescents from Matthews and Pantesco and a follow-up review by Fobian et al. showed that shorter sleep duration is often associated with higher blood pressure, while the only two longitudinal studies yielded mixed results.18,19 Furthermore, Navarro-Solera et al. reported a cross-sectional relationship of short sleep with mean arterial pressure in children 7–16 years of age with obesity, 20 but no studies have examined cardiovascular indicators other than blood pressure in a community sample.
The current study examined the prospective association of sleep duration, measured repeatedly across infancy by 24-hour sleep diaries, with BMI and body composition throughout childhood, and with cardiovascular health in mid-adolescence in a community cohort of Australian children. Furthermore, we examined whether short sleep in infancy poses a risk for being on a high BMI or fat mass trajectory from childhood onward. We expected that shorter sleep duration in infancy is associated with (trajectories of) higher BMI and fat mass and with adverse cardiovascular outcomes in mid-adolescence.
Methods
Study Design and Participants
This study drew on data from the Parent Education and Support (PEAS) Kids Growth Study, which commenced as a prospective quasiexperimental study and followed-up as a prospective community-based cohort focused on growth and cardiovascular health in Australian children. Parents provided written consent at each phase of the study. At the age of 14 years, adolescents also gave written consent. The PEAS Study and the PEAS Kids Growth Study were approved by The Royal Children's Hospital Human Ethics Research Committee (HREC 28135).
Between June 1998 and February 2000, all first-time mothers were approached when their baby was 2 weeks old in three local government areas of Melbourne (urban, suburban, and semirural) to participate in the PEAS Study. This program was a nonrandomized quasiexperimental trial, delivered through existing universal government-funded Maternal and Child Health (MCH) program visits. Both the intervention group and control group received routine visits available to all Melbourne babies throughout the first 2 years of life, namely at 2 weeks and at 2, 4, 8, 12, 18, and 24 months. Parents of the intervention group received additional advice on a wide range of common parenting problems, including cry–fuss behavior and sleep problems. At the 4- and 8-month scheduled visits, the intervention group discussed infant sleep with MCH nurses who gave guidance notes on nighttime sleep routines and simple strategies to encourage good sleep patterns. Groups were similar in baseline and end-of-trial child health and behavior, including sleep, and were therefore followed-up as a combined cohort from the age of 4 years onward in the PEAS Kids Growth Study. 21 Participating families still residing in Melbourne were invited for six follow-up visits between 4.5 and 6 years, followed by visits at 10 and 14 years.
Originally, 493 mother–child dyads were recruited, of whom 469 children completed the PEAS Study at 24 months. At the age of 4 years, 402 mother–child dyads continued to participate in the PEAS Kids Growth Study. The final sample for the current study included those with at least one assessment of infant sleep duration and one outcome assessment later in childhood (4, 6, or 10 years) or early adolescence (14 years), to keep the study sample as large as possible (n = 336). Of those, 276 children had sleep duration information available at all three assessments (82.1%). The study sample was smallest at the age of 14 years (n = 195), due to participant withdrawal or loss to follow-up (Flowchart: Supplementary Fig. S1).
Procedures and Measurements
During each wave, parents completed written questionnaires. Additionally, objective physical health measures were collected by MCH nurses from 2 weeks to 2 years (as part of their usual service), by trained researchers during home visits from 4 to 10 years, and again by researchers at a clinic visit at Melbourne's Royal Children's Hospital or home visit at 14 years of age.
Infant sleep duration
Infant sleep duration at 2, 4, and 12 months was measured with infant sleep/fuss diaries, originally developed by Barr et al. 22 At each age, parents completed a single 24-hour diary (from 8.00 am to 8.00 am) by reporting whether the infant was sleeping, being fed, awake/content or crying/fussing at each 5-minute interval over a 24-hour period.
BMI and body composition
Between the ages of 4 and 6.5 years, anthropometrics of the participants were measured every six months, and at 10 and 14 years during in-person visits in light clothes and with bare feet. Height was measured twice in centimeters (recorded to the nearest 0.1 cm) using a portable rigid stadiometer (IP0955; Invicta, Leicester, United Kingdom). The mean of two height measurements was used unless these differed by >0.5 cm, in which case height was measured a third time and the mean of three measurements was used. Weight was measured using a digital scale (4–6.5 years: Tanita TI-THD 646; 10 and 14 years Tanita BC-351, Tokyo, Japan). BMI was calculated as kg/m2 for each time point.
Body composition was measured unfasted using Bioelectrical Impedance Analysis (BIA). Measurements between 4 and 6.5 years utilized four-limb multiple frequency bioelectrical impedance analysis (MFBIA; Bodystat QuadScan analyzer; Bodystat Ltd., Isle of Man, United Kingdom). MFBIA was performed with the child lying still and adhesive electrodes applied to the right wrist, hand, foot, and ankle. The Schaefer equation was used to calculate percent fat variables from the MFBIA output. 23 At 10 and 14 years, BIA was measured unfasted using portable two-limb BIA scales (BC-351; Tanita). Percent fat is calculated by these scales using proprietary impedance equations not in the public domain. Fat mass (kg) was calculated as total weight (kg) × percent fat, whereas lean mass was calculated as total weight (kg) − fat mass (kg). Fat mass index (FMI) was calculated as fat mass (kg)/height (m) 2 , and lean mass index (LMI) as all nonfat mass (kg)/height (m) 2 .
Cardiovascular function and structure outcomes
Cardiovascular function and structure outcomes were assessed during clinical assessments at Melbourne's Royal Children's Hospital or at home at the age of 14 years. Blood pressure and carotid-femoral pulse wave velocity (PWV) were assessed using the Automated SphygmoCor XCEL device (AtCor Medical). Brachial systolic and diastolic blood pressures were measured three times to the nearest 1 mmHg, after the child had been lying down quietly for 2 minutes, with 1-minute breaks between measurements. Carotid-femoral PWV was then measured once to the nearest 0.1 m/s. Pulse transit time (seconds) was determined by the SphygmoCor XCEL as the time between the bottom of the carotid and femoral pulse waveforms with corrections made for the femoral pulse wave being measured on the thigh. The SphygmoCor XCEL calculates PWV as distance (m)/pulse transit time (seconds). 24
Equipment for macro- and microvascular structure outcomes was not available for the home visits and, therefore, only children who attended the clinic-based visit have these data available. Retinal arteriole-to-venule ratio (AVR) was measured from one of four retinal photographs taken with a digital nonmydriatic camera (CR-DGi with EDS 30D SLR camera back; CERA, Melbourne, Australia) and saved for later analysis. Retinal vascular caliber was measured from the right eye retina-centered photo using the Interactive Vessel Analysis (IVAN) software, which measures all microvessels in the half- to one-disk diameter from the optic disc. 25 The “big 6” methodology summarizes the largest six arterioles and the largest six venules as the Central Retinal Artery Equivalent (CRAE) and the Central Retinal Vein Equivalent (CRVE), respectively. 26 AVR was calculated as CRAE/CRVE. Carotid intima-media thickness (cIMT) was measured by Vivid i portable ultrasound with linear array probe for vascular ultrasound and ECG (Vivid i BT06; GE Healthcare, Buckinghamshire, United Kingdom). cIMT was measured 1 cm proximal to the carotid bulb at the R wave using automated Carotid Analyzer 6 program (MIA). These methods have been reported in detail elsewhere. 27
Covariates
Several potential confounders were identified a priori. At baseline, mothers reported child sex, date of birth, child place of birth (Australia vs. other), and highest maternal level of completed education (did not complete high school, completed high school, completed tertiary education). Gestational age and BMI at birth were retrieved from the parent-held Child Health Record, completed at birth. Neighborhood socioeconomic status was based on the socioeconomic indexes for areas (SEIFA, Index of Relative Socioeconomic Disadvantage) for the residential postcode, derived from Australian census data; the Australian national mean is 1000 [standard deviation (SD) 100], with lower scores reflecting more disadvantage. 28 Mothers reported their own height (cm), and weight was assessed at the 4-year visit, from which BMI was calculated as weight (kg)/height (m) 2 .
Statistical Analyses
Body composition trajectories from 4 to 14 years of age
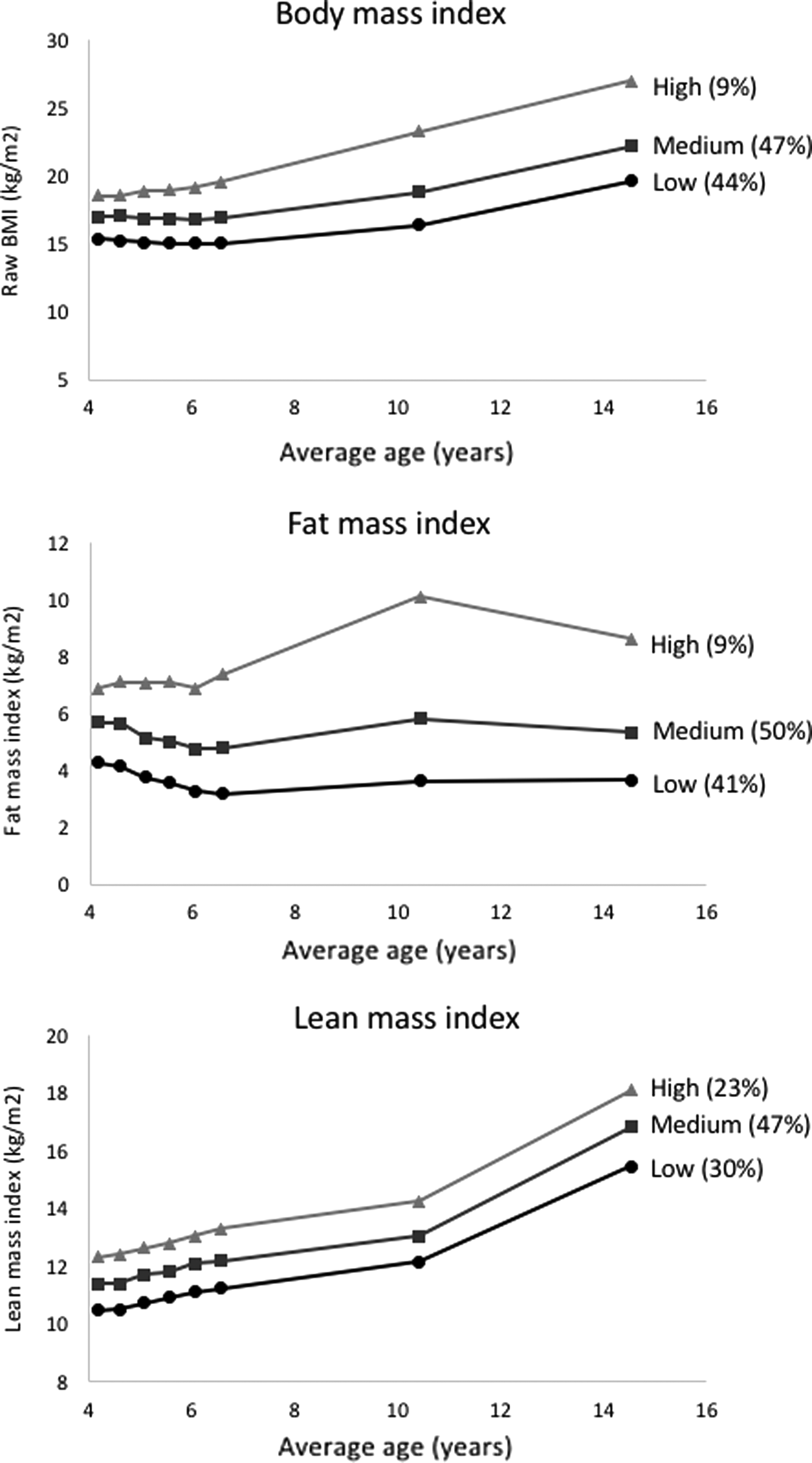
Body composition trajectories were identified for children with at least one cardiovascular outcome measured at 14 years. For each of the three separate body composition variables, latent class analysis was used to assign children to their most likely trajectory class. Model fit parameters (Supplementary Table S1) were assessed to determine the optimal number of latent classes. Model fit parameters considered included the following information criteria; the model entropy, which we aimed to maximize; the sample size of the smallest trajectory category, which we aimed to keep above 10% of the total sample; the significance of the Vuong–Lo–Mendall–Rubin likelihood ratio test; and the interpretability of the resulting trajectories. Consideration of these factors resulted in a three-class solution for all three trajectory analyses that is, low, medium, or high BMI, FMI, and LMI (Fig. 1). Latent Class Analyses were performed with Mplus version 5. 29
Associations of infant sleep duration with body composition and cardiovascular function and structure
To examine the relationship of sleep duration in infancy with body composition (ages 4, 6, 10, and 14 years) and cardiovascular phenotypic outcomes (age 14 years), multivariable linear regression analyses were conducted, adjusted for the abovementioned covariates. Second, we examined whether sleep duration in infancy was associated with trajectories of BMI, FMI, and LMI across childhood and adolescence (age 4–14 years), using multinomial logistic regression analysis adjusted for the covariates.
We checked for nonlinearity by adding a quadratic term of sleep duration in the models with BMI. Furthermore, we repeated our analyses with trajectories based on sex- and age-adjusted BMI z-scores instead of raw BMI trajectories. To include as many cases as possible, missing data on confounders were estimated by multiple imputation techniques (fully conditional specification method). All study variables were included as predictors, and results are based on pooled results of 20 datasets. Analyses were performed with IBM SPSS version 24.
Results
Sample characteristics are provided in Table 1. Most of the children included had an Australian background (87.9%), and mothers had a mean BMI of 24.6 (SD 4.7) at the 4-year visit. At the age of 2 months, children slept on average 14.1 hours (SD 1.9), and this decreased to 13.4 hours (SD 2.0) at 12 months of age. Mean BMI at 4 and 6 years was 16.5 kg/m2 (SD 1.4) and 16.3 kg/m2 (SD 1.6), respectively, increasing to 21.5 kg/m2 (SD 3.5) at 14 years.
Characteristics of the Study Sample
Characteristics are based on original data.
IQR, interquartile range; SD, standard deviation.
Table 2 shows associations between infant sleep duration at 2, 4, and 12 months and later outcomes. Overall, neither the point estimates nor the confidence intervals (CIs) suggested associations between sleep duration in infancy and later BMI, body composition, or adolescent cardiovascular health indicators (systolic and diastolic blood pressure, PWV, cIMT, and AVR).
Associations of Sleep Duration in Infancy with Body Composition and Cardiovascular Outcomes Up to Age 14 Years
All models are adjusted for child sex, age at outcome visit (trajectories are not adjusted for age) ethnicity, BMI at birth, gestational age, maternal education, maternal BMI, and neighborhood socioeconomic status.
AVR, retinal arteriole-to-venule ratio; CI, confidence interval; cIMT, carotid intima-media thickness; FMI, fat mass index; LMI, lean mass index; PWV, carotid-femoral pulse wave velocity.
None of the associations between infant sleep duration and body composition trajectories reached significance. With the low trajectory as the reference in each case, estimates were in the expected direction for all three infant sleep time points for the high BMI and high FMI trajectories, but in the opposite to expected direction for the medium BMI and FMI trajectories. For example, compared with those with shorter sleep durations, children with longer sleep duration tended to have a lower odds of being in the: (1) high BMI trajectory [e.g., odds ratio (OR) = 0.86, 95% CI = 0.69, 1.06, per hour of sleep at 12 months] and (2) high FMI trajectory (e.g., at 12 months: OR = 0.91, 95% CI = 0.74, 1.12), while (3) simultaneously having a higher odds of being in a trajectory with high LMI (e.g., at 2 months: OR = 1.30, 95% CI = 0.95, 1.75). We did not observe a quadratic relationship of infant sleep duration with subsequent BMI. Finally, analyses with trajectories based on BMI z-scores yielded similar findings: no associations were observed between sleep duration in infancy and trajectories of BMI z-scores.
Discussion
Findings from this community-based Australian study showed that 24-hour diary-reported sleep duration at three different time points in infancy was not associated with body composition and cardiovascular function and structure up to mid-adolescence, despite a weak suggestion of relationships with the highest adiposity trajectories of BMI and FMI from 4 to 14 years.
It is recommended that infants until 1 year of age sleep 12–16 hours per 24 hours. 30 Variability in infant sleep duration can be explained by individual differences in sleep need, but can also be due to parents influencing the sleep–wake cycle, for instance by set bed times, bedtime routines, and strategies used in response to night waking.31,32 In our sample, there was considerable variability in sleep duration and on average 10% of our infants slept <12 hours per day, which is comparable to the prevalence of sleep problems during infancy. 33 Despite this variation, we did not observe that short sleep duration in infancy was associated with increased adiposity across childhood.
Results of this study do not align with the mounting number of articles linking sleep duration with BMI across the life course.2,4,6,34 This may partly relate to the high quality of our infant sleep measure. Most studies have used global maternal reports of infant sleep duration, which typically overestimate actual daily sleep duration. 16 We used prospective, validated 24-hour time diaries recording sleep in 5-minute intervals, known to provide more precise estimations. 16 Although likely still less accurate than objective sleep measures, such as polysomnography or actigraphy, diaries are more feasible in larger community-based settings. In this study, parents had to report every 5 minutes what their infant was doing (sleeping, being fed, awake, and cry/fuss) over a 24-hour period. The use of these diaries for assessing patterns of crying and fussiness was validated against audiotape recordings, and showed that diaries provide valid reports. 22 Although promising, such validation is lacking for sleep estimates. However, misclassification of sleep is only problematic if the degree of sleep overestimation differs between different groups of parents (e.g., by socioeconomic or ethnic background), as this may distort the association between child sleep and BMI. Second, it might be that infant sleep only affects weight development within early or mid-childhood (the follow-up window of previous studies). However, we did not observe a relationship of infant sleep duration with BMI and body composition at age 4 years nor with trajectories of BMI from 4 years onward. Furthermore, our findings are in line with randomized intervention trials focused on improving infant sleep. These studies reported no improvement of sleep duration, or no beneficial effect on the child's later BMI status,35,36 or had only marginal impacts.37,38
Few infant sleep studies have distinguished between the outcomes of fat and lean mass, despite the assumption that short sleep is mainly obesogenic. 39 Sleep duration has been associated with a higher skinfold thickness at 3 years and fat mass levels at 6, 7, and 13 years, and an association with both fat mass and lean mass in children 3–4 years of age has also been reported.7,8,12,39–41 We did not show prospective associations of sleep duration with any marker of body composition at 4, 6, 10, and 14 years, nor did shorter sleep duration have any meaningful effect on FMI or LMI trajectories across childhood.
We did not observe an association between infant sleep and adolescent structural and functional cardiovascular outcomes. To our knowledge, this study is the first to examine such relationships from infancy. Within the adult literature, those reporting a short sleep duration had a higher risk of developing or dying from coronary heart disease (48%) or stroke (15%) compared with adults with normal sleep duration. 42 Child and adolescent studies examining sleep duration and high blood pressure are conflicting. 19 For example, in a large Chinese population, short sleep duration was only associated with higher blood pressure in 11- to 14-year-old boys, but not in girls or children at other ages. 43 Prospective studies with sleep duration in infants are scarcer. One previous study reported that infant sleep duration at age 2 months (but not at later ages up to 36 months) was inversely associated with systolic blood pressure at 6 years. 12 Plumptre et al. reported no association between sleep duration in children 12–36 months of age and systolic blood pressure in mid-childhood. 44 Perhaps shorter sleep duration only at later ages alters cardiovascular health.
This study was strengthened by the repeated use of valid, prospective 5-minute interval diaries to report infant sleep duration, its 14-year follow-up, the ability to use body composition trajectories, and detailed cardiovascular health outcomes at mid-adolescence. A necessary consequence of such precise and intensive assessments of sleep duration and health outcomes is a relatively small sample, reducing the power of the study to confirm small true associations. However, even though our CIs were not narrow, the point estimates did not suggest any meaningful associations. The number of participants in the trajectory groups may have also reduced the power to detect associations between sleep duration and body composition trajectories. This emphasizes the need for replication in larger samples. Differential loss to follow-up in less privileged participants may affect the generalizability of the results. However, 336 (68%) of the original children could be included in analyses and both predictor and outcomes showed expected variability for a community sample, suggesting that the influence of selective follow-up on our findings was minimal.
Conclusions
From this Australian prospective community-based study, we conclude that 24-hour, diary-assessed infant sleep duration was not associated with body composition or cardiovascular health from mid-childhood to mid-adolescence. Larger observational studies that accurately measure infant sleep (using actigraphy or sleep diaries) are needed to confirm whether shorter sleep duration is a risk factor for later adverse health outcomes or not. However, this study suggests that at most such effects would be small, if they exist at all. Therefore, it still seems premature to implement intervention programs that aim to increase infant sleep to prevent childhood obesity.
Footnotes
Acknowledgments
The PEAS Program was funded by the Community Division of the Victorian Department of Human Services, and the evaluation component was funded by the Australian Rotary Health Research Fund. The PEAS Kids Growth Study was funded by the Australian National Health and Medical Research Council (NHMRC) Project Grant 284509. P.W.J. was supported by the Dutch Diabetes Foundation, grant number 2013.81.1664. M.W. was supported by NHMRC Senior Research Fellowship 1046518 and Cure Kids New Zealand. A.N.G. was funded by an Australian Postgraduate Award PhD scholarship. Research at the Murdoch Children's Research Institute research is supported by the Victorian Government's Operational Infrastructure Program. The authors thank all families, investigators, staff, and students involved in earlier waves of the PEAS study and PEAS Kids Growth Study for their participation and input.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.