
Abstract
Abstract
Background:
We aimed to determine the correlation of BMI with depression and to determine the role of gender in this association, in a large study sample.
Methods:
We used the data of participants in the Iranian Children and Adolescents' Psychiatric Disorders (IRCAP) Study, conducted in 2017. This study was a national community-based, cross-sectional study in which the urban and rural areas of all provinces of Iran were covered. Overall 30,532 children and adolescents, ages 6–18, were randomly selected with the stratified cluster sampling method.
Results:
Of a total of 30,532 participants, 25,321, whose BMI had been measured and who had been interviewed with Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS), entered the study (12,455 boys and 12,866 girls). We categorized the participants according to the national cutoff points for BMI classification. After controlling for age, father's and mother's job and education, and place of residence, the odds ratio (OR) of depression in underweight, healthy weight, and overweight boys compared with obese boys was 2.19 [95% confidence interval (95% CI): 1.00–4.81], 1.06 (95% CI: 0.73–1.55), and 0.80 (95% CI: 0.49–1.32), respectively. In the girls' subgroup, after controlling for the aforementioned covariates, the OR of depression in healthy weight, overweight, and obese participants compared with underweight subjects was 1.29 (95% CI: 0.52–3.19), 1.54 (95% CI: 0.59–3.98), and 1.79 (95% CI: 0.68–4.69), respectively.
Conclusions:
Underweight boys were more likely diagnosed with depression than normal weight and overweight boys. While in girls, the probability of depression increased by increased BMI.
Introduction
Body weight and BMI undergo changes in persons with mood disorders, such that based on the DSM-5 criteria, unusual significant weight loss or weight gain (more than 5% of the body weight), poor appetite, or overeating are considered for the diagnosis of major depressive disorder. 1
However, the type and direction of the association between depression and BMI remain controversial. Some studies have revealed positive correlations between BMI and depression (increasing depression with increasing BMI). For example, Richardson et al. have reported almost two times the chance of being obese for both boys and girls with depression symptoms 2 and Ahmadi et al. have reported an odds ratio (OR) of 1.45 for obesity and overweight in women with depression compared with normal subjects. 3 Moreover, some well-designed studies have reported that both underweight and overweight are associated with depression; for instance, Geoffroy et al. in a survey among British residents, ages between 11 and 45 years, reported a higher risk of depression in persons with underweight and obesity compared with those with normal weight. 4 de Wit et al. have reported a U-shaped association in this regard. They have reported more depression symptom scores among underweight and obese subjects and fewer scores among normal weight and overweight subjects. 5 They have also proposed that this effect may be due to gender differences. Furthermore, some studies have mentioned that this association is affected by gender. An example is the study by Dragan and Akhtar-Danesh, in which they have reported that the pattern of this association is different in boys and girls. 6
While the controversy exists about the type and direction of the association between depression and BMI in adult studies, more complexities and ambiguities exist in this regard in the population of children and adolescents. Adolescence and puberty both predispose teenagers to changes in body shape, BMI, and mood. The teenagers' body shape plays a psychosomatic role in the association between BMI and major depressive disorders.
Abnormalities in BMI and mood disorders are both major public health issues; however, there are not enough well-designed and large-scale studies that focus on them. Furthermore, little has been studied about the role of gender and growing age in this association. Therefore, the aim of this large community-based study was to determine whether underweight or overweight correlates with depression in children and adolescents, and also to determine the role of the gender variable in this association.
Methods
Materials and Methods
Study design
The present study is based on the data set provided by the Iranian Children and Adolescents' Psychiatric Disorders (IRCAP) Study. 7 This study was designed by the Nutritional Neuropsychiatry group and was performed by the Psychiatry and Psychology Research Center located in Iran. This was the first national, community-based, cross-sectional study regarding the association between BMI and depression, implemented in all provinces of Iran and was financially supported by the National Institute for Medical Research Development (NIMAD).
Sampling
This study was conducted on 30,532 children and adolescents, ages 6–18 years, who had been selected from 29 provinces of Iran. On average, 1000 samples were selected from each province by the multistage cluster sampling method (cluster and stratified random sampling). One hundred and sixty-seven blocks were randomly determined in each province according to the postal codes provided by the regional post offices. In each cluster head, six samples were selected, including three girls and three boys in different age groups (6–9, 10–14, and 15–18 years; permuted-block design). Samples were gathered from the urban as well as the rural areas of the provinces (proportional to population size). More information about the methods and sampling in this study will be found in the protocol article. 8
Data collection
Houses were selected randomly by postal code and trained clinical psychologists were sent to the houses. They explained the project objectives to parents and invited them to have their children and adolescents participate in the study. On average, 8 well-trained clinical psychologists (MSc degree) in each province, and 240 in total, completed the Persian version of the Kiddie Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (K-SADS-PL) questionnaire. These psychologists were also trained to gather the accurate weight and height information. After informed consent was signed by the adolescents and the participants' parents, data about the accurate body weight and height, and information on the demographic and socioeconomic factors were collected. Then, the K-SADS-PL interview was conducted by the psychologists in collaboration with the parents and their children and adolescents.
Depression Diagnosis
Kiddie-SADS-Present and Lifetime Version
The K-SADS is a semistructured interview aimed at early diagnosis of psychiatric disorders, including affective disorders [depression disorders (major depression, dysthymia), mania, and hypomania] (21). We used the depression diagnosis method presented by the K-SADS subscale, based on the DSM-IV criteria, for analysis of major depression. This diagnostic subscale included depressive episodes lasting at least 6 months but with three to four symptoms, or depressive episodes with five or more symptoms that lasted 1–2 weeks. Based on 100 pairs of ratings, the Kappa for all K-SADS-PL definite DSM diagnoses of affective disorders was 0.93 (p < 0.001), which shows a good inter-rater reliability and agreement between interviewers. 8
BMI categories
In this study, we defined obese as ≥95th percentile of national age- and sex-specified cutoffs for BMI, overweight as ≥85th to <95th percentile of national age- and sex-specified cutoffs for BMI, normal weight as 5th to <85th percentile of national age-and sex-specified cutoffs for BMI, and underweight as <5th percentile of national age-and sex-specified cutoffs for BMI. 9
Statistical Analysis
The data collected from all the provinces were first screened for outlying amounts and these outliers were removed from the data. Then, we calculated descriptive statistics using SPSS 19 (IBM Corp., Released 2010, IBM SPSS Statistics for Windows, version 19.0; IBM Corp., Armonk, NY). Furthermore, we used the multivariable binary logistic regression analysis to predict the ORs or the probability of the occurrence of major depression in each of the categories of BMI after adjusting for covariates [the 95% confidence interval (CI) was used to estimate the precision of the OR].
Potential bias
The team administering the investigation tried to address the sources of bias from the very beginning, in the design of the study, to the end. At the design stage, we tried to decrease the selection bias via using the multistage cluster and stratified random sampling methods and via evenly distributing the main confounders such as age and sex in each cluster. At the implementing stage, we tried to reduce the information bias through using 240 trained psychologists across the country to complete the validated Persian version of the K-SADS-PL interview, based on the DSM-IV diagnostic criteria.
The sensitivity and specificity of the Persian version of K-SADS are shown to be high (the test/retest reliability of the Persian version of this questionnaire was 0.81 and the inter-rater reliability was 0.69). 10 The interviewers were also trained to explain the study process to the participants and to ensure them about the confidentiality of the information gathered to guarantee maximum collaboration from the households. Furthermore, the administrative team implemented an auditing process to inspect the interviewers via randomly contacting the samples by phone and also via sending auditors to all provinces across the country. Also the data were double-checked to validate their accuracy. In addition to using the power of random sampling in controlling unknown confounding factors, we tried to decrease the confounding bias in the analysis stage by categorizing the known confounders and also by the use of multivariate analysis.
Ethics
The consent to participate in this study was obtained from the parents of participants younger than 15 years; for participants between 15 and 18 years, consent was obtained from both the adolescents and their parents. All information about the participants and their families remained confidential. Moreover, those children or adolescents who have been diagnosed with a disorder in this study are being treated and managed, free of charge, by the child and adolescent psychiatrists who participated in the project. The NIMAD supported this study (the ethics code of NIMAD REC.1395.001).
Results
Of a total 30,532 children and adolescents, 25,321 whose BMI had been measured and who had completed the K-SADS questionnaire entered the analysis (response rate: 81.3%). The participants included 12,455 boys (mean age ± standard deviation [SD]: 11.87 ± 3.75) and 12,866 girls (mean age ± SD: 11.75 ± 3.81). Other demographic variables are listed in Table 1.
Demographic Variables in 6–18-Year-Old Children and Adolescents Who Participated in the Study on the Correlation between BMI and Depression
95% CI, 95% confidence interval.
A total of 445 participants (1.8%) were diagnosed with DSM-IV major depression, 498 (2.0%) were underweight, 14,557 (57.5%) were healthy weight, 4434 (17.5%) were overweight, and 5832 (23%) were obese (Table 2).
Prevalence of Depression and Underweight, Overweight, and Obesity among Children and Adolescents in Iran, 2017
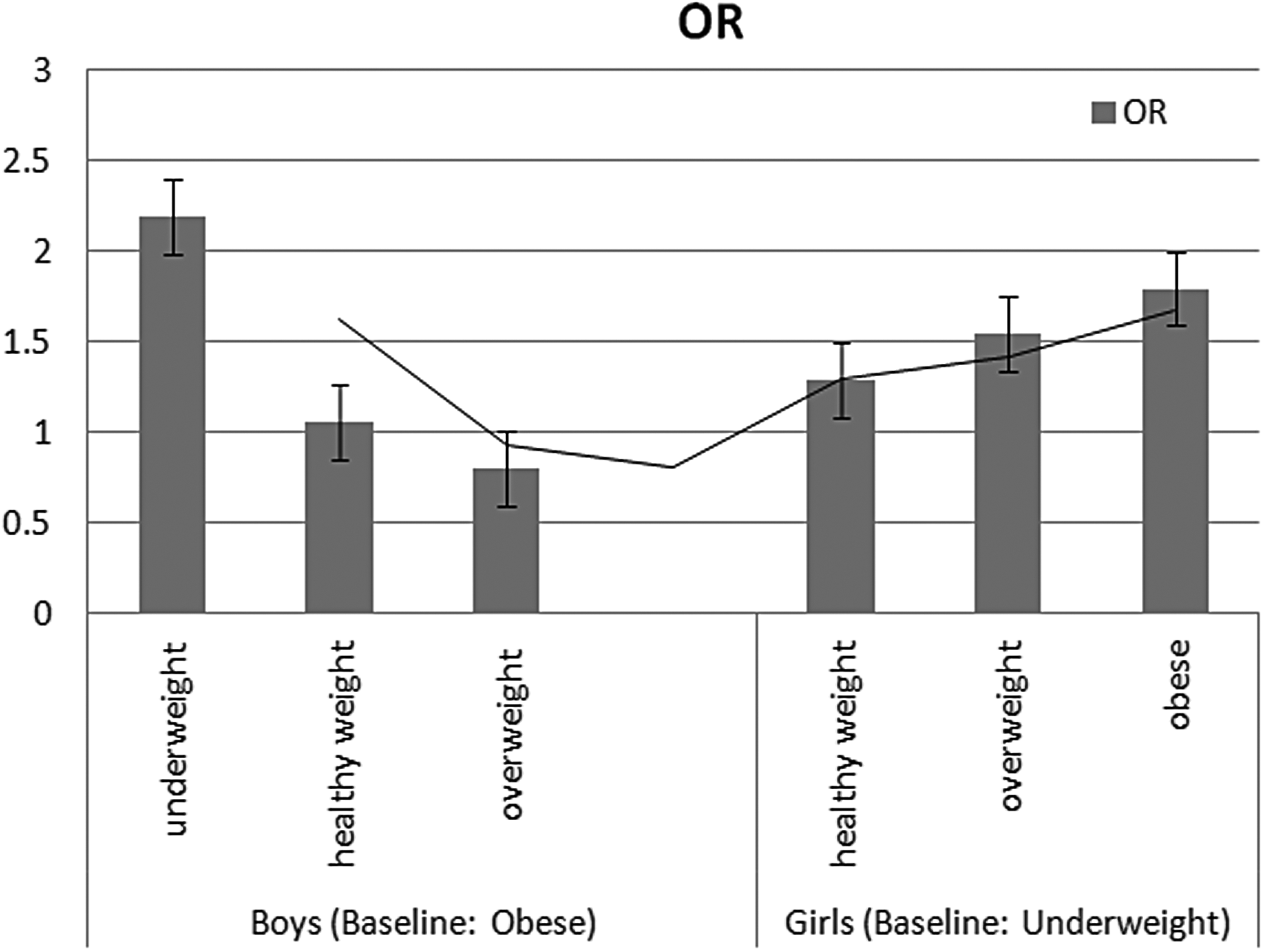
We categorized the participants according to the national cutoff points for BMI classification. 11 In boys, after controlling for age, father's and mother's job and education, and residential area, the ORs of depression in underweight, healthy weight, and overweight participants compared with obese subjects were calculated to be 2.19 (95% CI: 1.00–4.81), 1.06 (95% CI: 0.73–1.55), and 0.80 (95% CI: 0.49–1.32), respectively. In the girls' subgroup, after controlling for age, father's and mother's job and education, and residential area, the ORs of depression in healthy weight, overweight, and obese participants compared with underweight subjects were calculated to be 1.29 (95% CI: 0.52–3.19), 1.54 (95% CI: 0.59–3.98), and 1.79 (95% CI: 0.68–4.69), respectively (Table 3).
Association of Depression with BMI Categorized Based on the National Cutoff Points in Relation to Sex
The ORs calculated with the binary logistic regression analysis after adjusting for age, place of residence, and father's and mother's jobs and educational levels.
OR, odds ratio.
Figure 1 illustrates the different patterns of association between BMI and DSM-IV depression in boys and girls.
Discussion
In boys, after controlling for age, father's and mother's job and education level, and place of residence, we found that the probability (OR) of diagnosis with DSM-IV major depression increases with a decrease in BMI. While in the girls' subgroup, after controlling for the aforementioned covariates, the probability (OR) of diagnosis with DSM-IV major depression was found to increase with an increase in BMI.
Richardson et al. 2 studied the association between depression symptoms and obesity among 3101 adolescents in the United States, ages 11–17 years. They have reported that boys with higher depression symptoms had an OR = 1.95 (95% CI: 1.19–3.18) and the girls had an OR = 2.17 (95% CI: 1.25–3.77) for obesity. The findings about the girls' subgroup were consistent with our results, but about boys we observed an inverse relationship. Also, compared with this study, our survey was performed on a larger scale and was therefore more accurate in detecting the DSM-IV depression disorder and in categorizing BMI.
Dragan and Akhtar-Danesh. 6 have reported that the pattern of this association is different in boys and girls, which is consistent with our results. However, there are differences between our findings and their results as well. They have reported that in male subjects, higher BMI was associated with greater depression. While in our study, in the obese and overweight subgroup of boys, the number of persons with depression disorder was fewer than in the normal weight and underweight subgroups. The inconsistencies may be because Dragan and Akhtar-Danesh 6 have done their research on a different population in Canada with mixed age groups, ranging from 15 to older than 65 years, and with a different method (a structural equation modeling approach). Also, they have performed their analysis with the AMOS software, which has its own limitations for estimation.
Also similar to our findings, Wild et al. have revealed gender differences in the association between depression and obesity in different ages. After a 5-year follow-up of 7808 elderly people, they reported that women were more predisposed to obesity, and that overweight was associated with a reduced risk of depression in elderly men. 12
Geoffroy et al., 4 in a well-designed cohort study of British citizens, reported that depression in males predicts underweight (OR 1.84); while in female subjects, obesity predicts depressive symptoms (OR 1.34). These findings were very similar to our results.
de Wit et al., 5 in a survey of depressive symptoms among more than 43,000 subjects, ages between 19 and 90 years, reported a U-shaped association between the two variables, with a significant difference in trends between males and females. They reached these findings using analysis of variance with polynomial contrast analysis. Our results, especially Figure 1, which have been obtained using a different methodology, approve this U-shaped association.
Carpenter et al. 13 have performed a similar study on 40,086 African American and white participants in the United States who were older than 18 years. They have reported that the association between depression and obesity is gender dependent. In women, increasing BMI was associated with increasing depression, while in men decreasing BMI was associated with increasing depression.
The DSM tries to define the signs of depression, losing weight and gaining weight. These symptoms may be because of the different reactions of boys and girls as a result of major depression. In boys with depression, appetite may decrease; and so, they may eat less food and may lose weight. 14 While girls may react differently to cope with depression; they may have an increased appetite and gain weight. 15 This difference may be explained by gender differences in brain function and hormonal change. 16 Moreover, this difference may be deepened by the psychosomatic characteristics of major depression. Underweight boys and obese girls may feel that they are not charming and not socially accepted, and so, they may feel dissatisfied with their body shape. Psychological pressures of social acceptance and self-concerns about body shape may aggravate the signs of depression.17,18
Strengths and Limitations
Some of the advantages of this study are that it was a national population-based survey, with face-to-face interviews, involving a large sample of children and adolescents. Also, the processes of auditing and inspection of the interviewers across the country, which were carried out while the study was being performed, guaranteed the validity of the data gathered. Additional to these, for the diagnosis of major depression, we used an international instrument designed to generate diagnoses of psychiatric disorders in children and adolescents, rather than simply assessing the signs. This instrument has been validated for use in Iran and was applied by trained psychologists. And finally, we used a wide assortment of sociodemographic variables, as the covariates. On the contrary, one of the limitations of our study was that weight and height were gathered based only on information provided by the parents.
Conclusion
Underweight boys were more predisposed to depression than normal weight and overweight boys, while in girls, the probability for depression was greater by increased BMI. Comparing these results with the findings of similar large-scale surveys around the world, which used different methods, various assessment tools, and different statistical analysis techniques, further supports the probability that gender has a modifying effect in the association between depression and BMI.
Suggestion
The DSM definition for a major depressive disorder includes both losing weight and gaining weight. This article, along with existing literature, suggests adding gender differences in the diagnostic criteria.
Footnotes
Acknowledgments
We thank all the families and the children and adolescents who participated in this research for their cooperation. We also thank the NIMAD (Grant No. 940906) and the Psychiatry and Psychology Research Center of Tehran University of Medical Sciences for their financial and nonfinancial support. Furthermore, we thank all the interviewers involved in the project.
Author Disclosure Statement
No competing financial interests exist.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Ethics Committee of NIMAD (the ethics code of ![]() ). The written consent to participate in this study was obtained from the parents of participants younger than 15 years (verbal consent was witnessed and formally recorded), and for participants between 15 and 18 years, written consent was obtained from both the adolescents and their parents.
). The written consent to participate in this study was obtained from the parents of participants younger than 15 years (verbal consent was witnessed and formally recorded), and for participants between 15 and 18 years, written consent was obtained from both the adolescents and their parents.