
Abstract
Background/Objective:
Understanding the influence of genetically determined ancestry may give insight into the disparities of obesity seen in different ethnic groups beginning at a very early age.
Aim:
To investigate the relationship between children's ancestral genetic proportions and excess weight at 12 months of age.
Methods:
Eight hundred twenty-one 12-month-old children were included in this cross-sectional study. Their genetic admixture was estimated using the ancestry and kinship tool kit by projecting the samples into the 1000 Genomes principal component database. Weight-for-length percentile (WFLP) at 12 months of age was categorized as <95th percentile or ≥95th percentile. Multiple logistic regression analysis was performed to calculate odds ratios (ORs) with 95% confidence intervals (CIs) for the association of admixture proportions, including European (EUR), admixed American (AMR), African (AFR), South Asian (SAS), and East Asian (EAS) populations, with WFLP categories, adjusting for maternal education, birth weight, frequency of breastfeeding, and juice consumption.
Results:
Eight hundred twenty-one children were included; WFLP <95th percentile = 671 (81.7%) and WFLP ≥95th percentile = 150 (18.3%). Crude ORs showed that the EUR admixture was protective [OR 0.45 (95% CI 0.27–0.74)], whereas AMR [OR 3.85 (95% CI 1.92–7.70)] and AFR [OR 5.70 (95% CI 2.19–14.85)] admixtures were positively associated with excess weight. After adjusting for confounding variables, only the AFR admixture was associated with WFLP ≥95th percentile [OR 7.38 (95% CI 2.31–23.59)].
Conclusions:
AFRs remain associated with early excess weight after accounting for confounding variables, suggesting that this ancestral genetic background may contribute to the differences seen in early childhood obesity.
Introduction
Childhood obesity has become a critical public health concern both in the United States and worldwide. Overall childhood obesity rates in the United States are reported at 17.8%, with a recent increasing prevalence of 13.9% in preschool-aged children.1,2 With rising rates of obesity, some racial/ethnic groups are noted to be disproportionately affected, starting at an early age.3–6
Prior studies have found rapid infant weight gain to be associated with advanced skeletal maturity, physical maturation, and earlier onset of puberty. 7 Additionally, rapid weight gain and increased weight compared with length/height and BMI for age in infancy and the first few years of life have been shown to be associated with obesity later in life,3,8–11 leading to additional health risks.
Due to significant health risks associated with early childhood obesity, risk factors across different racial/ethnic groups have been identified. Factors such as lower maternal education, higher birth weight, Hispanic ethnicity, greater than recommended weight gain during pregnancy, and increased consumption of sugar-sweetened beverages have all been positively associated with childhood obesity, while breastfeeding has been identified as having a protective effect in some studies, including our prior work, but not in other studies, including a randomized controlled trial.12–19
Most literature examining early childhood obesity focuses on children in the 2–5-year age range and uses self-reported race and ethnicity to compare differences in obesity and obesity-related risk factors across populations. While self-reported race and ethnicity do provide insight into certain cultural and environmental factors contributing to an individual's obesity risk, they are not necessarily reflective of an individual's ancestral genetic background. 20
Genetic admixture analysis is a means of estimating one's ancestral genetic background and can be used to assess the influence of genetic makeup on health outcomes. In children, the genetic admixture has been used to assess differences in bone mineral density, body composition, and insulin resistance syndromes.21,22 There are several studies in the adult population that examine the relationship between genetic admixture and obesity. In these studies, the AFR admixture has been associated with higher BMI, while EUR admixture was found to be protective.23–25
Little, however, is known about the influence of the genetic ancestral admixture on early childhood obesity. This information would allow further understanding of genetic contributions to individual variations observed in obesity, possibly allowing targeted and personalized anticipatory guidance to reduce obesity in the future. Using Inova's First 1000 Days of Life and Beyond longitudinal cohort, our study aimed to assess the influence of genetic admixture on early childhood obesity at 12 months of age.
Methods
Study Design
Inova's First 1000 Days of Life and Beyond Study (Western Institutional Review Board #20120204, Inova Human Research Protection Program #15-1804) is a longitudinal, childhood cohort study based at the Inova Fairfax Medical Center, the academic teaching hospital of the Inova Health System in Falls Church, Virginia. 18 Mothers were recruited during their pregnancy and informed consent was obtained by experienced research staff prenatally; protection for human subjects was provided throughout the entire study, including privacy and confidentiality of data.
Two thousand eight hundred families were recruited into this longitudinal study; of those, 1710 were at least 12 months old and were eligible to complete surveys and 1440 of 1710 had completed the 12-month survey. Children who had missing anthropometrics or genomic data were excluded. Outliers were removed for reported lengths using the interquartile range rule, as previously validated, 26 and four subjects were excluded due to medical conditions associated with disordered growth patterns (trisomy 21, Ogden syndrome, and hypothyroidism). The study reported in this article is a cross-sectional study of 821 children (Supplementary Fig. S1).
Data Collection and Measurements
Maternal prepregnancy BMI and paternal BMI were calculated using self-reported height and weight. Weight-for-length percentiles (WFLPs) at 12 months were calculated with the World Health Organization sex-specific growth charts with parent-reported anthropometrics. Weight gain during pregnancy was calculated using prepregnancy weight and admission weight at delivery. The Health and Medicine Division of the National Academies weight gain recommendations were used to determine whether mothers met the recommended weight gain for their prepregnancy BMI. 27
Data on sociodemographic factors, including maternal race, ethnicity, and education, were collected through questionnaires. Information about pregnancy complications, birth weight, gestational age, and sex was obtained from medical records. Nutritional data were collected through the use of a food frequency table (adapted from the Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System questionnaire) 28 through surveys at 6 and 12 months.
Briefly, a small amount of blood was collected from each newborn with heel stick. The samples were sent to Illumina Services for whole-genome sequencing. The ancestry of the 821 children was estimated by the ancestry and kinship tool kit 29 developed at Illumina using 17,535 reliable and common (minor allele frequency [MAF] >5%) biallelic single-nucleotide polymorphism (SNPs). Briefly, the 17,535 marker SNPs were selected from biallelic SNPs in the phase 3 dataset from 1000 Genomes 30 with an overall MAF ≥5% and are present on most of the commonly used SNP arrays. Ancestry and Kinship Toolkit (AKT) converts genotypes of marker SNPs in the samples into a numerical matrix (0,1,2 copies of the minor allele), followed by projecting the samples onto the five superpopulations [European (EUR), admixed American (AMR), African (AFR), South Asian (SAS), and East Asian (EAS) populations] in 1000 Genomes 30 principal components. The proportion of admixture belonging to each of these five superpopulations (summing up to one) was calculated for each subject.
Finally, the admixture of samples was determined by calculating the distance between a sample and the centroid of the five ancestries in the 1000 Genomes sample in the principal component analysis (PCA)-projected space.
Statistical Analyses
The binary outcome variable was defined as WFLP ≥95th (excess weight) or WFLP <95th (normal weight) percentile. Genetic admixture (continuous variable) proportions, including EUR, AMR, AFR, SAS, and EAS, are described as means and standard deviations. Distribution of genetic admixture proportions was plotted, along with the distribution of genetic admixture proportions for excess weight and normal weight children. The characteristics of the study cohort and known obesity risk factors are described as means, standard deviations, and frequencies for continuous and categorical variables, respectively (Table 1).
Characteristics and Obesity Risk Factors in the Study Cohort
Known obesity risks factors examined were birth weight, breastfeeding frequency, juice consumption, maternal education, maternal ethnicity, maternal BMI, paternal BMI, and weight gain during pregnancy. Associations between WFLP categories and known obesity risk factors were examined using the chi-square test for categorical variables and two independent samples t-tests for continuous variables (Table 2). To detect confounding variables, associations between known obesity risk factors and genetic admixture proportions were examined using the Spearman correlation and Kruskal–Wallis tests for continuous and categorical variables, respectively. Maternal education, breast milk, juice consumption, and birth weight were detected as confounding variables as per Table 2. While Hispanic ethnicity was also shown to be significantly associated with WFLP ≥95th percentile, because of the strong collinearity between maternal ethnicity and maternal education, only education was chosen.
Comparison of Risk Factors of Childhood Obesity Among Weight-for-Length Percentile <95 and Weight for Length Percentile ≥95 Children
WFLP, weight-for-length percentile.
The association of admixture proportion with WFLP categories was evaluated, regardless of study participants' race or ethnicity. To do this, five multiple logistic regression analyses were performed to calculate odds ratios (ORs) with 95% confidence intervals (CIs) for the association of each genetic admixture proportion, including EUR, AMR, AFR, EAS, and SAS, with WFLP categories, adjusting for maternal education, birth weight, frequency of breastfeeding at 6 months of age, and juice consumption at 12 months. All statistical analyses were performed using R 3.1.2 (R Project for Statistical Computing, Vienna, Austria) and SAS 9.4 (SAS Institute, Inc., Cary, NC).
Results
Eight hundred twenty-one children from 62 parental countries of birth were included; frequencies of WFLP categories were 671 (81.7%) <95th percentile and 150 (18.3%) ≥95th percentile. Figure 1 shows the first two principal components from projecting these samples onto precalculated 1000 Genomes with known ancestries. Instead of using hard thresholds to bin individuals into ancestry groups, the admixture proportions derived from their genotypes were used in the analysis in this study. The median of the genetic admixture proportion in this cohort was 0.87, 0.013, 0.01, 0.0, and 0.02 for EUR, AMR, AFR, EAS, and SAS populations, respectively. The means of EUR, AMR, AFR, EAS, and SAS genetic admixture proportions across maternal self-reported races and ethnicities are described in Supplementary Tables S1–S11.
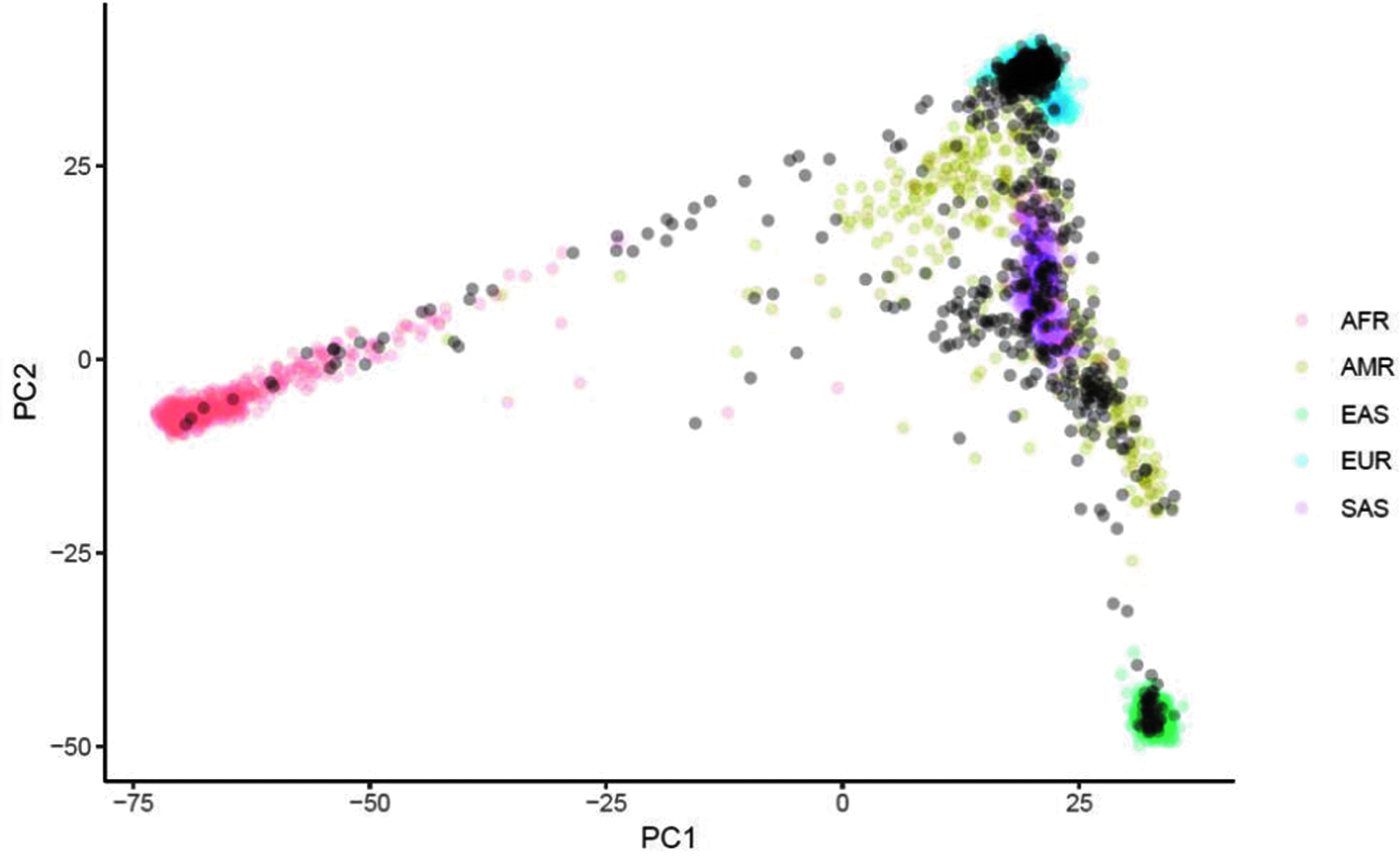
PCA plot of samples used in the study projected onto 1000 Genomes samples. PC1 and PC2 of samples used in the study projected onto 1000 Genomes samples. Samples in this study are annotated as semitransparent black circles. The 1000 Genomes samples (reference cohort) are colored by their superpopulation. The PCA plot shows the classic population structure in human studies, where the three tips represent Africans, Europeans, and East Asians. The Hispanic populations are admixed samples mostly between Europeans and East Asians. PC1, principal component 1; PCA, principal component analysis.
Characteristics of the study cohort are described in Table 1. The distribution of the admixture proportion for the study cohort is shown in Supplementary Figure S2. The admixture proportions for excess weight and normal weight children are shown in Supplementary Figure S3. Characteristics of the study cohort and risk factors for obesity were compared between excess weight and normal weight children (Table 2).
Maternal education, breast milk, juice consumption, and birth weight were detected as confounding variables. Crude ORs showed that the EUR admixture was associated with lower odds of WFLP ≥95th percentile [OR 0.45 (95% CI 0.27–0.74)], whereas AMR [OR 3.85 (95% CI 1.92–7.70)] and AFR [OR 5.70 (95% CI 2.19–14.85)] admixtures were positively associated with higher odds of WFLP ≥95th percentile. After adjusting for confounding variables, only the AFR admixture was associated with higher odds of WFLP ≥95th percentile [OR 7.38 (95% CI 2.31–23.59)], while the AMR admixture was no longer associated and the EUR admixture was no longer a protective factor. No association was observed between the EAS or SAS admixture and these two WFLP categories.
Discussion
The rising rates of obesity as well as the observed disparities among different racial/ethnic groups have been largely attributed to socioeconomic and environmental factors. Several studies have been conducted in the adult population to determine whether genetics may also play a role in risk for obesity in the current environment. This is the first study to examine the influence of the genetic admixture on early childhood excess weight at 12 months of age while controlling for known socioeconomic and environmental risk factors. Additionally, by focusing on the first year of life, it may highlight the influence of genetic contribution as there has been less exposure to environmental factors over time.
In our analysis, both AMR and AFR admixtures were associated with WFLP ≥95th percentile at 12 months of age. Conversely, the EUR admixture was noted to be protective against development of childhood excess weight. After adjusting for known obesogenic risk factors, the associations between EUR and AMR admixtures and WFLP ≥95th percentile were no longer significant, reinforcing the strong influence of social and environmental factors such as maternal education. The AFR admixture, however, remained significantly associated with excess weight, suggesting that this genetic ancestry background may more significantly contribute to the observed differences in excess weight.
In several studies conducted in the adult population, a positive association was similarly observed between the BMI and AFR admixture, while no direct association was observed between the AMR admixture and obesity.23–25 It could be speculated that those with a higher AFR proportion have differential genetic factors involved in metabolism, as suggested in studies on puberty and adults, and this may even be apparent in very early childhood contributing to early excess weight.31,32 Contrary to our findings, in a large cohort study examining the relationship between European ancestry and obesity-related traits, the EUR admixture was found to have a protective effect, even after controlling for confounding social factors. 23 This protective effect of EUR admixture was also demonstrated in a population of Native American college students, suggesting that the influence of admixture on weight may vary with age, 25 with less of an influence in very early childhood obesity.
A limitation of our study is that the anthropometrics used are parent reported, which are known to have varying reliability. While measured anthropometrics are preferred, the accuracy of parent-reported anthropometrics was improved in this study by removal of outliers, which has been previously validated in this cohort. 26 A challenge in investigating very early childhood obesity is that there is no universally accepted definition for obesity in those under 2 years of age. While there is some evidence to suggest that a high BMI in infancy may be more strongly correlated with childhood obesity than WFLP, 33 for this analysis, the recommendation from the American Academy of Pediatrics to use World Health Organization WFLP charts for children <24 months of age to identify those at risk for developing obesity was followed. 34 Moreover, in infancy after 6 months of age, there is high concordance between WFLP and BMI for age. 33
While all children included in the analysis (n = 821) had all the genetic and anthropometric data required, the larger study cohort (n = 1440) could not be used due to missing genomic and anthropometric data in addition to removal of outliers. The final sample was representative of the original participants in regard to key variables of interest from baseline questionnaires and medical records (e.g., birth weight, sex, maternal education, maternal ethnicity, maternal BMI, paternal BMI, and weight gain during pregnancy) without significant differences being observed. However, in those who did not complete the 12-month survey and therefore could not be included in the analysis, it is not possible to ascertain whether a few variables of interest were representative of the final sample due to certain data points only contained in the 12-month survey (e.g., juice consumption at 12 months).
The findings of our study emphasize the role of social and clinical factors in the prevalence of obesity and how the modern environment may have a greater influence on racial/ethnic disparities than their genetic makeup. This result is encouraging as many of the social and environmental factors are modifiable. However, it must be acknowledged that the genetic admixture could partly overlap with cultural factors associated with obesity.
While the AFR admixture continued to exhibit a statistically significant association with WFLP ≥95th percentile after adjusting for known environmental risk factors, this finding is somewhat limited by the small average proportion of AFR admixture in our study population and possible overlap of genetic admixture and cultural factors even after adjustment of confounding variables. Additional research with a larger study population should further explore the influence of the AFR genetic admixture on early childhood obesity. In addition, it cannot be excluded that the observed association between AFR admixture and 12-month obesity reflects an early growth pattern typical of AFR admixture and not necessarily a real association between AFR admixture and childhood obesity; this will be clarified in our ongoing longitudinal study. The influence of genetic admixture on childhood obesity as a child ages will also be investigated in our longitudinal study. These data, combined with social and environmental factors, will eventually allow for a more comprehensive predictive model of childhood obesity, giving the opportunity for early age, targeted, and personalized anticipatory guidance to reduce obesity rates.
Footnotes
Acknowledgments
Inova expresses its appreciation to Fairfax County, which has supported Inova's research projects with annual funding from its Contributory Fund (Fund 10030). Since its founding, Inova has been proud to be a partner with the County in providing world-class health care in the community.
Authors' Contributions
Drs. Hourigan, Niederhuber, and Ms. Fuller designed the study. Drs. Hazrati, Huddleston, Sadat-Hossieny, Tilman, Deeken, and Wong collected data, drafted the initial manuscript, and reviewed and revised the manuscript. Drs. Hazrati and Wong carried out data analyses and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding Information
All phases of this study were supported by Inova Health System.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.