
Abstract
Abstract
Purpose:
Children and adolescents affected by overweight or obesity are at risk of greater declines in self-esteem than healthy-weight individuals. Participation in multicomponent weight-management programs can positively influence self-esteem in children and adolescents affected by overweight or obesity; however, the variety of questionnaires used to assess self-esteem makes it difficult to compare changes across and identify effective interventions. This review identified and critically examined questionnaires currently used for monitoring self-esteem in children and adolescents.
Methods:
An electronic search, from 2007 onward, identified multicomponent weight-management interventions that included a measure of self-esteem. A second search identified studies that reported validation assessment of the questionnaires identified in search one.
Results:
Seven validated self-esteem questionnaires were employed across the 36 studies identified in search one, including (in descending order of use) Harter's Self-Perception Profiles for children and adolescents, Rosenberg Self-Esteem Scale, Marsh's Self-Description Questionnaire-I, Beck Youth Inventory II, Piers-Harris Self-Concept Scale, and Children and Youth Physical Self-Perception Profile. These tools measured global self-esteem (n = 1) as well as self-esteem as a series of subscales (multidimensional), such as physical appearance and social competence (n = 6).
Conclusions:
In the absence of changes in global self-esteem, multidimensional tools allow the examination of domains of self-esteem. The Harter's Self-Perception Profile for Children (SPPC) and adolescents questionnaire is an example of a tool that encompasses multidimensional aspects of self-esteem and global self-esteem and is appropriate for younger and older aged children and adolescents.
Introduction
Childhood and adolescence are critical times during which self-esteem is developed. Although a multitude of determinants (i.e., age, gender, family relations, and body weight) potentially influence self-esteem, a fairly consistent pattern emerges that self-esteem is high during childhood but dramatically drops during the transition from childhood to adolescence.1–3 The greatest drop appears to be around the age of 11–13 years, corresponding with the beginning of puberty. During early puberty, both genders experience a multitude of physical changes (i.e., greater body fat and larger hips for girls, growing taller and thinner for boys) that are at odds or are perceived to be at odds with the sociocultural norms of male and female beauty (i.e., thin for girls; muscular for boys). 4 Not surprisingly then, children and adolescents with overweight or obesity, which is also perceived to be at odds with the sociocultural norms of beauty, often experience reduced self-esteem compared with their healthy-weight counterparts.5,6 However, high self-esteem is generally supportive of better physical and mental health outcomes in the long term and is an important indicator of overall mental health and well-being.7–10
The target age group for this review was children and young adolescents aged 7–13 years. This is deemed a particularly vulnerable age group in relation to self-esteem. Although higher self-esteem is observed in young childhood, this is followed by a dramatic drop during the transition from childhood to adolescence, with several studies recording such a decline.1,2,11–13 Therefore, this is the age group when intervention is the most important to prevent further negative health outcomes and why identification of an appropriate measurement tool is vital.
Multicomponent weight-management programs, that is interventions that aim at promoting healthy eating, physical activity, and positive mental health,10,14 can positively influence self-esteem in children and adolescents.10,15–17 It is important to capture these improvements in self-esteem so that the full health impact of such programs can be determined. However, the variety of tools used to measure self-esteem in children and adolescents to date makes comparison between existing interventions and identification of effective methods for improving self-esteem challenging.14,18 In addition, not all programs that aim at improving self-esteem in children and adolescents use any scales designed to measure self-esteem.
What Is Self-Esteem?
Self-esteem has been variously defined in the literature but is taken to mean a person's overall appraisal of their worth, including how much they like, respect, and accept themselves (“How do I feel about who I am?”). 19 There are two distinctive aspects to the definition of self-esteem: First, self-esteem involves an evaluation of the self along a continuum ranging from positive to negative, with an optimum level being somewhere in the middle of this continuum; second, the evaluation of oneself includes a cognitive component (i.e., how one thinks about oneself) and an affective component (i.e., how one feels about oneself).20,21 Other terms used in the literature to denote self-esteem include self-concept, self-perception, self-worth, or self-confidence.19,22
How Has Self-Esteem Been Measured?
Typically, self-esteem is measured via self-report scales that are usually constructed and validated by psychologists and or other researchers. Although there are inherent limitations with using tools of this nature (i.e., self-report bias), the use of pen and paper self-report questionnaires remains the primary and most reliable means of ascertaining self-esteem. 23 Such tools can be used to assess either global self-esteem or domain-specific subscales of self-esteem.
Global self-esteem can be distinguished from domain-specific evaluations of the self and is defined as “the totality of the individual's thoughts and feelings having reference to himself [sic] as an object” (page 7). 24 Domain-specific evaluations include aspects such as academic competence, physical appearance, and social competence, which can be combined to give an overall global self-esteem measure. Although domains of self-esteem are found to be highly related to specific outcomes (e.g., academic self-esteem as a predictor of academic achievement), global self-esteem is more strongly related to overall outcomes such as mental health and well-being. Depending on the research target, assessments can be made of either global self-esteem or specific domains of self-esteem.
Validity of Self-Esteem Measurement Tools
The validation of a tool involves the collection of empirical evidence to demonstrate the usability of the tool to measure what it was designed to measure or, as Gable et al. puts it, does the scale do what it is intended to do?. 25 In this context, validity refers to the “appropriateness, meaningfulness and usefulness of the specific inferences made from test scores,” which, in this instance, refers to whether the scale does, indeed, measure self-esteem. 25 The Standards for Educational and Psychological Tests state that the most important consideration in the evaluation of a measure or test is its validity. 26
The aim of this scoping review was to provide a summary of self-esteem measurement tools currently used to assess changes in self-esteem in children and adolescents participating in multicomponent weight-management programs and critically appraise their validity. This review will inform researchers and interventionists of the best available evidence for assessing changes in self-esteem in children and adolescents participating in weight-management programs.
Methods
This scoping review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews (PRISMA-ScR). 27 A two-tiered approach was used to fulfill the aim of this review. The first search was carried out to identify recently conducted multicomponent weight-management interventions for children and adolescents with overweight or obesity (2007 to present) that assessed self-esteem as an outcome and reported the self-esteem measurement used. The purpose of this search was to identify self-esteem measurement tools currently being used in the setting of interest. A second search was then performed to find studies that evaluated the validity of the tools identified in search one for use in children and adolescents (no date limit), to determine how appropriate these tools were for use in the population and setting of interest.
Search Strategy One
A search was conducted in Ovid Medline, CINAHL Plus, Scopus, and PsycINFO databases up to October 2017 to identify relevant studies published since 2007 in the English language. A 10-year time frame was selected for the review to identify currently used, rather than historically used, self-esteem measurement tools. Free-text keywords were used to describe the population (children and adolescents), the intervention (multicomponent weight-management interventions), and outcome (self-esteem) (Table 1). The same terms were used to identify relevant subject headings. The criteria for inclusion were (1) child or adolescent population, including individuals aged 7–13 years who have overweight and obesity; (2) a multicomponent weight-management intervention setting; and (3) reported use of a self-esteem measurement tool. Papers were included if their population contained any individuals within the age group of 7–13 years (transition period from childhood to adolescents), for example, a study of 12–15 year olds would have been included, whereas a study of 4–6 year olds would have been excluded. Papers were excluded if the participants had comorbidities where the focus of the intervention was not general weight management (e.g., diabetes or binge-eating). Population groups were limited to Australia, New Zealand, the United Kingdom, Canada, the United States, and Europe as only tools in English were of interest. Search results were imported into Covidence (© 2018 Covidence, Melbourne, Australia). Three authors (C.B., K.D., and M.M.) independently screened titles and abstracts. Two authors (K.D. and M.M.) screened full texts to identify relevant articles.
Search Strategy for Identification of Self-Esteem Tools Used in Multicomponent Weight-Management Interventions in Children and Adolescents
Search Strategy Two
Ovid Medline, CINAHL Plus, and PsycINFO databases were searched in November 2017 to identify peer-reviewed literature evaluating the validity of the self-esteem measurement tools identified in search strategy one, for use with children aged 7–13 years. The reliability of each measure is also important and is captured in the description of each scale. For specific reliability scores of each scale, the information is provided in the Supplementary Data.
The search terms are outlined in Table 2. Included papers were (1) validation studies, (2) included children and adolescents aged 7–13 years, and (3) reporting on a self-esteem measurement tool. Studies that validated self-esteem measurement tools in languages other than English were excluded. There was no date limit on this search. Search results were imported into Covidence (© 2018 Covidence, Melbourne, Australia). Two authors (A.D. and M.M.) independently screened titles, abstracts, and full texts to identify relevant articles. A third author (M.B.) resolved any discrepancies.
Search Strategy for Self-Esteem Validation Studies
Data Extraction
Data were extracted from the studies identified in search strategy one to identify the self-esteem tools used, study population, study setting, and whether a change in self-esteem was reported. Three authors (C.B., K.D., and M.M.) independently performed data extraction. Data extracted from the studies identified in search strategy two included the study population and setting, the self-esteem tool assessed and how it was administered, the design of the validation study, and reported validity of the tool. Two authors (A.D. and K.D.) independently performed data extraction for the validity studies.
Results
Literature Search
Search strategy one
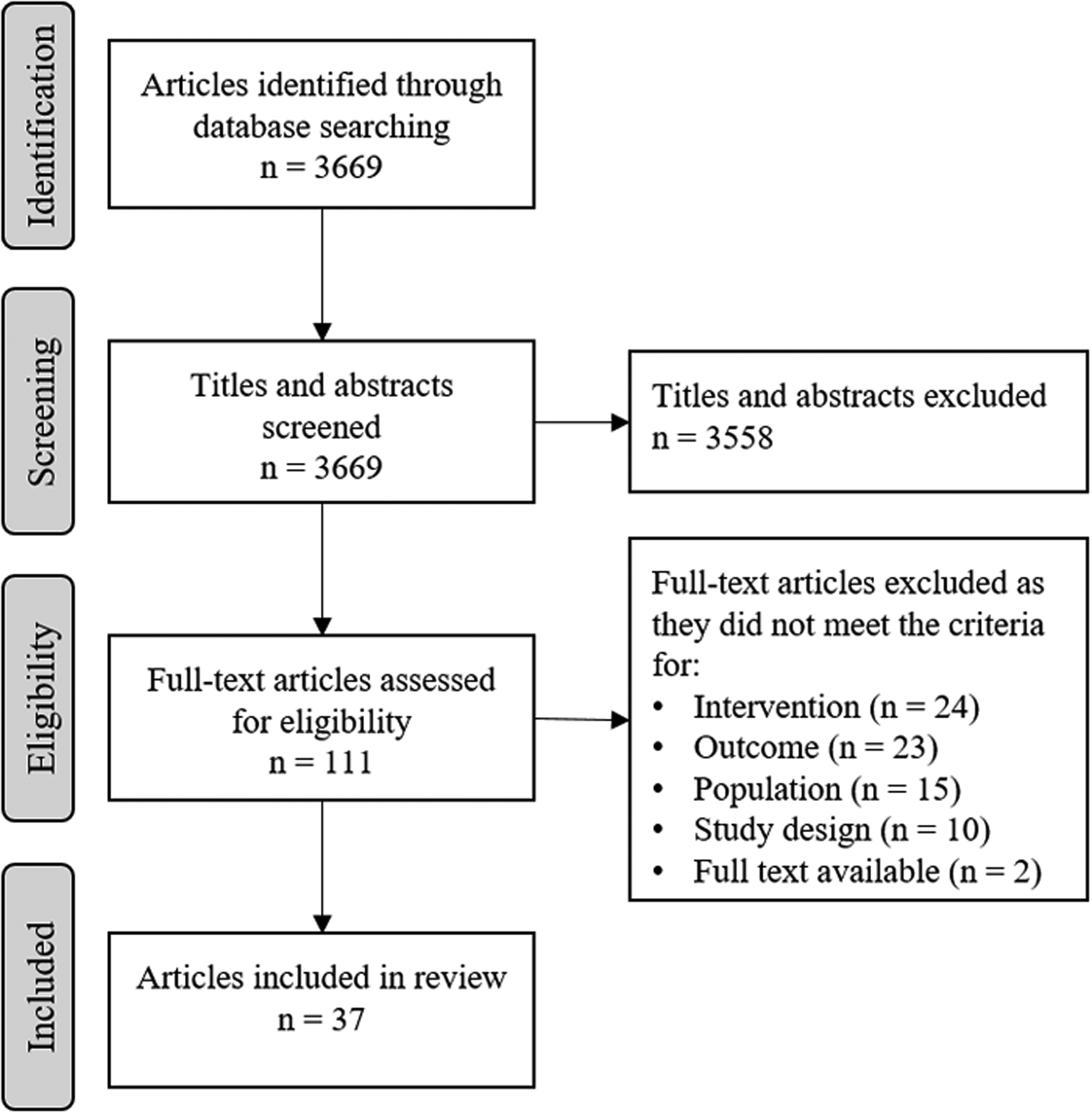
Database searching identified a total of 3669 articles. After title and abstract screening, 111 full texts were assessed for eligibility. Thirty-seven papers (representing 35 studies) met the inclusion criteria for search strategy one (Fig. 1).
Search strategy two
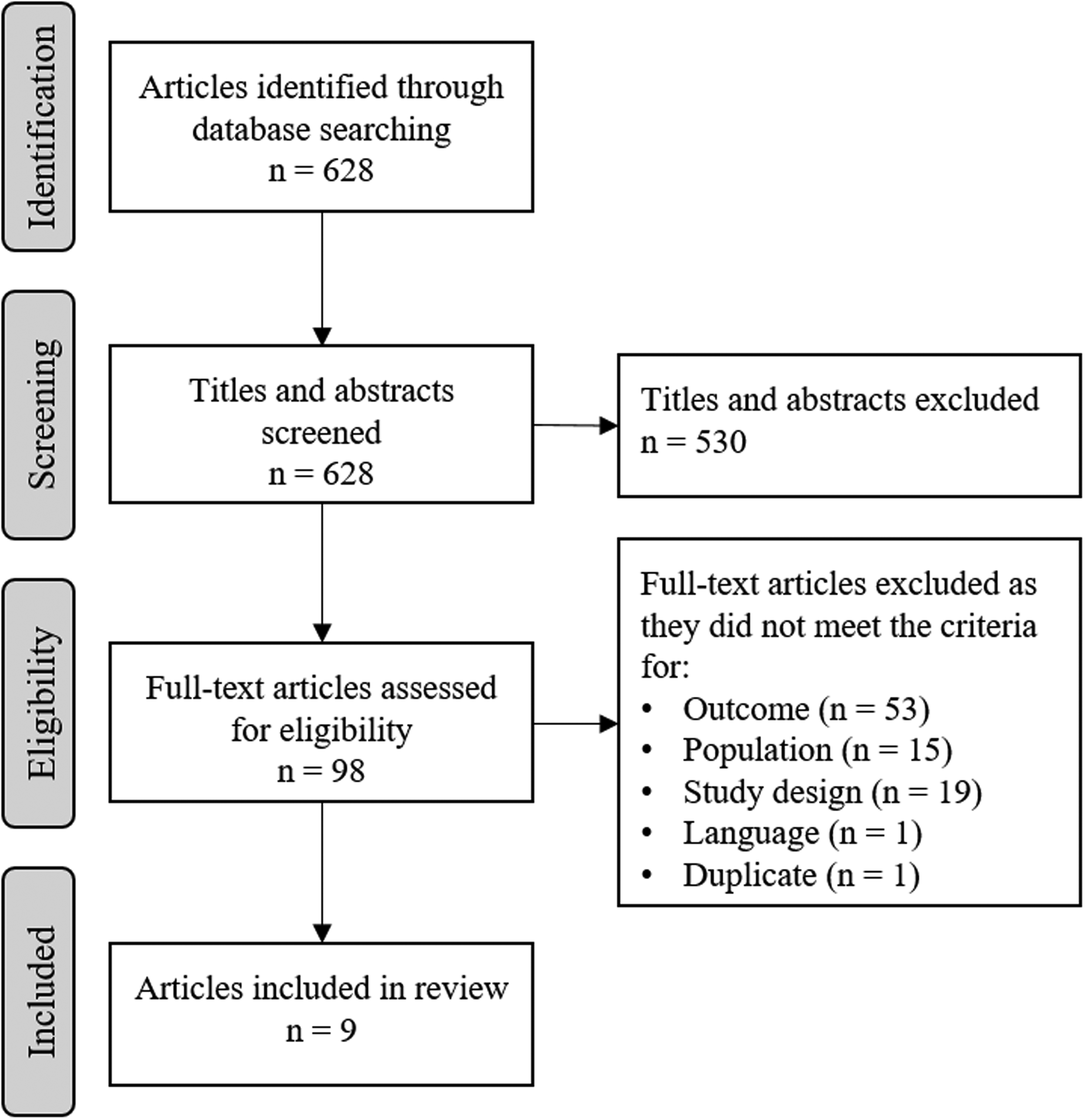
Database searching identified a total of 628 articles. After title and abstract screening, 98 full texts were assessed for eligibility. Nine papers met the inclusion criteria for search strategy two (Fig. 2).
Summary of Currently Used Self-Esteem Measurement Tools
The following summary describes measurement tools currently used to assess self-esteem in multicomponent weight-management interventions, the settings in which each tool has been used and any validity properties reported by the studies in which they were used. Seven different self-esteem measurement tools, across 35 intervention studies, were identified as being currently used in multicomponent weight-management interventions: the Harter's Self-Perception Profiles for children (SPPC) 28 and Harter's Self-Perception Profiles for adolescents (SPPA), 29 the Rosenberg Self-Esteem Scale (RSES), 30 Piers-Harris Self-Concept Scale version 2 (PH2), 31 Marsh's Self-Description Questionnaire-I (SDQ-I), 32 Children and Youth Physical Self-Perception Profile (CY-PSPP), 33 and Beck Youth Inventory II (BYI-II) 34 (Table 3). Global self-esteem was the most commonly reported outcome (n = 19), and this was most commonly reported using the RSES (n = 13). Sixteen studies reported global self-esteem in combination with other domains of self-esteem, such as physical appearance and social acceptance. The SPPC and SPPA were the most commonly used tools to report domains of self-esteem (n = 13).
Multicomponent Weight-Management Intervention Studies That Measured Self-Esteem in Children and Adolescents
M, male; F, female; NS, not stated; PSCS, Perceived Competence Scale for Children; Rosenberg, Rosenberg Self-Esteem Scale; SDQ-I, Marsh's Self-Description Questionnaire I; Piers-Harris, Piers-Harris Children's Self-Concept Scale; SPPC, Harter's Self-Perception Profile for Children; SPPA, Harter's Self-Perception Profile for Adolescents; Coopersmith, The Coopersmith Self-Esteem Inventory; CY-PSPP, Children and Youth Physical Self-Perception Profile; BYI-II, Beck Youth Self-Concept Inventory.
Among the intervention studies, 27 observed an improvement in global self-esteem or a subscale of self-esteem over the course of the intervention and one observed a reduction in global self-esteem. These observed changes indicate that the self-esteem measurement tools used in these studies (RSES n = 10, SPPC n = 8, SPPA n = 4, SDQ-I n = 2, CY-PSPP n = 1, BYI-II n = 1, PH2 n = 1) were able to identify changes in self-esteem caused by the intervention. Physical self-esteem was the most commonly reported subscale of self-esteem to show improvement after intervention, with 75% of studies that reported subscales showing an improvement in physical self-esteem (CY-PSPP n = 1, SDQ-I n = 2, SPPA n = 4, SPPC n = 5).
To assess the broad acceptability and usability of the identified tools, data were collected to determine the percentage of participants who completed the self-esteem measures (Table 3). Overall, the SPPC (55%–100%), SPPA (95.7%–100%), RSES (37.7%–100%), SDQ-I (100%), and BYI-II (100%) tools had the highest completion rates, particularly the SPPA, which is possibly due to the older age range in which it is administered. Both the PH2 and CY-PSPP tools were only used in one study, hence the interpretation of usability is limited; however, these two tools had lower completion rates of 19% and 45.8%, respectively.35,36
Harter's self-perception profile for adolescents
The SPPA is a 36-item scale that includes five subscales of self-esteem: scholastic competence, athletic competence, social competence, physical appearance, and behavioral conduct. A separate, sixth subscale, covers global self-worth (or self-esteem). 29 Five studies were identified that used the SPPA to measure self-esteem.37–41,83,84 This tool was used across community- and research-based settings in populations ranging from 22 up to 151 participants. Studies that used this tool ranged in duration from 7 weeks up to 5 months. All studies that used this tool had a population aged 13–16 years and the tool was completed by the adolescent participant. Of the five studies that used this tool, two reported on the internal consistency of the tool within their study populations. Internal consistency across the five subscales of the tool was reported as Cronbach's alpha 0.75–0.88, 38 and as 0.79–0.90, 39 which was rated as good to excellent internal consistency. One study cited a previously reported Cronbach's alpha value of 0.74–0.92. 40
Harter's self-perception profile for children
Similar to the SPPA, the SPPC is also a 36-item scale that includes subscales of global self-esteem, scholastic competence, athletic competence, social competence, physical appearance, and behavioral conduct. The SPPC was used to assess self-esteem in 11 multicomponent weight-management interventions.16,17,42–50 This tool has been used in multicomponent weight-management interventions across community, research, and primary care settings. Studies that used this tool included between 21 and 258 participants aged from 4 up to 17 years, with interventions ranging from 2 weeks to 6 months in duration. This questionnaire was completed by the child or adolescent participant, with assistance for younger children where required. Two studies using this tool reported on internal consistency within their own study populations, which were Cronbach's alpha 0.77–0.95, 48 and 0.91. 17 Four studies referred to previously reported values for internal consistency, which ranged from Cronbach's alpha 0.71–0.86.42,47,49,50 Similar to the SPPA, the SPPC has good to excellent internal consistency in the included studies.
Rosenberg self-esteem scale
The RSES is a 10-item scale that measures global self-esteem. 30 The RSES was used in 13 of the identified studies.10,15,51–61 It was primarily used in a community-based setting, but it has also been used in primary care and commercial settings. This tool has been used in study populations ranging from 19 to 13,998 participants, with ages ranging from 5 to 19 years. Studies that used the RSES had interventions ranging from 2 to 48 weeks in duration. One study that used this tool reported a Cronbach's alpha for internal consistency of 0.84 for within their study population. 58 One other study cited a previously reported value for internal consistency of the RSES, of 0.80. 10
Piers-Harris self-concept scale version 2
The PH262 is an updated version of the Piers-Harris Self-Concept Scale for Children (PH1). 63 It is a 60-item scale that assesses six subscales of self-esteem: (1) behavioral adjustment, (2) intellectual and school status, (3) physical appearance and attributes, (4) freedom from anxiety, (5) popularity, and (6) happiness and satisfaction. An overall combined score is used to assess global self-esteem. Only one of the identified studies used the PH2. 36 This study was conducted in a community-based setting and consisted of 345 participants aged 6–12 years, who participated in an 8–12-week multicomponent weight-management intervention. This questionnaire was completed by the child participants. There was no mention of any reliability or validity testing of the tool within the study population.
Marsh's SDQ
This 76-item scale measures self-perceptions relative to four nonacademic areas (physical ability, physical appearance, peer relations, and parent relations) and three academic areas (reading, mathematics, and school in general), as well as a global perception of self. 64 Two studies conducted in community-based settings were identified to have used the SDQ-I.65,66 They included 231 and 269 participants aged 9–12 years of age. The interventions lasted 12 weeks in duration. The child participants completed this questionnaire. Both studies reported internal consistency of the tool within their study populations, as Cronbach's alpha 0.81 and 0.83, respectively.65,66
Children and youth physical self-perception profile
The CY-PSPP 33 consists of 36 items related to children's physical self-perception in which six subscales are represented: global self-esteem, physical self-worth, sport competence, body attractiveness, physical strength, and physical condition. Only one community-based study used the CY-PSPP. 35 It included 84 participants aged 8–16 years who participated in a 10-week multicomponent weight-management intervention. The child/adolescent participants completed this questionnaire. There was no mention of any reliability or validity testing of the tool within the study population.
Beck youth inventory II
The BYI-II 34 includes five self-report inventories (20 questions each), of which self-concept is one. The other inventories assess depression, anxiety, anger, and disruptive behavior. The inventories can be used separately or in combination with one another. For the purpose of this review, the focus is on the self-concept inventory that measures cognitions of competence, potency, and positive self-worth. Two studies used the BYI-II to measure self-concept (self-esteem).67,68 One was a community-based 10-week intervention program, with 144 participants aged 6–17 years. The other was a 7–13-week intervention that included 17 participants with a mean age of 10.7 years (age range not reported), conducted in a primary care setting. In both studies, the questionnaire was completed by the child/adolescent participants. One study reported on the internal consistency of this tool, stating that Cronbach's alpha typically exceeds 0.86, and in their study population was 0.94, suggesting excellent internal consistency. 68
Validation of the Identified Self-Esteem Measurement Tools
All self-esteem tools included in this review have undergone some assessment of validity in children and/or adolescents, though not necessarily in an intervention setting. Where possible, information on reliability, face validity, construct validity, and content validity of the tools was collected and is detailed in Supplementary Data and summarized in Table 4. The self-esteem tools vary considerably in their length but are all considered short-form in that they can be completed in one sitting. Although the majority report a completion time of between 10 and 15 minutes, this will vary based on levels of literacy, understanding, and support required to complete the tool. Self-esteem tools specifically targeted at younger children may require additional assistance from parents or program facilitators. Table 4 summarizes the self-esteem tools identified by this review as tools currently used for measuring self-esteem in children and adolescents participating in multicomponent weight-management interventions.
Characteristics of Self-Esteem Measurement Tools Currently Used in Multicomponent Weight-Management Interventions for Children and Adolescents
RSES, Rosenberg Self-Esteem Scale; SPPC, Harter's Self-Perception Profile for Children; PH2, Piers-Harris Self-Concept Scale for Children 2; SDQ-I, Marsh's Self-Description Questionnaire; BYI-II, Beck Youth Self-Concept Inventory; CY-PSPP, Children and Youth Physical Self-Perception Profile; RA, research assistant; Y, yes; N, no.
Nine validation studies were retrieved. Three studies were conducted in Australia,22,69,70 one in the United Kingdom 71 and five in the United States,72–76 and validated tools included the RSES (n = 1), SDQ-I (n = 2), CY-PSPP (n = 1), and SPPC (n = 1). Additional validation studies retrieved in the second search that were not based on tools identified as currently used in multicomponent weight-management interventions assessed the Piers-Harris Self-Concept Scale for Children version 1 (PH1) (n = 1), Coopersmith Self-Esteem Scale (SEI) (n = 1), State Self-Esteem Scale (SSES) (n = 1), and Self-Perception Score (n = 1). Most validation studies were performed as a single testing occasion in a school or classroom setting.
Rosenberg self-esteem scale
The RSES internal reliability and construct validity was undertaken in the United Kingdom in a sample of male and female children aged 12–19 years (n = 1310). The questionnaires, including the RSES and various other measures of personal adjustment (which had established reliability and validity), were completed independently by students in a classroom setting across four schools in two working to middle-class English counties. 71 Ethnicity data were not collected. Internal consistency (Cronbach's alpha) for the 10-item RSES ranged from α = 0.81 to α = 0.88 for both male and female participants. Evidence for construct validity was demonstrated by good self-esteem being negatively correlated with the four subscales of behavioral disorders (somatic problems, hyperactivity, conduct disorder, and emotional disorder). These findings supported the reliability and validity of the RSES for use with British male and female secondary school students. 71
Marsh's SDQ
There are two studies that reported validation of the SDQ-I22,70 validity. The two Marsh reports22,70 were based on the same study that assessed male and female children aged 10 years from five suburban public schools in Sydney, Australia (n = 290). Participants were described as varied SES from working class to upper middle class (percentages and ethnicity were not reported). The SDQ-I was administered to children in a classroom setting with researchers' guidance, along with the PH1 and an older version of the SPPC called the Perceived Competence Scale for Children (PCSC), for comparison. When comparing the three tools to check construct validity, the PCSC, and the SDQ-I, factor loadings were consistently larger (median 0.75) than the PH1 scale, suggesting that these two scales more appropriately measured their intended domains. Convergent validity for the SDQ-I was demonstrated through multitrait multimethod analysis that showed high associations with similar measures and lower associations with unrelated tools. With regards to construct validity, all three tools were closely correlated with other measures of self-esteem but the SDQ-I had stronger divergent validity in that it had weaker correlation with measures of a separate construct from self-esteem.
Children and youth physical self-perception profile
The CY-PSPP was validated as a self-report form during a physical education class in a school setting in male and female students aged 8–12 years (n = 754). Schools were from predominantly middle-class neighborhoods and the majority of the children were white (70%). 76 The questionnaire was read to children and assistants circulated throughout the room to provide extra assistance where necessary. Structural equation modeling was employed to assess the factor structure of the CY-PSPP scale. Confirmatory factor analysis supported its factorial validity. The comparative fit index and non-normed fit index exceeded the 0.90 criterion in all instances, indicating an overall fit of the model to the data in each analysis. Factor loadings for the total sample, males subsample, and females subsample, respectively, were 0.69 (range 0.41–0.82), 0.67 (range 0.32–0.85), and 0.70 (range 0.43–0.83), indicating no areas of concern. 76
Harter's SPPC
The Self-Perception Score validity was examined in males and females aged 11–14.5 years, from two schools in the same district in Sydney, Australia (n = 470). Ethnicity and other demographics were not reported. Students completed the scoring independently during class time under the supervision of the researcher. Significant correlation scores were reported between the Self-Perception Score (measured from 0 to 10) and the SPPC, Beck Junior Depression, Speilberger State, and Trait Anxiety and Eating Disorder Inventory 69
Piers-Harris self-concept scale for children version 1
The PH1 was validated in male and female students in grades 4 and 7 (aged 9 and 12 years). Five schools participated from the South-western United States region and students were reported as 21% Hispanic, 75% Anglo-Saxon, and 4% other ethnic classification (n = 569). The tool was administered in a self-report format and compared with the Coopersmith Self-Esteem Scale. To test sensitivity to change, the content of the PH1 was split into two 40-item forms and 180 pupils (60% Hispanic, 22% Anglo-Saxon, and 17% Native American) divided into control and experimental groups, with the experimental group tutored for 4–6 months to improve self-concept. The PH1 and SEI were correlated to test for convergent validity. Pearson r was reported as r = 0.78 for all students, r = 0.75 for 4th grade students, and r = 0.81 for 7th grade students, providing evidence that the two scales measure the same construct. Discriminant validity was supported by weak correlations reported between PH1 and academic achievement (r = 0.18 for 4th grade students and r = 0.22 for 7th grade students); and PH1 nonsignificant correlations with ethnicity, gender, or age. 74 Internal consistency was high α = 0.92 (p < 0.001) for the total scale, α = 0.74 (p < 0.001) for the first 40-item scale, and α = 0.77 (p < 0.001) for the second 40-item scale. 74
Coopersmith self-esteem scale
The SEI is a self-report tool that was validated in a school setting in Kentucky. The questionnaire was administered by teachers who were trained in the delivery of the questionnaire. Randomly selected children were assessed twice, two weeks apart. Ethnicity was not reported. The construct validity of the tool was tested via convergent validity, discriminant validity, internal consistency, and sensitivity to change. 72 Regression and Pearson's correlation indicated the SEI had convergent validity when compared with the Piers-Harris Children's Self-Concept Scale (r = 0.63, p < 0.01) and the Children's Social Desirability Scale (CSDS) (r = 0.47, p < 0.01). Further, the SEI had discriminant validity when compared with CSDS, indicating that it does not measure the same construct and had high overall internal consistency (Cronbach's alpha = 0.86). Sensitivity to change was also acceptable, with inter-rater stability reported ranging from 0.85 to 0.97 and the inter-rater agreement being 0.86.
State self-esteem scale
The SSES was validated in 11–13 year olds from a Southeast Texas middle school. Participants were reported as 42% white non-Hispanic, 57% African American, and <1% Asian. The questionnaire was a self-report form that was completed weekly during a 6-week mandatory “Success Program” class at the school, which was designed to promote self-esteem and school success. The SSES was compared and correlated with the RSES and the Student Questionnaire and the findings provided support for psychometric properties of the scale. 73 The SSES demonstrated sensitivity to weekly changes based on participants' involvement with the success program as well as changes in self-esteem across time.
Discussion
Children and adolescents with overweight or obesity are at an increased risk of experiencing reduced self-esteem compared with their healthy-weight counterparts.5,6 Improving self-esteem in this population may help to support better physical and mental health outcomes in the long term.7–10 Weight-management programs for children and adolescents can positively influence self-esteem in children and adolescents. Through evaluations, these interventions should also be able to capture and monitor any changes in self-esteem. Unfortunately, there are few tools available to measure self-esteem and few data to support the validity of scales designed to measure self-esteem. Therefore, clinicians require to be cautious when utilizing self-esteem tools to track and measure the program's impact. The aim of this review is to provide a summary of self-esteem measurement tools currently used in weight-management programs for children and adolescents and assess their validity. Seven self-esteem measurement tools were identified as being currently used in multicomponent weight-management interventions for children and adolescents. Some key factors that differentiate the tools and are important in considering the most appropriate self-esteem measurement tool for use in weight-management programs for children and adolescents are discussed.
Validity/Reliability
All of the tools included in this review have demonstrated acceptable validity and reliability in the populations studied. However, it is important to note that all of the currently used tools were created and originally validated more than 15 years ago, raising some consideration as to whether the results are applicable and appropriate to the populations in which they are used today. For instance, language and discourse is dynamic and evolving over time. 75 It is important, thus, to reassess whether these scales still measure what they intend to measure. 25 Further, the reliability of a tool is population specific. Therefore, it is strongly recommended that intervention programs test the reliability, utility, and validity of their chosen tool in their own population group.
Multidimensional Nature
Multidimensional tools consist of subscales that measure constructs of self-esteem (such as scholastic competence, athletic competence, social competence, physical appearance, and behavioral conduct) that contribute to global self-esteem. 77 These tools can demonstrate a change in global self-esteem as well as in any individual subscale. 78 All currently used self-esteem measurement tools identified in this review demonstrated an ability to detect changes in self-esteem over time, as shown by changes in self-esteem following the multicomponent weight-management interventions. However, the evidence suggests that changes in subscales of self-esteem, as opposed to global self-esteem, occur more quickly and that changes are more likely to be observed within the time frame of a multicomponent weight-management intervention, particularly subscales related to physical appearance.14,18,42,46,48 Therefore, self-esteem tools that assess subscales of self-esteem (multidimensional) are likely to be more sensitive to changes in self-esteem than tools that only assess global self-esteem (uni-dimensional). This is in line with the literature, which appears to show an increased utilization of self-esteem tools that are multidimensional rather than uni-dimensional. 79 Further, the use of a multidimensional tool also allows investigators to monitor whether interventions may be having a negative effect on aspects of participants' self-esteem. 80 The tools identified in this review that are multidimensional are the SPPC, SPPA, PH2, SDQ-I, BYI-II, and CY-PSPP. The only uni-dimensional tool is the RSES.
Administration of the Tool
The selection of a self-esteem tool for use in interventions may rest on criteria such as ease of use and length of questionnaire, which are important considerations when selecting a self-esteem measurement tool. The language should be relatively simple so that children and adolescents, including those with poor reading skills, can understand it. Another criterion to consider is the tools' suitability for assessing individuals from diverse backgrounds. The RSES (n = 13) and the SPPC/SPPA (n = 16) were the most frequently used tools identified in this review. Both the RSES and SPPC are freely available and have comparatively low administrative burden, being 10 and 36 items in length, respectively, compared with BYI-II, which is 100 items. Although all of the tools identified in this review are considered short-form, that is they can be completed in one sitting, the RSES remains the shortest tool available to assess self-esteem, which makes it easy to administer on a large scale and is likely a reason for its popularity among intervention programs as a self-esteem measure. However, the RSES is uni-dimensional and does not assess subscales of self-esteem, which has been identified as an important aspect for tools used to assess self-esteem in multicomponent weight-management interventions.14,18,42,46,48 The SPPC/SPPA tools are also relatively short (36 items) and include measures of subscales of self-esteem, making these tools an appealing option for multicomponent weight-management interventions for children and adolescents with overweight or obesity. These findings are supported by the recent systematic review and meta-analysis by Murray et al., 14 which reported the SPPC/SPPA to be the most commonly used tools among multicomponent weight-management interventions measuring self-esteem in adolescents. Likewise, the review by Lowry et al. 18 also identified the SPPC/SPPA as commonly used tools.
Another important consideration is whether the questionnaire can be completed by the child/adolescent independently or whether support from a parent/carer is required. In this review, the only identified tool for which parental/carer assistance was required was the SPPC as it is designed for a younger group (grades of 3–7 or 8 in the American system or ages 8–15 years). 81 The SPPA, RSES, SDQ-I, PH2, CY-PSPP, and BYI-II were all designed to be completed independently. Evidence regarding the usability/acceptability of the included self-esteem tools, as found by this review, is scarce outside of the initial validation studies. Of the 36 studies identified in search strategy one that reported measuring self-esteem, none specifically commented on the usability of the tool. As a proxy measure for this, we examined completion rates of the questionnaires as an indication of the tools' usability/burden. Nineteen out of the 36 studies reported completion rates for the self-esteem measures. The RSES and SPPA had the highest completion rates (91% and 100%, respectively). The SDQ-I and BYI-II also had completion rates of 100%, however this was only observed by a single study each.65,98
Limitations
The percentage of participants who completed the self-esteem measures was used as a proxy for acceptability and usability of the measure. However, we acknowledge that this may be confounded by the context in which the measure was used. For instance, it is common that research settings allocate more resources to assuring that surveys are completed, whereas in community settings this is not the case. Likewise, in the included studies where this was reported, completion rates did tend to be higher in research settings than in community settings.
With the current societal shift away from paper-based systems and toward electronic systems, it is perhaps surprising that none of the self-esteem measurement tools identified in this review were being used electronically nor had been validated for online use. Although the use of electronic-based questionnaires would allow for easier larger scale data collection and analysis, self-esteem measurement tools would need to have their validity retested in an electronic, online setting before use, to ensure the new platform does not alter the way the tool is interpreted. The cultural background of participants is also a factor that can influence the way that self-esteem measurement tools are interpreted. 80 There can be vast differences in language use and communication style between cultures, deeming tools that have been designed in one population not necessarily transferrable to another. 80 Common issues include differences in cultural norms, dictating responses (e.g., some cultures will only respond in the affirmative so as to not disagree with the interviewer) and difference in ethnicity between interviewer and respondent. 82 When choosing a tool, it is important to consider whether the wording and administration of the tool would need to be adapted to suit the needs of children from diverse backgrounds. Once the tool is adapted, it would need to be thoroughly tested in the group of interest.
Conclusion
The measurement tools currently being used to assess self-esteem in multicomponent weight-management interventions are the SPPC, SPPA, RSES, PH2, SDQ-I, CY-PSPP, and BYI-II. All of these tools demonstrated acceptable validity for use in children and adolescents aged 7–18 years; however, evidence regarding the usability/acceptability of the included self-esteem tools is scarce outside of the initial validation studies. All studies that utilize these tools should report on the usability/acceptability of the tool in their population, as well as the reliability of the tool. The use of a multidimensional tool not only allows for the assessment of subscales of self-esteem, such as physical self-esteem, but also allows investigators to monitor whether interventions may be having a negative effect on aspects of participants' self-esteem. 80 Because of this, it is increasingly important to consider the adoption of a multidimensional self-esteem tool for use in weight-management programs for children and adolescents. Based on its validity and age-specific and multidimensional nature, this review concludes with a general recommendation of the SPPC/SPPA for assessing self-esteem in children and adolescents participating in weight-management programs.
Footnotes
Acknowledgments
This work was supported by funding from the Sax Institute Commissioning Agency—Office of Preventive Health. The funding agency had no role in the analysis, interpretation of data, writing of this article, or the decision to submit the article for publication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.