
Abstract
Introduction:
To identify longitudinal sleep trajectories in early childhood and examine the influence of sleep duration on obesity risk via BMI percentile (BMIp).
Methods:
Sleep, physical activity, and television viewing were measured in a cohort of 301 children, starting in 2001–2002, when children were 3 years and followed them through age 6. Nighttime sleep, daytime naps, and sleep duration were calculated. A series of latent growth curve models were used to estimate predictors of rate of change in sleep duration and BMIp overtime. A parallel process latent growth model examined the longitudinal relationship between sleep duration and BMIp simultaneously.
Results:
Most children (>80%) slept >10 hours per night across ages 3 to 6 years, despite the majority of children (>66%) having bedtimes after 9 pm. Sleep duration decreased on average by 0.22 (95% CI 0.20–0.24) hours each year of age (p < 0.001), while BMIp increased on average by 1.76 (95% CI 1.18–2.34) each year of age (p < 0.001). Baseline sleep duration predicted the BMIp slope factor, over and above strong effects of baseline BMIp. This indicated that greater sleep duration at baseline was predictive of decreased BMIp over time (unstandardized coefficient = −1.52 (95% CI 0.34–2.71, p = 0.012).
Conclusions:
Longer sleep duration at age 3 predicted decreased BMIp from ages 3 to 6. These findings indicate that focusing on sleep behaviors in children before age 3 may be a priority for pediatric providers with a goal of decreasing obesity risk.
Introduction
Chronic short sleep is a pervasive issue at all ages. The National Sleep Foundation reported that children are sleeping dramatically less than the amount recommended, leading to a regular state of sleep restriction. 1 Young children are at particular risk, as sleep problems are one of the most common parental complaints to pediatricians, 2 and young children are more likely to be diagnosed with a sleep disorder than any other age group. 3 Poor sleep in childhood tends to persist into adolescence and adulthood, developing into chronic sleep problems.4,5
Prior research has shown a relationship between poor sleep and obesity in children as young as 3 years.6–9 Short sleep duration has been shown to influence several important metabolic hormones, including leptin, ghrelin, insulin, cortisol, and growth hormone.10–16 Short sleep duration may also decrease metabolic rate (i.e., resting energy expenditure) and affect metabolic regulation.17–19 Insufficient sleep is thought to shift metabolism toward utilization of protein rather than fat for energy generation, processes that are associated with insulin resistance and metabolic diseases, including type 2 diabetes and obesity.
In a cross-sectional study of 7-year olds, short sleep duration (less than 9 hours/night) was associated with increased risk of obesity, and these findings were independent of television (TV) watching or accelerometry-measured time spent in sedentary activities. 20 In a cohort of >300 children 4–10 years old, obese children slept less than nonobese children and showed more variability in their sleep on the weekends, compared with school days. 21 However, the existing studies are limited by use of retrospective parented-reported sleep and cross-sectional designs, and few have investigated other key obesity-related health behaviors such as eating and activity.20–24
Of the few longitudinal studies conducted, some studies report shorter sleep duration in early childhood associated with increased weight gain and percent fat mass during later childhood, while others report no association.25–27 In a birth cohort from New Zealand (n = 244), sleep and other health behaviors were measured from age 3 to 7 years, and short sleep duration at ages 3–5 years was found to predict higher adiposity (measure via DEXA) at age 7. 27 However, in a similar study conducted in the United States with more than 800 Hispanic children ages 4–19 years, parent-reported sleep duration did not predict increased weight gain 1 year later. 25 These mixed results warrant the need for additional longitudinal studies to examine the stability of sleep during early childhood to identify optimal times to intervene to prevent the negative consequences of insufficient sleep, such as childhood obesity. The objective of this analysis was to (1) identify sleep trajectories in early childhood and (2) examine the influence of these trajectories on obesity risk. We hypothesized that shorter sleep duration during early childhood would negatively impact a child's obesity risk.
Methods
Participants
Participants in this analysis were children from a 2001–2002 prospective cohort study of healthy 3-year-old children from Cincinnati, OH. Further details regarding this study have been previously published.28–35 Participants attended study visits every 4 months for 4 years during 2001–2006. A total of 372 children enrolled, and the current analysis included 301 children with complete data from ages 3 to 6 years. The 71 children excluded from this analysis did not differ from our analytical cohort (n = 301) based on socioeconomic characteristics. The study was approved by the Cincinnati Children's Hospital Medical Center Institutional Review Board and all parents/guardians provided written informed consent. The current analysis was conducted in 2019.
Study Variables
Study visits occurred every 4 months from when the children were recruited at age 3 through 6 years for each of the 301 children included in this analysis. Data from each of the visits were aggregated by study year and the individuals' average values for sleep, physical activity, and TV viewing were used in analysis. 36 A triaxial actigraph (RT3; Stayhealthy, Inc., Monrovia, CA), worn on the hip, was used to assess physical activity and was worn for 3 days, including 2 weekdays and 1 weekend day. 31 Minutes of moderate/vigorous physical activity (MVPA) were calculated by the number of minutes >1400 counts. During the same days as the actigraph was worn, parents were asked to complete an activity diary in which the child's sleep for each of the three nights was recorded as the time the child went to bed and the time the child woke the following day. Nighttime sleep duration, daytime nap duration, and 24-hour sleep duration (nighttime sleep plus daytime naps) were calculated using the average of all 3 days.
Parents were also asked during these 3 days “how much time did your child spend watching TV or videotapes?” which was used to estimate average hours per day spent watching TV. Demographic data were collected via questionnaires completed by parents and included participant age, sex, race, and household income. Height and weight were measured during the research visit using a Health-O-Meter (Alsip, IL) electronic scale and a custom stadiometer. BMI was calculated and age- and sex-specific BMI percentiles (BMIps) were derived using the Centers for Disease Control and Prevention growth charts.
Statistical Analysis
Analyses were conducted in SAS 9.4 (SAS Institute, Cary, NC) and Mplus v8. A series of latent growth curve models were estimated to test the average rate of change in sleep duration and BMIp over time, variability in change, and predictors of the initial status factor (age 3) and the slope factor (change over time). First, separate unconditional models were estimated for both sleep duration and BMIp to examine trajectories over time in the absence of other explanatory variables. Next, conditional models were estimated to test child gender, race, MVPA, and TV viewing as potential predictors of baseline values and change over time of sleep duration and BMIp. As a final step in the model building process, we estimated a parallel process latent growth model to examine the longitudinal relationship between sleep duration and BMIp. The growth factors (e.g., initial status and slope) of each variable were simultaneously modeled to test associations between sleep duration and BMIp at baseline and over time. Of primary interest was the relationship of baseline (age 3) sleep duration with baseline BMIp (age 3) and BMIp over time (slope), although associations among all four growth parameters were estimated for completeness. This final model adjusted for child gender, race, TV viewing, and MVPA (although primary conclusions were unchanged between the adjusted and unadjusted models).
Results
The analytical cohort was 49% female, predominately white (82%) with 36% having household incomes below $50,000 (Table 1). At age 3, 21% were defined as overweight or obese and at age 6, 32% were defined as overweight or obese. Children had a similar bed and wake time across ages 3 to 6 years with the majority of children reported as having a bedtime after 9 pm (Table 2). Most children took naps at age 3 (94%), but by age 6 years, none of the children in this cohort was taking naps.
Demographic Characteristics of Cohort (n = 301)
BMI and Sleep Characteristics from Age 3 to 6 Years
Minutes of daytime naps are summarized using median (IQR). Data include mean ± SD, mean (min–max), or median (IQR).
Total sleep duration includes nighttime sleep duration plus daytime nap duration.
IQR, interquartile range; SD, standard deviation.
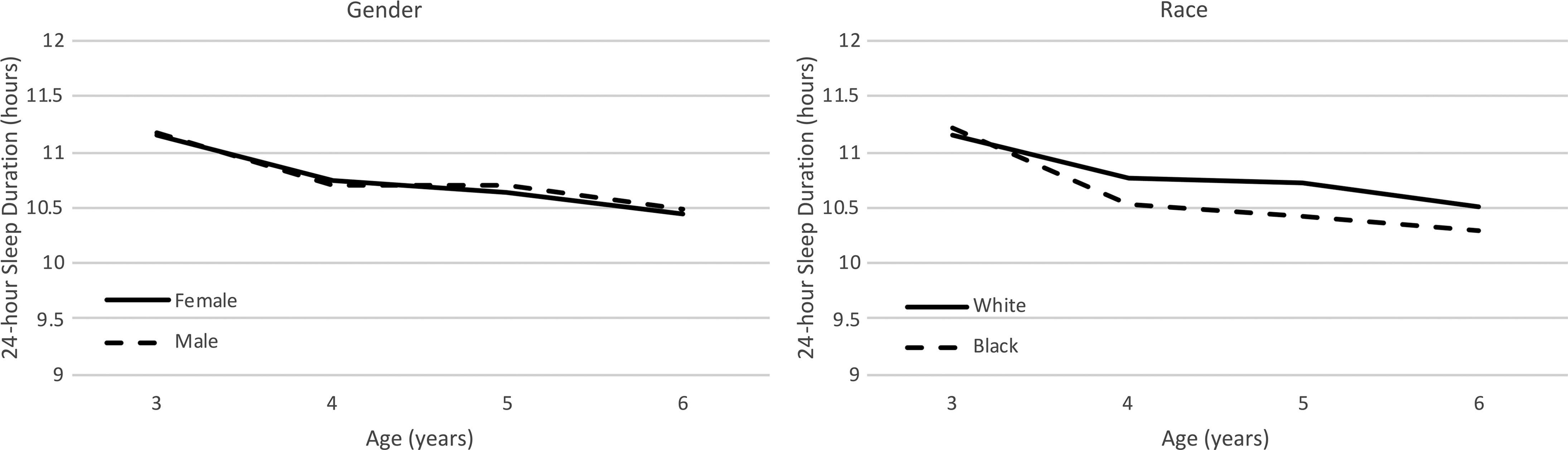
The latent growth curve model examining change in sleep duration showed a small but significant decrease over time (Table 2). At baseline, the sleep duration average was 11.2 hours and decreased on average by 0.22 (95% CI 0.20–0.24) hours each year of age (p < 0.001). Child gender did not predict baseline sleep or change in sleep over time (Fig. 1); however, children categorized as black had significantly steeper decline of sleep duration from ages 3 to 6 years compared with children categorized as white [0.08 hours steeper decrease per year of age (95% CI 0.02–0.14)]. Sleep duration (at baseline or over time) was also not influenced by MVPA or TV viewing (all ps > 0.24).
BMIp demonstrated a significant increase over time. At baseline, average BMIp was 61.1 (Table 2) and increased on average by 1.76 (95% CI 1.18–2.34) each year of age (p < 0.001). Neither baseline BMIp nor changes in BMIp over time were influenced by child gender or race (Fig. 2; all ps > 0.29). TV viewing was associated with higher BMIp at baseline [0.048 increase (95% CI 0.005–0.09) for every unit increase in TV viewing (p = 0.03) but not with changes in BMIp over time (p = 0.82)]. MVPA was unrelated to BMIp at baseline or over time (both ps > 0.33).
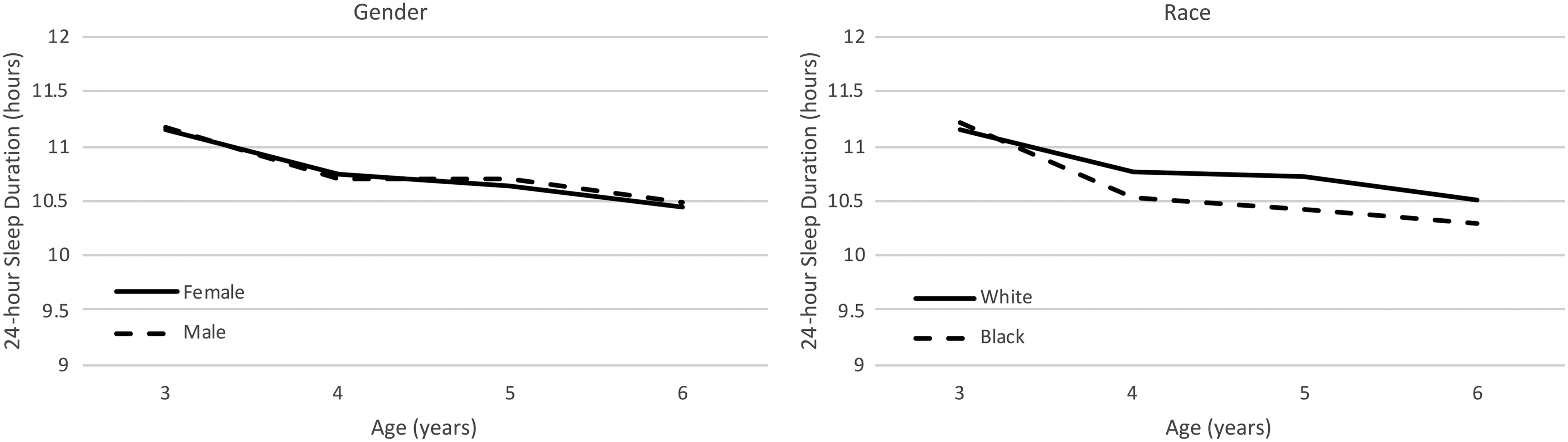
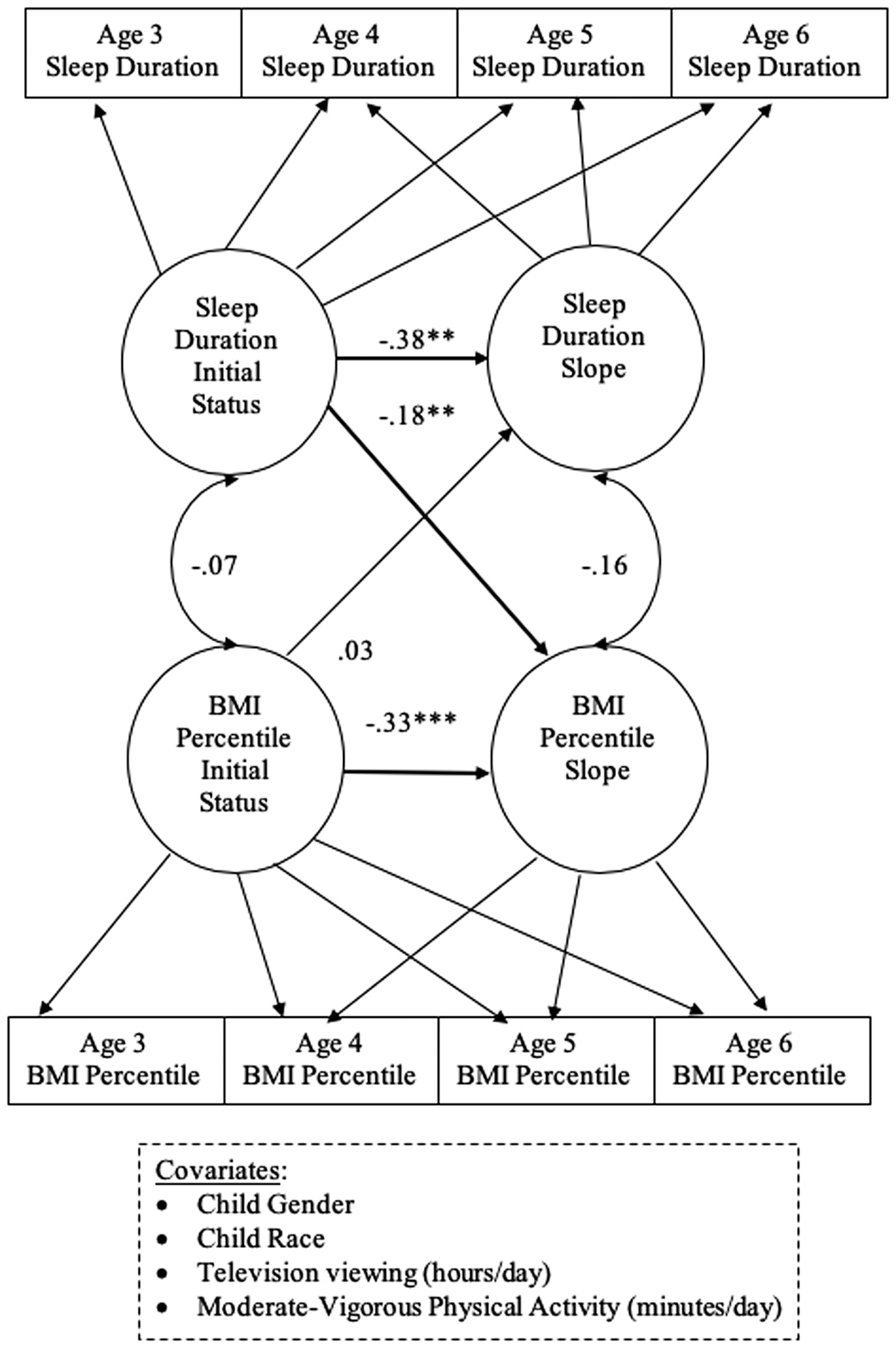
Figure 3 displays the results of the parallel process growth model simultaneously testing longitudinal relationships of sleep duration with BMIp. Standardized beta coefficients are reported so that all relationships may be examined on a common scale. Baseline (age 3) sleep duration was unrelated to baseline BMIp (p = 0.36), and change in sleep duration was unrelated to change in BMIp (p = 0.24). Consistent with study hypotheses, baseline sleep duration predicted the BMIp slope factor, over and above strong effects of baseline BMIp. This indicated that greater sleep duration at baseline was predictive of decreased BMIp over time (unstandardized coefficient = −1.52 (95% CI 0.34–2.71, p = 0.012).
Discussion
In our cohort of 301 children followed from age 3 to 6 years, we found that sleep duration significantly decreased over time by an average of 0.22 hours each year of age (i.e., 13 minutes). A child's baseline sleep duration (age 3) was predictive of BMIp changes over time, suggesting that children with higher sleep duration had a trajectory of lower BMIp over time. The children in our cohort tended to meet the minimum recommended hours of sleep for children ages 3–5 years (>10 hours/day), with only 5%–19% reported as having insufficient sleep at any given age. Although we did not see any significant differences in this decline by child gender, we did find that children categorized as the black race had a significantly steeper decline in sleep compared with children categorized as the white race.
The finding that the majority of children achieved sufficient sleep is similar to another study conducted in a white, middle class population where 87% of children ages 1–8 years met aged-based recommendations for sleep. 37 However, in a sample of low-income, African American and Hispanic children ages 3–5 years, over half (61.9%) were categorized with insufficient sleep (<10 hours/day). 38 Similarly, we found that the black race, compared with white, was a significant predictor of decreased sleep over time in our cohort.
Our findings should be interpreted with caution as they may not be representative of all young children. The cohort was not recruited with the intent to be nationally or locally representative, and due to the location of study enrollment only white and black children but no other racial or ethnic groups were enrolled. As this was a secondary analysis from a larger, longitudinal study, it was not originally designed to address the specific research questions presented in this article. Future studies should calculate a priori an adequate sample size to have sufficient statistical power to observe such an effect. In addition, the study did use rigorous methods for physical activity by using accelerometry; however, sleep variables were collected via parent report, which may be subject to bias.39,40 Strengths of our study include following a large number of children over 4 years with multiple measures of key health behaviors. Future work should be conducted to replicate our findings in a more diverse, longitudinal cohort with objective measures of sleep duration and timing.
In conclusion, we observed that longer sleep duration at age 3 predicted decreased BMIp from ages 3 to 6 years. Pediatric providers should consider focusing on sleep behaviors with their patients at a young age. Based on our findings, future interventions should be explored focusing on sleep behaviors before age 3 as a means of improving sleep and reducing obesity risk in children.
Footnotes
Funding Information
Funded by the American Heart Association Scientist Development Award (16SDG29170007; PI: J.L.K.) and the National Heart, Lung, & Blood Institute, National Institute of Health (R01 HL064022).
Author Disclosure Statement
No competing financial interests exist.