
Abstract
Background:
Overweight and obesity among children under the age of 5 have become a public health problem. The worldwide prevalence is 4.9% and 6.0%, whereas in Peru it is 7.4% and 1.9%, respectively. The causes of these problems are multifactorial and must be studied to prevent the multiple consequences on children's health.
Methods:
Secondary data analysis of the 2016 Demographic and Family Health Survey (DHS). The sample size was 7935 children and their mothers. The dependent variable was childhood overweight/obesity, measured according to the Z-score of the BMI >2 standard deviation (SD), while the main independent variable consisted of the maternal depressive symptoms (DS) (Patient Health Questionnaire-9 score >10 points). The software STATA/MP 14.0 was used for statistical analysis.
Results:
The prevalence of overweight/obesity among children aged 0–5 years was 4.5% and the prevalence of moderate and severe maternal DS was 7.1%. No maternal depressive symptoms were found to be associated with the outcome [adjusted PR = 1.36 95% confidence interval (CI) = 0.59–3.09 p = 0.47]. An association was found between socioeconomic status (SES) Q3 (adjusted PR = 3.86 95% CI = 1.9–7.6 p < 0.0001), Q4 (adjusted PR = 5.53 95% CI = 2.76–11.1 p < 0.0001), Q5 (adjusted PR = 6.9 95% CI = 3.24–14.7 p = < 0.0001), maternal BMI (adjusted PR = 1.06 95% CI = 1.03–1.08 p < 0.0001), and cesarean delivery (adjusted PR = 1.42 95% CI = 1.01–1.99 p = 0.042).
Conclusions:
No association was found between maternal depressive symptoms and overweight/obesity among children aged 0–5 years. The upper SES quintiles, maternal BMI, and cesarean delivery were associated with the outcome.
Introduction
Overweight and obesity among children under the age of five have become an important worldwide public health issue as the prevalence of only the first has increased from 4.9% to 6.0%, from 1990 until today. 1 According to the Pan American Health Organization (PAHO), 3.9 million children under the age of five are overweight and South America is one of the most affected regions with 7%. 2 The World Health Organization (WHO) has considered both problems, pandemics and estimates that about 8.6% of the children in that age group will be overweight by 2020. 3 In Peru, the prevalence of overweight and obesity was 7.4% and 1.9%, respectively. 4 These increasing figures are alarming because they are a risk factor for the development of multiple diseases.5–9
The origin of childhood overweight and obesity is multifactorial. Children factors are sex, age, amount of sleep, diet, diseases during childhood, eating habits, and physical activity, among others.10,11 The maternal factors are physiological aspects such as the BMI,12,13 gestational age, 14 or previous diseases; social aspects such as support networks or harmful habits 15 ; and mental health.
According to the PAHO, depression around the world increased 18.4% from 2005 to 2015. Therefore, there are currently 322 million (4.4%) people suffering from this disease, being more prevalent in women. 16 In Peru, the National Institute of Mental Health “Honorio Delgado-Hideyo Noguchi” found that the prevalence of depressive episodes in the adult population from Metropolitan Lima and Callao was 2.8%, being more prevalent in women as well. 17 Maternal depression affects both the mother and her child's development. The presence of the disease during and after gestation has been shown to be related to inadequate prenatal care, poor nutrition of the mother and the child, and high-risk pregnancy. Additionally, it would lead to a poor development of verbal and social abilities,18–20 behavioral disorders, psychological alterations and developmental delay.21,22 The disease would also be related to restrictive and permissive eating practices, which could cause malnutrition problems such as undernutrition or overweight/obesity.23–25 Several studies seek to determine an association between maternal depressive symptoms and overweight/obesity among children. However, no conclusion has been reached.26–28 There is no consensus in Latin America either.29,30
In addition, there are studies indicating a direct relationship between the socioeconomic status (SES) and the health status.31–33 In developed countries, the lower the SES, the more prevalence of overweight is found. However, in developing countries, overweight is more prevalent in higher SES.34,35 In Peru, a study revealed greater incidence of overweight/obesity in a high SES population, in comparison to a lower SES population. 36
These and other factors, such as the maternal BMI,37,38 were evaluated in this research to determine whether they are associated with overweight/obesity among children aged 0–5, according to the 2016 Demographic and Health Survey (DHS).
Methodology
Study Design
A secondary data analysis on a Peruvian population-based survey that took place in 2016 was conducted. The DHS, which is carried out annually nationwide, was used to find up-to-date information on different social indicators provided by the National Institute of Statistics and Data Processing (INEI). 39
Study Population and Sample
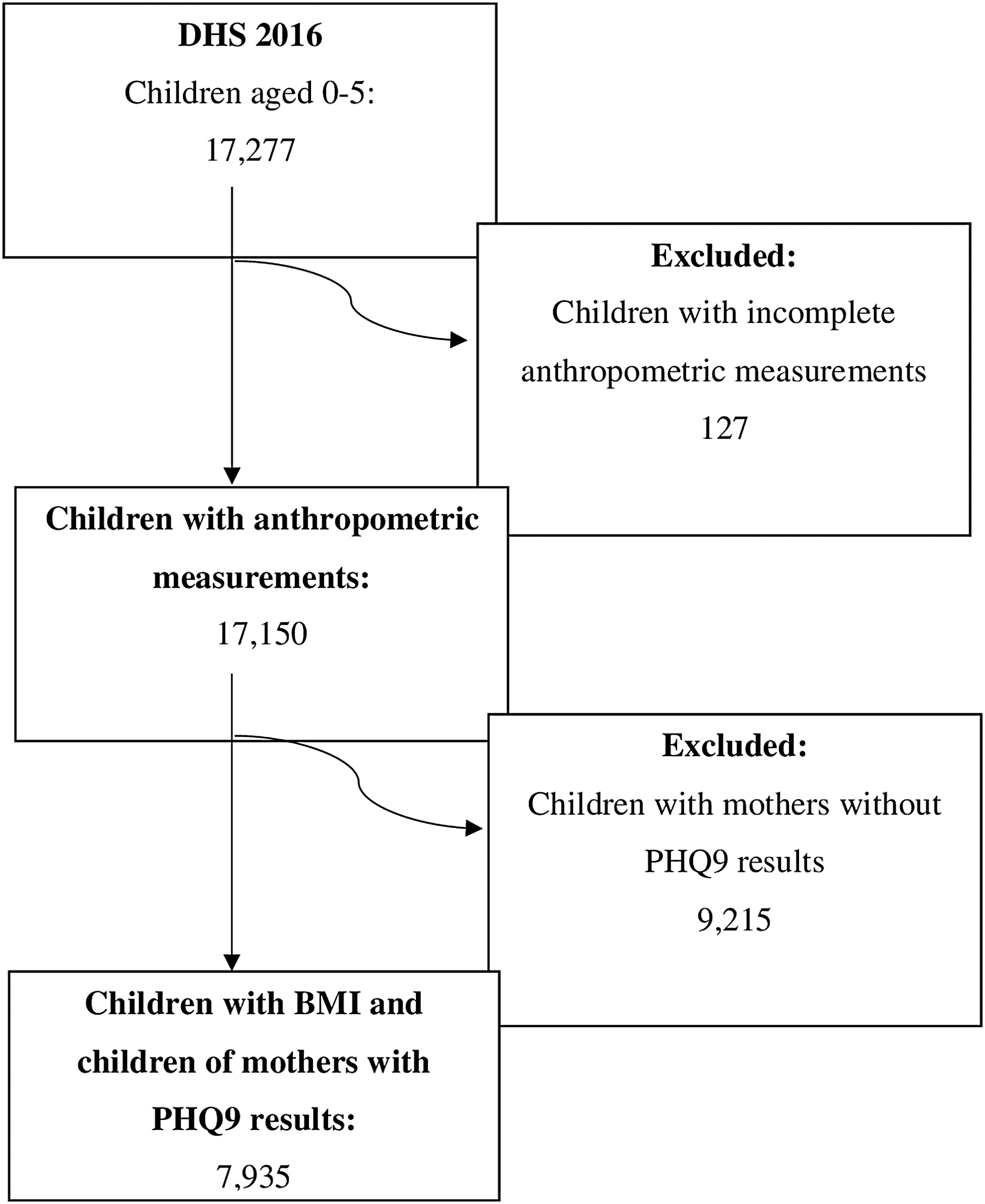
The inclusion criteria were children aged 0–5 and mothers aged 15–49 who participated in the 2016 DHS and who responded to the health, household, and individual questionnaire. The exclusion criteria were mothers who did not respond to the questions related to the Patient Health Questionnaire-9 (PHQ-9) in the health questionnaire, and children whose anthropometric measures were not complete. In the end, 7935 children and their mothers were included in this research (Fig. 1). A comparative analysis was performed between the included and excluded participants to dismiss any selection bias; however, both populations had a similar distribution according to age, sex, and other variables.
The web1.sph.emory.edu/cdckms/ website was used for calculating power. The prevalences found in a research article on the African American and Hispanic population 40 were taken as a reference. The prevalence of childhood obesity in the study population with nondepressed mothers (9%) was considered as Population 1, and the prevalence of childhood obesity in a population with depressed mothers (18%) was Population 2. Finally, we considered the complex sampling design (design effect 3), the ratio of sample sizes was 9, and a 95% confidence interval (CI) was used, resulting in a power of 91%.
Variables and Instruments
Depression symptoms (DS) were considered an independent variable and were analyzed using the PHQ-9 scale.41,42 The interviewees were rated according to the severity of DS. Scores between 0 and 9 were considered absence of DS, or minimum or mild DS levels, while scores between 10 and 27 were considered moderate, moderately severe or severe DS levels. In Chile, the PHQ-9 scale was validated in Spanish, showing 92% of sensitivity and 89% of specificity in the detection of DS in a population older than 20 years attending to psychiatrists' offices. 43 PHQ9 was also validated in Peru using the Health Questionnaire of the Demographic and Health Survey (DHS) in 2019. 44
Overweight/obesity was considered a dependent variable, for which the boy or girl's BMI Z-score was analyzed. For the final analysis, the variable was divided into “no overweight,” from −3SD to 2SD of the mean, and “overweight/obesity,” above 2SD of the mean. 45 The reason to dichotomize this variable was made so the results in this study can be compared to other articles, additionally the main objective was to determine the association between maternal depressive symptoms with overweight/obesity status in children, and not to analyze further on the obesity status by itself.
The SES was already classified by the authors of the DHS in an index including five quintiles, each of them representing a level of wealth, where Q1 refers to the poorest population while Q5 refers to the wealthiest.46,31 Furthermore, there were other co-variables: age of the mother, marital status, maternal education, maternal BMI, origin, tobacco use, diabetes mellitus, hypertension, sex of the child, age of the child in months, and birth weight of the child in grams, among others.
Data Collection
The collection of data from the 2016 DHS was performed during the two semesters of the year. The collection technique was a direct interview to women aged 15–49 from the homes selected. The people in charge of measuring children's height and weight were widely experienced in anthropometric measurement techniques and passed the evaluation of the National Center for Food and Nutrition (CENAN) from the National Institute of Health (INS). They performed a double anthropometric measurement after the quality control of height rods and weighing scales. 47
Data Analysis
Statistical comparisons were made among the survey participants with the statistical data analysis software STATA MP 14.0 (Statacorp, TX). For all the analyses, the complex structure of the sample was considered (svy command).
For the univariate analysis, proportions were calculated for the categorical variables and measure of central tendency and dispersion measures for the numerical variables. The bivariate analysis of categorical variables was performed with the Chi-square test and for the numerical variables, Student's t-test. For the multivariate analysis, variables with a p < 0.2 were considered and the Poisson regression with robust variance was used. The crude and adjusted prevalence ratio (PR) was calculated with 95% CI. To analyze the results, the value of p < 0.05 will be taken into account.
Ethical Aspects
The DHS study has a de-identified public database, available at www.inei.gob.pe. This research was approved by the Ethical Committee of the Universidad Peruana de Ciencias Aplicadas.
Results
Table 1 shows the prevalence of children aged 0–5 years with overweight and obesity (4.5%) in addition to the other characteristics of the children (Table 1). Of the mothers who completed the PHQ-9 questionnaire, only 7.1% had moderate/severe depressive symptoms. The rest of the maternal characteristics is presented in Table 1. No association between maternal depressive symptoms and childhood overweight/obesity was found on the bivariate analysis (Table 2).
Characteristics of Children Aged 0–5 Years and Their Mothers in the 2016 ENDES (n = 7935)
Standard error/average.
Factors of the Child and Their Mother Associated with Overweight/Obesity
Average (standard error).
For the adjusted analysis, the variables that had a p < 0.2 in the crude analysis were used. Only statistically significant association was found in the BMI variables of the mother (adjusted PR: 1.06 p < 0.0001), SES (Q3 aPR 3.86 p < 0.0001 Q4 aPR 5.53 p < 0.0001 Q5 aPR 6.9 p < 0.0001 95% CI), and type of delivery (PR: 1.42 p = 0.04). There was no association with the other maternal variables such as depressive symptoms, marital status, origin, hypertension, and diabetes. Similarly, no association was found with the rest of the children's variables (Table 3).
Association between Maternal Depression and Overweight/Obesity Crude and Adjusted Models
Poisson regression analysis was used with robust variance.
aPR, adjusted prevalence ratio; CI, confidence interval; cPR, crude prevalence ratio.
Multiple sensitivity analysis were performed considering different PHQ-9 cutoff points (5,10,15); however, no association between depressive symptoms and overweight/obesity in children were found with any of those.
Discussion
The main finding of this study is that the prevalence of overweight/obesity in children of this age range is 4.5%, while the prevalence of moderate and severe depressive symptoms in mothers is 7.1%. In this article, no significant association was found between these two variables, but between the overweight/obesity of the child, SES, and BMI of the mother.
The prevalence of overweight/obesity in children aged between 0 and 5 years found in this study was low compared to other investigations. In a study from the United States, the prevalence of overweight in children from 1 month to the sixth grade was between 16.6% and 34% 28 ; however, the prevalence of overweight and obesity in the American population is much higher than in Peru's population, which is why differences are understood. Furthermore, in a study based on data from Child Lives Cohort, 36 it was found that the prevalence of both in children aged 6–18 months was 21.6%. On the other hand, in a research with data from the Nutritional Status Information System with the same population of this study, the highest prevalence was of 6.8% in 2014. 48
The prevalence of depressive symptoms in this article is comparable to that of other studies. In a study conducted in New York, the prevalence of moderate-severe depressive symptoms was 7.7%, using the same instrument. 40 In addition, in another study that analyzed depressive symptoms at different times, the prevalence of these was, on average, 8.9%, using the Brief Symptom Inventory. 49 In other studies, there is a higher prevalence of depression in mothers, as in a Mexican study, in which it was 21.4%. 28 However, the tool used is the Center for Epidemiologic Studies Depression Scale (CESD-7).
The association between maternal depressive symptoms and overweight/obesity in their children is reviewed in the literature, but an exact conclusion has not been reached. Although in this study no association was found between these variables, it is important to consider that some factors might interact. For example, the PHQ-9 evaluates the presence of depressive symptoms in the last 15 days but does not indicate previous maternal episodes. Additionally, other variables as the person in charge, other than the mothers, of the children alimentation should be considered. On the other hand, there are studies in which this association has been found.27,28,39,40 However, most of these are performed in different populations. Likewise, there are studies where they find the association at a certain stage, but not at other times.28,49,50 In a systematic review that analyzed articles published between the years 2000–2014, extrapolated data were not found, because—although an association between maternal depressive symptoms and overweight/obesity in children or the risk factors associated with them was found—, populations had very delimited characteristics. 26 On the other hand, there are articles where there is no association between both variables.14,51,52 Despite this disagreement, in general, studies suggest that the mechanism by which these variables might be associated would be that the mother, when presenting depressive symptoms, downplays the importance of caring for her child. This would have consequences in the overall development of the child, including weight. In this way, the mother would not pay attention to a healthy diet for her child and the child may suffer from malnutrition, by either default or excess. In addition, they suggest that mothers with depression, in general, engage in fewer interactions, especially those involving physical activity.27,29,49 Moreover, it is hypothesized that postpartum depression results from weight, hormonal changes, and sleep habit changes, which would cause negative consequences in the relationship with the child. 28
In this study, a statistically significant association was found between the upper quintiles of SES and overweight/obesity. This means that the higher individuals are in the socioeconomic scale, the more likely it is that the child will suffer from these conditions. A systematic review found that, in developing countries, both variables were associated in children and adolescents. 34 In addition, multiple studies done with Peruvian populations find this same association. One of them, in which ENDES data from 1996 to 2011 were used, found that overweight was more prevalent in the urban area, 53 which includes more individuals in the upper quintiles of the SES. Another research that studies the same population, but uses data from the Monitoreo Nacional de Indicadores Nutricionales (MONIN) (Nutritional Status Information System), found a prevalence of 7.2%, 8.4%, and 11.9% in Q3, Q4, and Q5, respectively, compared with 5.2% found in Q2. 54 Similarly, a study with data from the 2009–2010 ENAHO (National Household Survey), found a higher prevalence in those that belonged to the nonpoor sector (10.6%) compared with the sectors of extreme and nonextreme poverty (3% and 6.3%). 4 All these findings suggest that those who have a better SES have greater access to buy food with more caloric content for their children. Moreover, although this article did not evaluate the physical activity of the child, the fact that they have a better economic status might be associated with a more sedentary life, possibly caused by a greater time in front of screens (electronic games, computers, tablets, and others) that can be accessed because of this same economic situation.
Additionally, this article identified an association between maternal BMI and overweight/obesity of the child. Similarly, there are studies that have found an association between these two variables.38,55,56 Despite the fact that these were performed in infants at different ages, in all three studies a strong association was found between maternal BMI and excess weight in their children. There is also a consensus that the weight of the mother or parents influences their children's weight not only with the obesity genes, but also with the behavior and food practices.
Finally, an association between the birth canal and overweight/obesity in the child was also found. According to our results, the child born by C-section is more likely to be overweight/obese than the child born by vaginal delivery. According to a meta-analysis published in 2013, a child born by C-section has a 33% higher risk of suffering from overweight/obesity than a child born by vaginal delivery. All this, although not clear yet, may be due to the lack of exposure to vaginal microbiota at birth. 57
No association was found between breastfeeding and overweight/obesity in our study. However, it should be noted that this variable was not properly explained in the ENDES. For this reason, its exclusivity or length was not specified. Nevertheless, other studies have found that breastfeeding is a protective factor against these conditions. Although overweight and obesity were not defined in the same way in all of them because they were international studies, it was also found that their length is even more important. This is because the children who were breastfed for more than 6 months were at a lower risk of becoming overweight or obese during their lives.58–62 Other studies found that those children who were not breastfed or received supplementary feeding before 6 months were at greater risk of developing malnutrition by excess.60,62 Although most studies mention that the mechanism by which breastfeeding as a protective factor is complex, they agree that some hypotheses are related to the passing of hormones such as ghrelin, leptin, and adiponectin, among others, which would influence the development of overweight or obesity through various mechanisms.60,63–65
The main limitation of this research is that it is an analytical cross-sectional study because temporality and causality cannot be found between positive associations. Another limitation is the lack of variables provided by the 2016 DHS, such as type of the child and mother's food, feeding practices, physical activity, and hours of sleep. Other variables that were used—but whose definition in the DHS did not allow a deeper analysis like that of breastfeeding—were diabetes and high blood pressure as they are self-report variables. Additionally, other limitation is the lack of criterion validity of the used instrument (PHQ-9); however, in the mentioned articles, PHQ-9 has good sensibility and specificity, and both found construct validity. It is also important to mention that this instrument is widely used to detect depressive symptoms in previous studies.
The sample size analyzed is one of its strengths. The type of sampling that the National Institute of Health (INS) carried out when developing the ENDES allowed for a representative sample of the country. By using the command svy, the sample obtained by this type of sampling was correctly analyzed. In this way, it was possible to extrapolate positive associations on the Peruvian population. This would help the Peruvian public health to develop improvements in their health programs. Most of all because although the prevalence of these diseases are relatively low, they are likely to increase over the years and, unlike malnutrition, there are no well-established public health measures in our country to combat those problems. Furthermore, our results highlight the importance of establishing a preventive pattern that involves the whole family, not just an individual.
We recommend carrying out a future study that keeps track of children with their mothers over the years. While it is true that this study found no association between maternal depressive symptoms and the child's overweight/obesity, other researchers have found it. Therefore, it would be ideal if we continue investigating with different methods, especially due the current increase in the prevalence of depression and obesity globally. Moreover, it would be ideal if we carry out further studies that seek to associate socioeconomic status and overweight in children.
Conclusions
In this study, no association was found between maternal depressive symptoms and the child's overweight/obesity in children aged 0–5 years, according to the 2016 DHS. However, it was found that upper quintiles of socioeconomic status, maternal BMI, cesarean birth, and the outcome were associated.
Footnotes
Acknowledgments
Universidad Peruana de Ciencias Aplicadas.
Scientific Society of Universidad Peruana de Ciencias Aplicadas.
Funding Information
The senior author acknowledges the Direction of Research of Universidad Peruana de Ciencias Aplicadas.
Author Disclosure Statement
This investigation was conducted as the thesis for the MD title of AM and NE. No competing financial interest exist.