
Abstract
Background:
Many families with young children practice nutrition, parenting, and lifestyle behaviors that set their children on trajectories for unhealthful weight gain. Potential adverse health effects of excessive body fat can result in the secretion of proinflammatory molecules and increased risk of inflammation and metabolic diseases. A pediatric obesity risk assessment tool named Healthy Kids (HK), demonstrated validity in a longitudinal study with child's measured BMI and 36-hour diet, screen, sleep, and activity logs. Our objective was to provide additional evidence of validity with low-income families with literacy issues using an inflammation index composed of four proinflammatory biomarkers.
Methods:
Parent/child pairs (n = 104) from Head Start and Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) provided HK, blood samples, and measured heights/weights. Select child inflammatory markers were discretized into two groups of HK scores. Data were analyzed with a mixed model adjusted for children's age and BMI.
Results:
A significant HK–time interaction effect was shown for the child inflammation index with two data collection points 1 year apart (pdid = 0.039). This index increased over 12 months in children with less healthful behaviors (p = 0.007), but not in children with more healthful profiles (p = 0.58).
Conclusions:
Children with less healthful HK scores had an elevated inflammation index indicating a low-grade chronic systemic inflammatory state. Taken together with our previously published findings, the HK tool has potential as a rapid and easy-to-administer assessment of the family environment and the child's obesity risk. HK can be useful for federal nutrition programs for evaluation, risk assessment, goal setting, and/or program planning in clinical and community environments.
Introduction
The 2016 prevalence of preschool children who are overweight is 26% and obese is 16%, despite concerted public health efforts. 1 Low-income families are less likely to recognize their children are overweight or believe they should change lifestyle behaviors despite having disproportionately higher rates of overweight and obesity.2,3 Obesity can induce a state of low-grade chronic inflammation and increase the risk of developing metabolic complications, such as insulin resistance, metabolic syndrome, cardiovascular problems, and asthma.4–6
The potential adverse health effects of excessive body fat are determined largely by type and distribution of fat. 4 Excessive abdominal fat, also known as visceral fat, results in the infiltration and activation of innate immune cells within this tissue and the secretion of proinflammatory molecules.7,8 Some of these molecules such as C-reactive protein (CRP),8–11 interleukin-8 (IL-8),12,13 tumor necrosis factor-alpha (TNF-α),7,9,10,14 and retinol-binding protein-4 (RBP4)15,16 are used as biomarkers to predict obesity risk, inflammation, and metabolic diseases although most of this work has been done in adolescents and adults. There are fewer studies with young children.17–19
Parents have direct influence over young children's physical and social environments related to child's weight status.6,20 Yet, many families are practicing nutrition, parenting, and lifestyle behaviors that set young children on trajectories for unhealthful weight gain. 20 Children 2–5 years of age are more susceptible to achieve higher BMI levels than at any other age in response to lifestyle stimuli. 4 In response to high child obesity rates, Congress authorized federal programs to include obesity prevention in federal education programs for families with young children. These programs include: Head Start 21 ; Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) 22 ; Supplemental Nutrition and Assistance Program–Education (SNAP-Ed) 23 ; and Expanded Food and Nutrition Education Program (EFNEP). 24
These four programs have a presence in all or most low-income communities in the U.S. Consequently, they have the potential to impact obesity prevalence among families. 25 Recognizing that this young age may be ideal for intervention, the Institute of Medicine (IOM) and the American Academy of Pediatrics (AAP) recommend the development of assessment tools targeting families' modifiable environmental and behavioral factors associated with the risk of pediatric obesity.20,26
Using the results of extensive literature reviews27,28 and qualitative cognitive interviewing, 29 we created a young child's obesity risk assessment tool called Healthy Kids (HK) replete with visuals that replace and clarify text making it suitable for families with limited literacy. 29 This 19-item tool contains assessments for these family-based behaviors: eating together, fruit availability, accessibility and intake, fruit as a snack, vegetable availability and variety, vegetable as a snack, vegetables at main meal, milk and sugar-sweetened beverage frequency, energy-dense foods and snacks, dairy and meat fat, modeling at mealtime, bedtime, screen time, and child activity (Fig. 1). The 19-item HK tool was further validated using 5 measures of validity and 5 of reliability, including predictive validity in a 2-year longitudinal study with measured BMI and three 36-hour sleep–activity–diet logs. 30

Self-reports of behavior can be an efficient way to identify key modifiable behaviors for individual participants in group education settings. 31 However, with self-report behavioral assessments, rigorous methods of validation should be applied. 31 Consequently in this study, we used objective measurements for validation of the HK tool, that is, measured weights and heights and blood biomarkers.
Objective of Study
Building on the qualitative and quantitative work described above, this current article describes the quantitative research to further establish validity of HK using blood values from samples drawn from young children, 2–5 years old. The objective was to show whether HK scores are related to biomarkers of inflammatory status, that is, selected as a proxy for obesity risk. Accordingly, we hypothesized that a lower HK score, that is, less healthful behaviors, was associated with children having a higher inflammation index compared with children with higher HK scores.
Methods
Participants
Participants (n = 104 parent–child dyads) are a subset of a larger cohort of 176 parent–child dyads from a 2-year longitudinal study designed to validate an obesity risk assessment tool. Details on timeline and data collection are presented elsewhere. 30 Participants were recruited at Head Start (n = 13) and WIC sites (n = 2) in two counties in California. They were ethnically diverse parents or caregivers, ≥18 years, who understood English as a first or second language, and had ≥1 children 2–5 years of age. The protocol was approved by the Institutional Review Board of the University of California, Davis.
Data Collection and Participant Attrition
Parents completed a demographic questionnaire at week 1 of the study. Baseline child height/weight measurements were collected at week 15. Parents completed HK at weeks 21–23, and about a year later at weeks 73–75. In close proximity to the above, we collected blood samples and height/weights from children at weeks 23–25 and 75–77. Parent and child data were collected approximately 1 year apart (377 ± 18 days) to minimize potential confounding seasonal effects on household food intake and physical activity. Child heights and weights were measured using digital scales and portable stadiometer (Seca Road Rod, Hanover, MD). BMI-for-age percentiles were calculated using the Centers for Disease Control's BMI Percentile Calculator for Children. 32 Additional details are reported elsewhere. 33
Sample size at weeks 1–15 was 176 with attrition to 133 at weeks 21–25 and 104 for data collected at weeks 73–77. Tests for selective attrition between the retained and dropped families (n = 76 participants) showed no significant differences on demographic parameters. There were 27 participants for which we did not have a child blood sample either due to parents dropping the study or because a sample could not be drawn from the child. For these reasons, we included 104 of the 133 participants at weeks 21–25 with a complete/matching set of data at both time points. A Logistic Regression analysis with dropout as the outcome confirmed that the study dropouts at weeks 23–25 did not differ significantly for the child inflammation index (p = 0.27), BMI-for-age percentiles (p = 0.84), and age (p = 0.20) from the participants remaining in the study at weeks 75–77.
Inflammatory Biomarkers
To measure the four cytokines, about 10 mL of blood was collected from fasted children through venipuncture by a pediatric certified phlebotomist. Body temperature was taken to rule out potential illnesses as confounders to inflammation markers. Serum and plasma vacutainer tubes were stored on ice for transport to the laboratory at the USDA Western Human Nutrition Research Center on the University of California at Davis campus, where the respective serum and plasma samples were recovered by centrifugation (10 minutes at 1300g at 4°C). Samples were aliquoted and stored at −80°C for later analysis.
Plasma IL-8, TNFα, and RBP-4 were measured by electrochemiluminescent immunoassay using a MULTIPLEX Adipokine Panel or a Singleplex Kit [Meso Scale Discovery (MSD), Rockville, MD]. Internal controls added to each plate assessed plate-to-plate variability. Serum CRP was measured on a COBAS Integra analyzer using an Enzymatic Kit (Roche Lifescience, Indianapolis, IN). For each biomarker, a unique standard curve was generated to harmonize the interassay variability. The four inflammation markers were assayed in duplicates. Duplicates with a coefficient of variability >25% were removed from the dataset.
Inflammation Index
From a biological standpoint, it is rarely possible to rely on a single biomarker to provide a valid assessment of status. 34 The use of a cumulative index delivers a comprehensive portrait of the inflammatory status of the child and provides greater accuracy than using any given individual biomarker. Building on that information, we prepared an inflammation index that was the sum of four cytokines, IL-8, RBP-4, CRP, and TNFα, measured from children's blood samples collected at weeks 23–25 and 75–77. The main characteristics of these biomarkers and literature supporting their selection are summarized (Table 1).
Characteristics and Evidence for the Selection of the Inflammatory Markers Measured in Child Participants
Numbers refer to publications cited in the reference list.
AT, adipose tissue; CRP, C-reactive protein; IL-8, interleukin 8; RBP-4, retinol-binding protein 4; TNFα, tumor necrosis factor alpha.
At each time point, the raw values for each cytokine were ordered from low to high, converted to ranks that were then multiplied by 100 and divided by the number of children with a cytokine measurement to produce percentile ranks. For each child, the percentile ranks were summed for each of the four cytokines. The number of children by cytokine varied from 94 to 97. For a given child, the inflammation index represented the sum of the ranks of his/her cytokine values with a potential index score of 4–400. Ranking the four cytokines enabled us to combine the 4 percentile scores independent of their unit of measurement and number of children. Additionally, we expected that the decreased variability of the inflammation index compared with that of the individual cytokines would increase the likelihood of a stronger correlation between variables, similar to the work of Freedman et al. 35
Healthy Kids
Each item was assigned 1–5 points with the highest score indicative of a healthier behavior. Answers to the 19 items were summed for a possible score range of 19–95 points. At each time point, the total scores were discretized into two groups, low HK (19, 67.5) and high HK (67.5, 95), to adjust for skewness of the data.
Statistics
Statistical analyses were performed using SAS (SAS, version 9.3; SAS Institute, Cary, NC). Descriptive statistics were presented as mean with standard deviations for continuous variables, or as frequencies and percent for categorical variables. Preliminary analyses between the inflammation index and HK scores or BMI-for-age percentiles showed that the relationships between these variables were nonlinear. Consequently, the child BMI-for-age percentiles were stratified in three groups [(0, 5), (5, 85) and (85, 100)] and data were analyzed using these BMI categories.
Differences in child inflammation index over time for the two collection periods, 1 year apart, and across the two HK groups, were analyzed by analysis of variance using a linear mixed model with current child age and BMI-for-age percentiles included as covariates. Because there was a significant time–HK group interaction effect, differences between groups were determined by post hoc contrast analysis. Due to skewness, medians and boxplots of the inflammation index for higher and lower HK scores are presented to confirm the direction of the findings. A Kruskal–Wallis test was used to assess the relationship between a child's inflammation index and his/her BMI-for-age percentile at each time point.
Because these data were generated from a cohort extracted from a larger longitudinal study, the power calculation was done a posteriori on this subset of parent–child dyads. Using analysis of variance (ANOVA), with 25 and 68 children in the two HK groups, we had 80% power to detect a 40-point difference in the inflammation index between the two HK groups.
Results
Study Participants
The demographic characteristics of the 104 participants that provided data at both time points (i.e., weeks 21–25 and weeks 73–77) are shown in Table 2. Most parents were young women reporting a low income and participating in federal programs. Children's CRP, IL-8, RBP-4, and TNFα levels are presented in Table 3 for 93–96 of 104 children. The missing data are children for which we could not include all four markers due to insufficient volume of blood collected, or poor reproducibility of the duplicates.
Descriptive Statistics of Study Participants
Categorical data are number of participants (% of sample).
Continuous data are mean ± standard deviations.
Baseline measurements at week 15.
SNAP, Supplemental Nutrition Assistance Program; TANF, Temporary Assistance for Needy Families; WIC, Supplemental Nutrition Assistance for Women, Infants, and Children.
Child Inflammatory Markers for Two Data Collection Points 1 Year Apart with Published Reference Ranges
Published data for large cohorts of children.
SD, standard deviation.
BMI and Inflammation
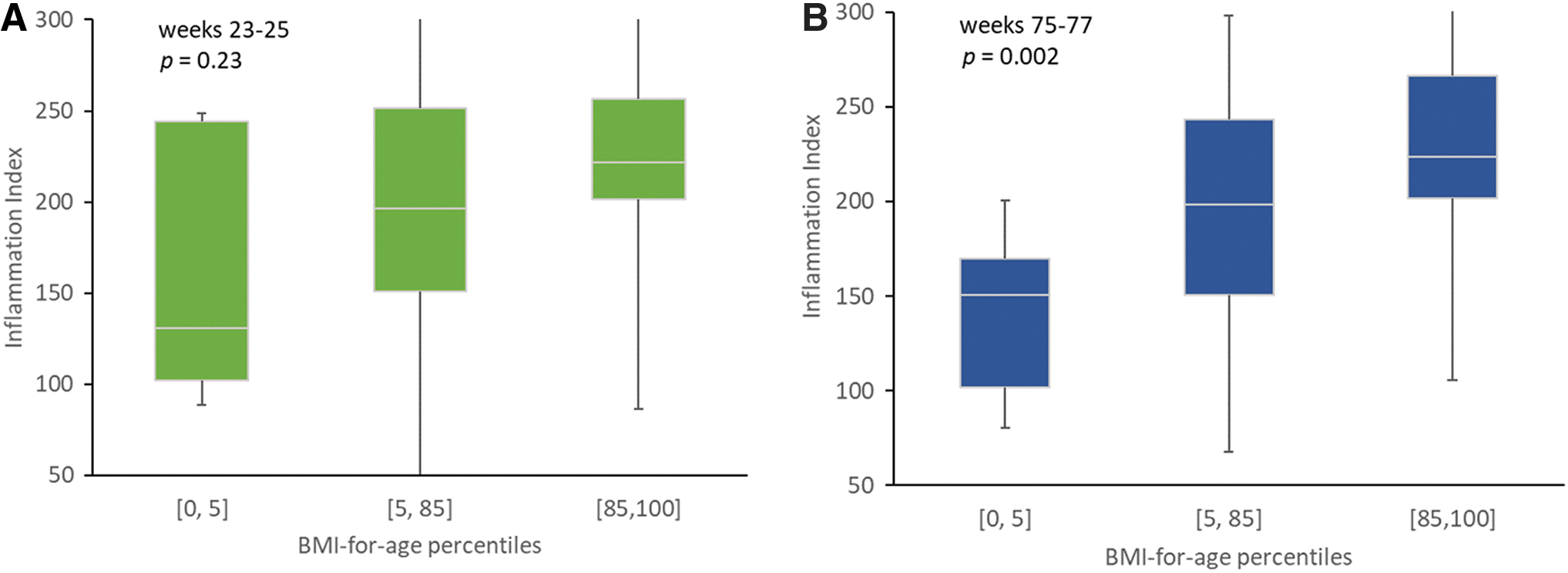
About 70% of the children were normal weight when assessed at week 15. At the study endpoint, that is, week 77, overweight children (BMI-for-age percentiles >85) showed high levels of chronic low-grade systemic inflammation indicated by a higher inflammation index (p = 0.002) compared with children with weights within the normal BMI range (Fig. 2B). A similar relationship was observed at the earlier time point, that is, week 25, but the data were not statistically significant (Fig. 2A).
HK and Inflammation
The relationship between the children's level of inflammation as indicated by the inflammatory index and the HK scores over time was analyzed using a mixed model adjusted for the child's current age and BMI-for-age percentiles (p = 0.0035; Fig. 3). There was a significant interaction effect of time and HK scores (pdid = 0.039). At the first blood draw, the child inflammation index was similar for low and high HK groups (p = 0.774; Table 4). However, 1 year later, the child inflammation index from the low and high scoring groups were substantially different (p = 0.018). The low scoring group increased significantly (p = 0.007) over time while the inflammation index in children in the high scoring group remained largely unchanged at its lower level (p = 0.579; Table 4).

Child Inflammatory Index for Two Data Collection Points 1 Year Apart Stratified by Healthy Kids Scores
Data are means (SD) and medians (IQR). Model was a linear mixed model (pnull = 0.0035) with HK, time, HK × time interaction (pdid = 0.039) with current child age and BMI percentiles for age included as covariates.
Results on post hoc contrast analysis, p-value indicates significant changes in inflammation index over time within an HK group.
Results on post hoc contrast analysis, p-value indicates significant differences in inflammation index between HK group within a given time.
HK, Healthy Kids; IQR, interquartile range.
Individual Biomarkers vs. Index
Because the raw cytokine data did not meet the conditions for the linear mixed model, we used the ranked percentiles to test for the effects of HK and time as described above for the inflammation index analyses. Overall, the profiles of the individual inflammation markers over time by HK scores were similar to that of the inflammation index and the overall model was significant for IL8 and RBP4 as outcomes. All four cytokines increased over time in children in the low-scoring HK group but showed limited changes (TNF, CRP, IL8), or decreased (RBP4) over time in children in the high-scoring HK. In contrast, the difference in outcomes for individual cytokines between HK groups was not significant compared with the inflammation index, thus providing support for use of the index.
Discussion
The current results show that children with higher HK scores have a healthier metabolic profile as shown by their lower inflammation index. Conversely, children with lower HK scores show compromised inflammatory status indicated by the increased inflammation index after 1 year. This time–HK score interaction suggests that family lifestyle and child behaviors can have substantial health effects. Specifically, our interpretation of these data is that unhealthy lifestyle choices over the 1-year duration of the study are associated with an increase in biomarkers of low-grade chronic systemic inflammation most likely due to visceral fat deposition and indicative of obesity and metabolic disease risk.
This study is the first to the authors' knowledge to validate a self-assessment tool for obesity risk with a longitudinal design targeting limited-literacy families with preschool-age participants of Federally funded programs and covering all lifestyle behaviors identified in the literature.27,28 Importantly, the HK assessment tool can serve as a proxy to identify 2–5 year-old children at greater risk of having an adverse inflammation index score, a precursor to chronic disease.4,5,8 In addition, our data show that this condition may be more prevalent than expected. This observation underscores the importance of identification of families with obesogenic lifestyles for early targeted intervention before these behaviors become immune to change in the child.
Inflammation Markers in Children
The values from our study compare reasonably to those reference values published in the literature (Table 3).10,16,36 In addition, our clinical biomarker results are consistent with studies reporting higher levels of inflammation in obese children with ages ranging from 3 to 14 years (Table 1; Fig. 2).9–19 Because so little biomarker research has been undertaken with young children, it was not clear to us at what age biomarkers of inflammation could be used to validate an obesity prevention risk assessment tool. The inflammation index tracked with BMI in our study (Fig. 2), but the relationship only became significant after the children were 1 year older. Coincidentally, this is also the time when HK was able to detect children with higher inflammation index (Fig. 3). These 2–5-year-old children showed evidence of low-grade chronic inflammation, and this is an indication that the selected biomarkers were sensitive to obesogenic behaviors and visceral body fat deposition and thus useful for validation of HK.
In adults and teenagers, circulating levels of inflammation molecules largely result from visceral fat accumulation and have been used as proxy for obesity-mediated metabolic complications. 37 Although limited information was available with respect to young children, obesity, and inflammation, we anticipated that overweight/obese children would exhibit a higher inflammation index than children with low BMI. As expected, a positive linear relationship between these two variables was observed at baseline (weeks 25) and at weeks 77, and reached statistical significance at the later time point (Fig. 2).
The reason for the lack of significance at baseline is unclear. Our sample size was constrained by the number of participants with a blood sample sufficient in quantity for each type of analysis and this small number of participants may have limited the power to detect statistical significance. Our power calculation was based on the ability to detect the difference in inflammation index between HK scores and not BMI. We examined the possibility that a greater proportion of very young children (<3 years old) at baseline could influence the association between inflammation and BMI. This did not appear to be the case for two reasons. First, in our study, only 12 of 95 children were between the ages of 27–36 months at baseline, and the average age was similar among all three BMI-for-age percentile categories. Published data show that some inflammation markers are age dependent38,39 while others are not36,40 or only under certain circumstances such as puberty 40 or infancy. 36
Second, as shown by the descriptive statistics provided (Table 3), the distribution of each of the four inflammation markers measured in the children spanned a wide range. This is particularly true in children with low BMI-for-age percentiles (<5) at weeks 23–25 with an inflammation index ranging from 89 to 248 units, compared with a range of 78 to 198 units at weeks 75–77 (Fig. 2). Two of these children had a high inflammation index at baseline but no longer at the end of study, most likely driven by an underlying metabolic condition unrelated to visceral fat. For all other children, the inflammation index and BMI were consistent over time. These atypical data for two children contributed to the high variability in the inflammation index in this group and may explain the lack of statistical significance at baseline.
Body fat can be a source of variability for cytokine levels in children. Our data show that as they grew older and gained weight, some children became overweight/obese. Of the children in our cohort, 33% were overweight/obese at weeks 75–77 compared with 29.7% at baseline (Table 2). Others have reported elevated levels of CRP,17,19,36 TNFα, 18 and RBP418,40 in overweight/obese children 2–8 years of age. We propose that the redistribution of children in the overweight/obese category reinforced the association between the inflammatory index and the children's BMI making it statistically significant at the later time point.
Comparison to Other Validation Studies
No validation studies supporting obesity prevention tools using markers of inflammation were found for low-income, families with young children, based on our previous reviews.27,28 However, there were three tools reported in the literature subsequent to the aforementioned literature reviews. The 181-item Healthy Home Survey for families with children 3–11 years was validated with in-home observations. 41 The 21-item family nutrition and physical activity screening tool for families with children 6–12 years designed for a medical clinic setting was extensively researched, including validation studies with measured BMI, body fat, lipids, and a clinical assessment of Acanthosis nigricans.42,43 Third, a 15-item evaluation tool developed for families with children 3–11 years participating in EFNEP was validated by comparing it with other self-reported behavioral assessments for diet, lifestyle, and parenting. 44
Despite the harm caused by pediatric obesity, with its effect on long-term health and its impact on medical costs, 6 rigorously validated tools for participants of federal nutrition programs are few and even fewer for limited literacy participants. 31 Consequently, HK is available for practitioners of these programs while other researchers could employ these methods in future validation research. Thus, HK is the only pediatric obesity risk assessment tool for the preschool child validated with blood biomarkers of obesity identified for the federal programs mentioned earlier.
Comparison to Inflammation Intervention Studies
We could locate no studies reporting on interventions to reduce inflammation in 2–6-year-old children. Reports of improved inflammation profile in obese older children and adolescents following lifestyle intervention protocols resulting in weight loss have been published.10,11,14 Our data show that young children exposed to a less healthy dietary and lifestyle environment identified by a lower HK score, exhibited low-grade systemic inflammation 1 year after baseline. The current results are consistent with and substantiate our previous findings that HK is a valid obesity risk assessment tool using BMI as the outcome measure. 30
One interpretation of these new data is that when using markers of inflammation for validation, the HK tool can identify earlier those children set on a trajectory for unhealthy weight gain, that is, before they reach a high BMI. With this interpretation, HK would be a valuable tool to assist interventionists with identification of children most at risk. For federally funded nutrition education programs, limited resources could now be targeted to those children most at risk before additional unhealthful weight gain. Although healthy children are expected to have low or no inflammation if they maintain a normal weight, our data suggest that abdominal obesity may develop insidiously in children faced with a less healthy family environment and induce systemic low-grade inflammation even in children with BMI within normal ranges. We reported a positive association between inflammation and BMI in these children and anticipate that this association would become stronger should the children's weight gain trajectory continue unchecked.
Using HK
HK, a simple paper/pencil self-assessment, is also the first to be evaluated using multiple data types, including blood values and measured heights and weights for the preschool child. The HK behavioral checklist format with color photographs circumvents the limitations of traditional data collection methods, such as the relatively complex and time-consuming 24-hour diet recall and blood samples. These measures are difficult and expensive for federal education and nutrition programs to routinely collect and analyze for program evaluation. 31 This visual checklist format is the preferred option for audiences with limited literacy. 45 HK takes less than 10 minutes to complete, maximizing time for nutrition education lessons and results could assist parents with goal setting during the nutrition education experience. 46
This tool could serve other functions as well. First, it could assist with determining those young children most at risk of low-grade inflammation and excess weight gain. Nutrition professionals could use the information from HK and accompanying website 47 to target nutrition education and/or counseling to those families with identified at-risk children, particularly those parents/children enrolled in SNAP-Ed, EFNEP, WIC, or Head Start. HK could serve as evaluation to assess program or intervention impact considering that this tool meets federal requirements for use of valid assessment tools. This tool is important for early screening as the primary prevention literature indicates that intervention efforts are more successful if begun before the child is classified as overweight or obese. 20 Clinically, medical providers could benefit from a risk assessment tool to supplement a physical exam to gain additional information about the family-based behaviors during well visits.48,49
Limitations and Strengths
The primary strength of this study is use of inflammatory markers of preschool children at two time points 1 year apart to estimate validity of HK (Fig. 3). Blood samples are not subject to the self-report bias of the parent. 31 The external validity of these findings to other limited-resource audiences is unknown. These results may be applicable to similar groups of program participants. Parents, and thus children, volunteered to participate in this study. Consequently, selection bias should be considered as a threat to external validity. 50 Social desirability bias influencing parent responses must be noted as a threat to internal validity, reducing differences between high and low HK scores. In addition, the Hawthorne effect may have served as a motivator for healthier food offerings by the parent during the 12 months of the study, thus may have impacted the blood values. 50
Next Steps
HK is a work in progress with face, 29 content,27,28 convergent, 30 predictive, 30 and now criterion validity estimated. Currently underway, is a new HK research study with Spanish-speaking parents and their young children in California.
Conclusions
To our knowledge, this is the first and only longitudinal study using inflammation markers to validate a pediatric obesity assessment tool. This study was conducted with low-income families, many of whom have literacy issues. This tool is appropriate for those adults reading at grade 2 and higher. HK has potential as a rapid and easy-to-administer parent assessment of the young child's risk for becoming overweight or obese. Further validation is provided by results from this current study: young children with lower HK scores have more chronic low-grade systemic inflammation, indicated by an elevated inflammation index. It appears that these preschool children are not immune to chronic systemic inflammation when engaging in sustained obesogenic behaviors resulting in positive energy balance and that a low HK score can detect these children.
Footnotes
Author Contributions
M.S.T. was the principal investigator responsible for the grant, conceptualized the study, interpreted results, and wrote all drafts of the article. M.K.S. was co-PI on the grant, conceptualized the study, supervised data entry and management, and reviewed drafts. D.M.S. was a collaborator on the grant, conceptualized the study, and provided substantial intellectual input in the selection of the biomarkers. C.D. supervised the statistical analyses, and interpreted results. L.L. conducted all statistical analysis, interpreted the biomarker results, and cowrote the article drafts. L.W. supervised the biomarker analyses. All authors reviewed and approved the final version of the article. L.O. was a co-PI on grant, conceptualized the study, and reviewed drafts. All authors approved the final article.
Ethics Approval and Consent to Participate
This study was approved by and conducted in accordance with the ethical standards of the Institutional Review Board at University of California, Davis. An oral and written description of the study was given to parents who provided written consent for themselves and their participating child.
Acknowledgments
The authors thank Ellen Bonnel, PhD, for establishing and executing the protocol for blood collection and processing; professor Kathryn Sylva for the HK design; Brenda Campos and Meghan Marshall of SETA Head Start in Sacramento, CA, for their ongoing support making this study possible; Christine Davidson, Larissa Leavens and Danielle Rehnstrom for data collection and processing.
Funding Information
This material is based upon work that is supported by the National Institute of Food and Agriculture, U.S. Department of Agriculture, under award nos. 2010-85215-20658 and 2015-68001-23280.
Author Disclosure Statement
No competing financial interests exist.