
Abstract
Background:
Obesity among children and adolescents is a worldwide public health concern. Type 1 diabetes (T1D) and type 2 diabetes (T2D) incidence are increasing, with heredity and socioeconomic status as possible risk factors. How these factors affect the risk of childhood obesity remains unclear. The aim of this study was to investigate the association between obesity and parental diabetes among 12-year-olds in Sweden, and how it relates to parental education level.
Methods:
We used data collected within the Exploring the Iceberg of Celiacs in Sweden (ETICS) study, a cross-sectional multicenter national screening study for celiac disease in 12-year-old children. Relative risk (RR) and confidence interval (CI) were calculated for the association between parental diabetes and obesity, also stratifying for gender and highest parental education.
Results:
Among 11,050 children, for both children with parental T1D and T2D, 31% of the children were overweight or obese, compared with 21% among other children. Comparing those with parental T1D with those without parental T1D within gender, boys had a statistically significant higher risk [RR 1.6 (95% CI 1.3–2.0)], and girls had a nonsignificant increased risk [RR 1.3 (95% CI 0.95–1.8)], of being overweight. For children with parental T2D, both boys and girls had a statistically significant increased risk of 1.5. Parental education showed no sign of influencing the RRs.
Conclusions:
Parental diabetes is associated with an increased risk of overweight among children, independent of parental education. Concomitant parental diabetes and overweight should be particularly alarming criteria when prioritizing preventive interventions at an early age.
Introduction
The prevalence of overweight or obesity in both children and adolescents remains high, and it is still increasing in large parts of the world, making it a worldwide public health concern and challenge.1–3 Being overweight is a strong precursor for the increase in the prevalence of Type 2 Diabetes (T2D) seen in this age group for the past several years. 4 Parental diabetes has been shown to be an independent risk factor for T2D.5,6
A study in the United States reported the prevalence of T2D among adolescents (10–19 years) to be 0.046% in 2009, and that the prevalence among adolescents was 35% higher than in 2001. 7 An increase in incidence of Type 1 Diabetes (T1D) has also been observed among children elsewhere in the world.7–9 Sweden has had a doubling of incidence rates during the years 1978–2007. 10 Several reports claim that the increasing incidence of T1D may be correlated with the increased incidence of overweight among children.11–14 One of these reports concluded that children with a certain genotype and having overweight also had an increased risk for T1D. 11
Heredity (genetics) and environmental factors (health behaviors of the family, including diet and physical activity) both play a role in childhood obesity.15–18 The latter have also been shown to be affected by parental socioeconomic status, where those with a lower socioeconomic status, in Europe, were shown to have a greater risk of overweight.19–21
One recent study showed that children of overweight parents are more than twice as likely to be overweight compared with those with parents of normal weight, although this may vary with the economic level of the country of residence. 22 Although parents with diabetes, irrespective of T1D or T2D, have been counseled on healthy lifestyle that could affect the health behaviors of the whole family, the genetic risk remains. There are few studies on parental diabetes as a risk factor for childhood overweight.23–25 None of these studies have been performed in combination with socioeconomic status or parental education level as a separate factor, which could help to differentiate the impact of genetics vs. environmental risk factors.
The aim of this study was to investigate the association between parental diabetes and obesity among 12-year-olds in Sweden, and how it relates to parental education level.
Methods
Study Design
All of the children in this study participated in the Exploring the Iceberg of Celiacs in Sweden (ETICS) study, a two-phase cross-sectional multicenter screening study for celiac disease in 12-year-old children. The screenings were school based, and there were two field phases conducted, the first in the school year 2005–2006 and the second in the school year 2009–2010, hence including two birth cohorts of 12-year-olds; those born in 1993 and in 1997. The screening phases used the same study design. The ETICS study was approved by the Regional Ethical Review Board of Umeå University, Umeå, Sweden (Dnr 04-156). In this study, we used information collected at the time of the screening about the child's height and weight, and responses by the parent of the participating child to a questionnaire, from which we used information about parental diabetes and highest parental education level.
Study Participants
Children in the sixth grade from five different study sites (Lund, Umeå, Norrtälje, Norrköping, and Växjö) were invited to participate in the ETICS study.
Informed consent was obtained from at least one legal guardian before a child was enrolled in the study. In the first field phase, 7567 children participated, and the second field phase enrolled 5712 children, covering 10% of the 12-year-olds in Sweden. The proportion of girls participating was similar in both cohorts (48% girls in the 1993 cohort, and 49% girls in the 1997 cohort). Further descriptions of children participating in ETICS, along with details of the celiac disease screening strategy, are available in two previous publications.26,27
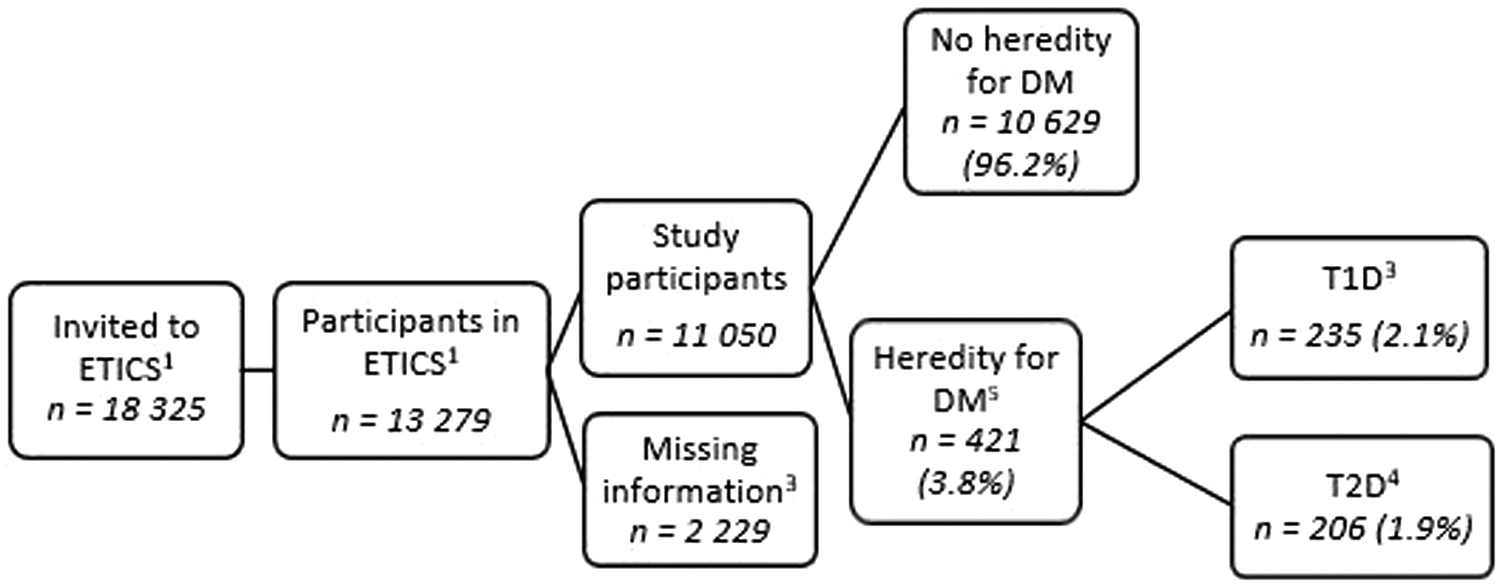
Information about weight and height, and parental diabetes, was required for this study (Fig. 1), resulting in the exclusion of 2229 (16.8%) children in our analyses, of them 480 lacked weight data, 487 lacked height data, and 2038 did not respond to the questionnaire.
Anthropometric Assessment
Newly calibrated scales were used when weighing children although they were wearing light clothes. A wall-mounted stadiometer was used when measuring their height, in a straight line with their head in an appropriate position.
BMI was calculated as weight/squared height (kg/m2). Overweight was defined according to Cole's international age and gender-adjusted cutoff values for the age of 12 (iso-BMI cutoffs used for overweight; 21.22 for boys and 21.68 for girls). 28 We did not differentiate obesity from overweight as there were only a few obese children who had parental diabetes.
As previously reported by the ETICS study, 23% of the participating children in the second cohort (born 1997) were overweight or obese. 29 Also from the first cohort (born 1993) the prevalence of overweight has been reported from the ETICS study by van der Pals et al., 30 and it was 22% (combining data reported in their study) of participating children who were overweight.
Questionnaires
A parent or other legal guardian of the child was asked to complete the questionnaire and return with prepaid postage. Three questions from the questionnaire were used in this study. Two of these concerned diabetes diagnosis among the biological parents, and whether they have an insulin- or noninsulin-dependent diabetes diagnosis. The questionnaire used Swedish common language, and the term insulin-dependent diabetes will be referred to as T1D, and noninsulin-dependent diabetes as T2D in this study. Parental diabetes was defined as having a mother and/or father with either T1D or T2D.
The third question concerned the highest education level of the adult/adults that the child mainly lived with. The choice options for completed years of school were <9 years of schooling, completed 9 years of schooling, completed 12 years of schooling, completing one or more years of tertiary education, or receiving an academic degree. In our analyses, at most 9 years completed years of schooling was defined as low-level education, completed 12 years of schooling was defined as middle-level education, and >12 years of schooling was defined as high-level education.
Statistical Analysis
The relative risk (RR) of being overweight or obese among children with parental diabetes, compared with the children with no parental diabetes, was reported with 95% confidence interval (CI), and, thus, the statistical significance was defined at a 5% level. Analyses were also conducted stratified for the gender of the child, field phase, maternal and paternal diabetes, and highest degree of parental education. SPSS 11.0.5 (SPSS, Inc., TX) software was used for all the statistical calculations.
Results
In total 3.8% of the parents reported having diabetes, approximately half for each of the two types of diabetes (Fig. 1). For 20 of the children (0.18% of the study population), it was stated that the parents had both T1D and T2D.
The prevalence of overweight or obesity was higher among children with parental diabetes for diabetes; 31% of those with parental T1D, and 31% of those with parental T2D (Table 1), compared with 21% of children with no parental diabetes.
Baseline Characteristics of the Study Population
T1D (response heredity for insulin-dependent DM).
T2D (response noninsulin-dependent DM).
No further than finishing preschool.
No further than finishing high school or 1 year of higher education.
University graduate.
T1D, type 1 diabetes; T2D, type 2 diabetes; DM, diabetes mellitus.
The risk of being overweight or obese was statistically significantly increased for those with parental T1D diabetes, RR 1.50 (95% CI 1.24–1.82), and T2D, RR 1.48 (95% CI 1.20–1.82), compared with those with no parental diabetes (Table 2).
The Association between Overweight/Obesity and Diabetes Mellitus among 12-Year-Old Children, Stratified for Gender, Study Year, and Highest Parental Education
Relative risks in bold are statistically significant.
T1D (parents stating that they have insulin-dependent DM).
T2D (parents stating that they have noninsulin-dependent DM).
There were 260 children who lacked information regarding parental education.
No further than finishing preschool.
No further than finishing high school or 1 year of higher education.
University graduate.
RR, relative risk for overweight/obesity, comparing those with heredity for DM (exposure group) with those with no heredity for DM (reference group); CI, confidence interval.
The results were similar when analyzing maternal and paternal diabetes diagnoses as separate factors for parental diabetes, both for T2D and T1D (data not shown).
Of the boys, 23% were overweight or obese, compared with 19% of the girls (Table 1). Boys with parental T1D had a statistically significant higher risk of being overweight or obese than boys without parental diabetes; RR 1.61 (95% CI 1.28–2.04), whereas there was a nonsignificant increased risk for girls with parental T1D; RR 1.32 (95% CI 0.95–1.84) (Table 2). The risk of being overweight or obese among children parental T2D was statistically significant and similar for both girls; RR 1.51 (1.12–2.04) and boys; RR 1.48 (1.11–1.95) (Table 2).
The prevalence of overweight was 2% higher for the children born in 1997 compared with the ones born in 1993. The children born in 1997 also had a higher risk of being overweight if they had parental T2D when compared with the corresponding group of children born in 1993 (Table 2).
The highest prevalence of overweight was seen among children with parents with low education (31% of 519 children in the low education strata), and the lowest prevalence was seen among the children with at least one highly educated parent (17% of 5496 children) (Table 1). However, when having parental T1D, the latter group of children had an RR of 1.70 (95% CI 1.23–2.35) for being overweight, a higher risk than the corresponding numbers for the children with lower parental education (Table 2). For children of parents with low education with parental T1D or T2D, there was no statistically significant difference in risk when compared with children of parents with low education with no parental diabetes.
Discussion
This study of 11,050 children, all of whom were about 12 years old, showed that there was a higher risk of being overweight for children with parental diabetes compared with children without parental diabetes, irrespective of the type of diabetes. This increased risk showed the same pattern regardless of parental education level. We also found that boys with parental T1D have a higher risk of being overweight than girls, but could not find any gender difference in the group with parental T2D.
Our finding of a positive association between parental diabetes and overweight or obese among children is compatible with the findings of previous studies conducted on children and young adults in other countries.23–25 In these studies, the corresponding results were based on participating parents with T2D or any type of diabetes. 25
One probable cause for the observed results regarding the increased risk of overweight for the children with parental T2D could be that parents with T2D, presumably, are overweight; hence, as shown in previous studies, increasing the risk, both environmentally and genetically, 31 for the child to be overweight, either in childhood 32 or in adulthood. 3 These children will then have a greater risk of receiving a T2D diagnosis, since two important risk factors for receiving a T2D diagnosis at a young age are overweight and a family history of the disease.33–36 However, a previous study of the same population showed that, at age 12, these children had not yet developed T2D. 29
Contrary to our expectations, children with parental T1D also had an increased risk of overweight, and the estimated risk was even slightly higher than for T2D. Several reports claim that increasing T1D incidence may be correlated with the increased overweight incidence among children.11–14 Overweight is also hypothesized to accelerate the process of developing T1D among children who are genetically predisposed to the disease. 37 Our results might support a link behind this theory, and may also raise the question of whether children with parental T1D have an increased risk of overweight due to inherited susceptibility to insulin resistance, and may, therefore, have an increased risk of developing both overweight and diabetes.
In our study, 12-year-old boys with parental T1D had a higher risk of overweight compared with girls. It is interesting that boys at this age are more often overweight, although there is also an increasing gender difference in T1D incidence that favors boys in this age group. It is speculated that this may be due to increased counter-regulating hormones during puberty and growth that favor an insulin resistance in genetically susceptible children, leading to an increased risk of exhausted beta cells and T1D. 37 The insulin resistance may be even greater if this group of boys is also more prone to be overweight.
T1D incidence has been shown to be almost twice as common among boys compared with girls, after age 15. 38 This leads us to consider another theory; perhaps there is a true gender difference with a genetic origin for an increased susceptibility to insulin resistance that promotes increased weight.
Contrary to our expectations, parental education level did not influence the prevalence of overweight in the groups with parental diabetes, which might support the influence of genetic factors in the development of overweight in families with a high level of education. However, education is only one measure of socioeconomic status, and we cannot exclude that financial measures would impact the risk.
Overweight among children with parental T2D did not differ between different levels of parental education, as we expected. Regarding T1D, it was somewhat surprising that the children from the “highly educated” strata had a higher RR than the ones from the “middle educated” strata. In this case, we believe that the results might be influenced by other social factors than education itself, therefore confounding the results for those in the middle (and low) educated strata, where certain factors have a greater impact than in the highly educated strata.
One of the strengths of this study was that it is population based, with a substantial number of children of the same age, gathered from different cities and environments around the country. The fact that the population was approached for a celiac study, and not diabetes, might be an advantage for our study, as it may minimize the risk of selection bias.
A possible weakness of the study could be that children with overweight or obesity did not want to be weighed, as a result of feeling embarrassed, consequently excluding themselves from the study. However, the prevalence of overweight in our study resembles that of other published studies, 2 and the proportion of children whose weight was not measured was low; therefore, we believe this only marginally, at most, affected our results. Not having information regarding the parental weight status, parents' age and parents' age at diabetes diagnosis is, nonetheless, a definite weakness as it would have made it possible to assess the potential role of having a parent or both parents affected by either type of diabetes on the risk of overweight/obesity in the offspring. The effect of parents' overweight/obesity and their age would then have been controlled in the statistical analysis. It is likely that, adjusting for parents' BMI or obesity, the children with one or both parents with diabetes should not have more risk of overweight or obesity than those with nondiabetic parents.
Another limitation to this study was that the parental diabetes diagnosis was based on questionnaire data. Consequently, this could be subject to inaccurate reporting, and we cannot further separate different subgroups of diabetes. In an attempt to minimize misinformation from a parent's misreporting the other parent's diabetes diagnosis, the answer choices in the questionnaire were set to either insulin-dependent or noninsulin-dependent diabetes. One is likely to be mistaken about the wording of the diagnosis, but one is less likely to forget witnessing an insulin injection. Therefore, a T1D patient may be mistakenly classified as a T2D patient based on the information from the questionnaire, as T2D can also be treated with insulin at a later stage of the disease. In our study, we did not collect information regarding gestational diabetes mellitus (GDM). It is known that women who have had GDM are at risk of developing T2D after delivery, and their offspring is at risk of developing overweight/obesity and T2D later. 39 However, we do not believe that these limitations significantly affected our results.
One further limitation was that, despite including >11,000 children, in some stratified groups (e.g., female gender and low parental education), too few participants were included for conclusive results to be drawn.
The prevalence of overweight or obesity is high. Numerous children and adolescents will grow up to be overweight or obese, with all the attendant-associated health risks, 40 one of which is an increased risk of T2D in adulthood. 41 Understanding factors influencing the risk of developing childhood overweight or obesity, such as parental diabetes (possibly an influence) is important. We believe it is crucial to identify effective strategies and interventions at an early age in high-risk individuals to reduce the risks of developing diabetes. It is more cost-effective for society, and the individual, to help the identified at-risk children at an early stage through interventions.
In conclusion, children with parental diabetes seem to have a higher risk of becoming overweight before puberty, which in turn may increase their risk of developing diabetes in adolescence and adulthood. The risk patterns were similar irrespective of parental education level, which may underline the influence of genetics on BMI in children. Concomitant parental diabetes and overweight or obesity should be particularly alarming criteria in prioritizing preventive interventions for children at an early age.
Footnotes
Acknowledgments
We want to thank all participating children and their families along with the people who worked on the initial ETICS study, including research nurses and collaborators within the school health services.
Funding Information
This study was funded by the European Union-supported project FP6-2005-FOOD-4B-36383-PREVENTCD, the Swedish Research Council (grants 521-2004-7093 and 521-2007-2953), the Swedish Research Council for Environment, Agricultural Sciences and Spatial Planning (grants 222-2004-1918 and 222-2007-1394), and the Swedish Council for Health, Working Life and Social Research (grant 2005-0802).
Author Disclosure Statement
No competing financial interests exist.