
Abstract
Objective:
To explore whether the association between bottle-feeding during the first year and childhood obesity at age 6 years is mediated by change in weight-for-age z-score (ΔWAZ) during infancy.
Methods:
Participants were 1062 mother–child pairs who participated in the Infant Feeding Practices Study II and Year 6 Follow-Up. Mothers completed 1 prenatal questionnaire, 10 postpartum questionnaires during the first year, and 1 follow-up questionnaire at 6 years. Child weights were reported by mothers and used to determine ΔWAZ from birth to later infancy. Causal mediation analysis was used to determine the average direct effect of bottle-feeding on obesity at age 6 years and the average causal mediation effect of bottle-feeding through ΔWAZ.
Results:
Infants who experienced rapid increases in bottle-feeding frequency during the first 6 months had significantly greater ΔWAZ compared with infants who had consistently low bottle-feeding frequency until 12 months of age [β = 0.45, 95% confidence interval (CI) 0.11–0.80]. Significant predictors of obesity at age 6 years were larger birth weight [adjusted odds ratio (AOR) = 4.27, 95% CI 2.42–7.64] and larger ΔWAZ (AOR = 1.59, 95% CI 1.29–1.98). An indirect effect of bottle-feeding, mediated via ΔWAZ, accounted for 59% of the total effect of bottle-feeding on obesity at age 6 years.
Conclusions:
Rapid increases in bottle use during the first 6 months postpartum predicted greater risk for obesity at age 6 years via an indirect mediation effect of larger ΔWAZ from birth to later infancy.
Introduction
High prevalence of childhood obesity remains a major public health concern. 1 Most recent data from the 2015 to 2016 National Health and Nutrition Examination Survey (NHANES) illustrate that 18.5% of children aged 2–19 years have obesity compared with only 10% in the 1988–1994 survey. 2 Obesity during childhood is one of the strongest risk factors for obesity during adulthood, 3 as well as for early onset of a number of medical and psychosocial comorbidities, such as type 2 diabetes and markers of cardiovascular disease. 4 Identification of early risk factors for childhood obesity is critical for identifying potential targets for primary and secondary prevention efforts. 5
When considering postnatal targets for prevention efforts, a large body of research demonstrates that rate of weight gain during infancy is a significant predictor of risk for later childhood obesity.6,7 In a recent meta-analysis, Zheng et al. found that infants who exhibited rapid weight gain during infancy had 3.66 greater risk for obesity during childhood than infants with slower rates of weight gain, with rapid weight gain between birth and 1 year more strongly associated with later obesity risk than rapid weight gain between birth and 2 years. 7
Parents and caregivers of young children play a pivotal role in supporting healthy growth trajectories during infancy and preventing obesity during later life.8,9 During infancy, a primary driver of weight gain and obesity risk is infant feeding practices. 10 Thus, parents' and caregivers' first decisions related to infant feeding—choosing to feed breast milk vs. formula and from the breast vs. from a bottle—are important.
In particular, the composition of the milk fed to infants contributes to weight outcomes during infancy, with infants fed breast milk exhibiting healthier weight gain trajectories during the first year compared with infants fed conventional, cows' milk-based formulas. 11 Feeding mode—directly from the breast vs. from a bottle—likely also impacts feeding outcomes, with accumulating evidence suggesting that bottle-feeding may facilitate overfeeding and rapid weight gain for certain dyads, regardless of whether breast milk or formula is in the bottle.12,13 Indeed, a recent study demonstrated that infants who received the majority of milk feedings from a bottle (vs. directly from the breast) by 6 months postpartum exhibited greater weight-for-age z-score (WAZ) change during infancy compared with infants who received fewer milk feedings from a bottle (<30%). 14
Rapid weight change during early infancy is more strongly associated with later obesity than rapid weight change during later childhood, suggesting that infancy is a critical period for obesity prevention efforts. 15 However, previous research on associations between early feeding choices and weight outcomes has predominantly focused on the first year postpartum. More studies assessing associations between early feeding patterns, weight gain during the first year, and obesity risk later in childhood are needed.
The purpose of the present study was to examine the association between bottle-feeding during the first year postpartum and childhood obesity at 6 years old, as well as the potential mediating role of weight gain during the first year. As highlighted above, previous research illustrates associations between bottle-feeding and rapid weight gain during infancy 12 and between rapid weight gain and subsequent obesity. 7 Thus, we hypothesized that bottle-feeding would not be directly associated with obesity risk during later childhood but would be indirectly associated with the mediating factor of change in infant WAZ during the first year.
Participants and Methods
Study Population
The Infant Feeding Practices Study II (IFPS II) and its Year 6 Follow-Up (Y6FU) were conducted by the FDA and CDC, in collaboration with other federal agencies in response to the nation's continued need to understand and improve the health status of mothers and their offspring. The sample for IFPS II was drawn from a nationally distributed consumer opinion panel of ∼500,000 households. Detailed information about the study was described elsewhere. 16 In brief, IFPS II was a longitudinal study that included a cohort of pregnant women recruited between May 2005 and June 2007, during their third trimester. Participants were followed through the first postpartum year, with a total of 1 prenatal and 10 postpartum mail questionnaires sent at ∼1, 2, 3, 4, 5, 6, 7, 9, 10.5, and 12 months after birth.
In 2012, mothers from the IFPS II study were recontacted to participate in the Y6FU, a mail survey designed to follow-up with IFPS II children to assess their physical development, health condition, and dietary patterns at 6 years old. 17 The IFPS II had the following inclusion criteria: mothers aged 18 years or older at the time of the prenatal survey, singleton delivery of a full or nearly full-term infant (≥35 weeks of gestation), newborn's birth weight of ≥2.25 kg, both mother and infant were healthy at birth, and infants did not develop illnesses or conditions that would likely affect feeding.
Childhood Obesity Outcome
The weight and height measurements obtained from the Y6FU survey were based on self-reported data. Mothers were sent a measuring tape and instructions on how to measure their child's height and asked to report their child's height in inches. They were also asked to weigh their child on a scale without shoes and report the weight in pounds. BMI was calculated as weight (kg) divided by height in square meters. Because weight and height vary by sex and age, the sex- and age-specific BMI percentiles were calculated using the 2000 CDC Growth Charts. 18 A binary variable was then created for childhood obesity at age 6 years using 95th BMI percentile as the cutoff point (obesity: ≥95th percentile vs. without obesity: <95th percentile).
Mediator
Change in WAZ during the first year postpartum was proposed as a potential mediating variable between bottle-feeding patterns and childhood obesity at age 6 years. Mothers reported infants' birth weights through a short telephone interview that occurred within a week after birth. At each assessment thereafter, infants' weights were reported as the measured weights from their most recent doctor's visit at the 3-, 6-, 9-, and 12-month surveys. Weights were standardized to age- and sex-specific z-scores based on the 2006 World Health Organization Growth Standards.19,20
All infants included in the present study had data on birth weight and at least two other weight measurements, but the timing of these measurements varied from infant to infant. To maximize available data, we examined change in WAZ between birth and later infancy, defined as the difference between WAZ score from birth to the last weight assessment between 6 and 12 months of age (referred to from hereon as ΔWAZ from birth to later infancy). The majority of infants' last weight measurement was provided at the 12-month assessment (81%). To account for the possibility that ΔWAZ differed based on the age of the infant at the time of the last weight assessment, we included the time interval considered for each infant's ΔWAZ (referred to from hereon as ΔWAZ interval in months) as a covariate in all analyses.
Main Exposure Variable
Bottle-feeding intensity was defined as the percentage of daily milk feedings from a bottle (vs. breastfeeding, defined here as feeding directly from the breast). Bottle-feeding intensity was derived from a food frequency questionnaire that mothers completed for their infants at all postpartum assessments. Mothers were asked to recall their infant's diet during the past 7 days, with specific prompts focused on the frequency of consumption of breast milk, formula, and other milks (e.g., soy). In a separate part of the IFPS II survey, mothers were also asked to report the number of times in the past 7 days their infant was fed expressed breast milk (EBM). Mothers' responses to this question and the food frequency questionnaire were combined to determine the percentage of daily milk feedings that were breast milk from the breast (BF%), EBM%, and nonhuman milk (NHM%; including formula and other nonhuman milks). These percentages were estimated at each assessment, with BF%+EBM%+NHM% = 100% of daily milk feedings. Bottle-feeding intensity was then calculated as the proportion of milk feedings given by the bottle, regardless of whether EBM, formula, or other milks (e.g., soy, almond) were in the bottle (EBM%+NHM%). 21
Group-based trajectory modeling (GBTM) analysis was used to identify bottle-feeding intensity trajectories across the first year postpartum; results from this analysis were published previously. 14 In brief, GBTM is a data-driven approach, wherein finite mixture models are estimated to describe longitudinal trajectories of a variable of interest without a priori assumptions about the shape of trajectory curves or group membership.22–24 In this way, GBTM was used to characterize bottle-feeding intensity trajectories among IFPS II mothers 14 ; a strength of this approach is that it allowed for consideration of bottle-feeding intensity as a dynamic variable that changes across infancy, thus providing a more complex—and likely more accurate—characterization of bottle-feeding patterns. Of note, GBTM allows for estimation of models with missing data using maximum likelihood estimation under a missing at random assumption 25 ; thus, all available data for participants could be retained. To maximize validity of trajectories, GBTM was conducted with the full sample of IFPS II participants who had at least 3 (of 11 possible) data points for bottle-feeding intensity (n = 2648).
Models with 1–5 groups representing differing patterns of bottle-feeding intensities across the first year postpartum were estimated. 14 Model selection criteria [Bayesian Information Criterion (BIC), Sample-Size Adjusted BIC, Akaike Information Criterion (AIC), and Lo–Mendell–Ruben Likelihood Ratio Test (LMR-LRT)] 23 were lowest for 4- and 5-group models, but the 5-group model did not provide significant improvement over the 4-group model. In addition, the average of the posterior probabilities of group membership for individuals assigned to each group was high (>0.90) for the 4-group model, indicating good classification accuracy.23,26 Based on these fit criteria, the 4-group model was selected as the best fit for the data, and participants were classified into their most probable groups based on posterior probabilities.
Groups were then labeled based on the shape and nature of their bottle-feeding intensity trajectories: (1) the High-Stable Bottle Use group, which included mothers who reported ∼100% of milk feedings were from bottles at all assessments; (2) the Rapid Increase in Bottle Use group, which included mothers who reported ∼35% of milk feeding were from bottles during the neonatal assessment increasing to ∼100% of milk feedings by the 6 month assessment; (3) the Gradual Increase in Bottle Use group, which included mothers who reported ∼10%–20% of milk feedings were from bottles at early assessments and gradual increase in bottle-feeding intensity across the first year; and (4) the Low-Stable Bottle Use group, which included mothers who reported low levels of bottle-feeding intensity (<10% of feedings) until the 12 month assessment. Figure 1 presents the bottle-feeding intensity trajectories for each group.
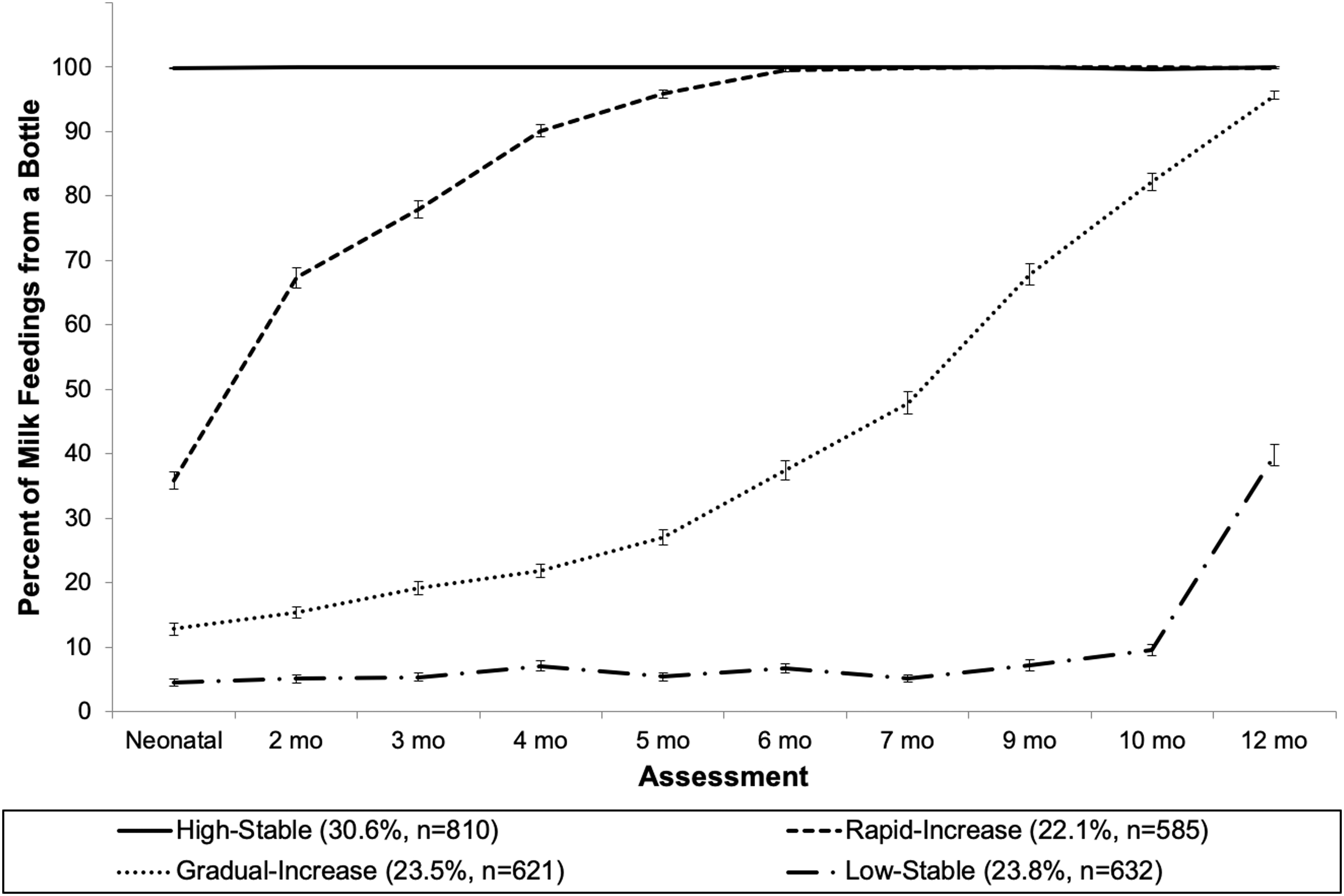
Bottle-feeding intensity trajectories derived from group-based trajectory modeling analysis of mother-reported bottle-feeding intensity across the first year postpartum. Bottle-feeding intensity calculated as (number of milk feedings from a bottle)/(total number of milk feedings). Milk was defined as breast milk, infant formula, cow's milk, or other milks (soy, almond, etc.). High-Stable: High-Stable Bottle Use group, which included mothers who reported ∼100% of milk feedings were from bottles at all assessments; Rapid-Increase: Rapid Increase in Bottle Use group, which included mothers who reported low levels of bottle-feeding intensity during the neonatal assessment increasing to ∼100% of milk feedings by the 6 month assessment; Gradual-Increase: Gradual Increase in Bottle Use group, which included mothers who reported low levels of bottle-feeding intensity at early assessments and gradual increase in bottle-feeding intensity across the first year; Low-Stable: Low-Stable Bottle Use group, which included mothers who reported low levels of bottle-feeding intensity (<10% of feedings) at the majority of assessments and a slight increase at 12 months.
Infant Eating Behaviors and Maternal Feeding Practices during Early Infancy
To further explore behavioral differences that may underlie associations between bottle-feeding intensity and childhood obesity at age 6 years, mediated by ΔWAZ from birth to later infancy, we assessed differences in infant-led bottle-emptying behavior and maternal encouragement of bottle-emptying among bottle-feeding intensity trajectory groups.
At each assessment, infant-led bottle-emptying, or the frequency to which an infant consumed all the milk in his or her bottle, was assessed by two questions: “How often does your baby drink all of his or her bottle of formula?” and “How often does your baby drink all of his or her cup or bottle of pumped milk?” Similarly, maternal encouragement of bottle-emptying, or the frequency to which a mother encouraged her infant to finish the bottle, was assessed by two questions: “How often is your baby encouraged to finish the bottle if he or she stops drinking before the formula is all gone?” and “How often is your baby encouraged to finish a cup or bottle if he or she stops drinking before the pumped breastmilk is all gone?”
Response options for all four of these questions ranged from 1 = Never to 5 = Always. At each assessment, mothers' responses to the formula and pumped milk versions of these questions were averaged to create infant-led bottle-emptying and maternal encouragement of bottle-emptying scores. The mean infant-led bottle-emptying and maternal encouragement of bottle-emptying scores over the first six postpartum surveys (a period when infants were predominantly fed breast milk or formula 27 ) were then calculated.
Covariates
The following covariates were included in all models. Mothers' characteristics were all obtained from IFPS II and included age at delivery, prepregnancy BMI (<18.5, 18.5–24.9, 25.0–29.9, and ≥30), race/ethnicity (white, black, Hispanic, other, or unknown), maternal education (less than high school, high school graduate, some college or more), marital status (yes or no for being married and cohabiting, or unknown), household income as percentage of federal poverty level (<185%, 185%–350%, >350%), and parity (primiparous, multiparous, or unknown). Infants' characteristics obtained from IFPS II included sex, gestational age in weeks, birth weight in kilograms, breastfeeding duration (≤16, 16 to <52, and ≥52 weeks), and age at introduction of complementary foods (CF; <4, 4 to <6, ≥6 months).
Breastfeeding duration was based on mothers' responses to IFPS II postpartum surveys unless they were still breastfeeding at the last IFPS II survey. In the case that the mother was still breastfeeding at the last IFPS II survey, answers to the Y6FU question “baby's last age in weeks when baby was breastfed” were used. Age at CF introduction was calculated as the midpoint between the infant's age when the mother reported no CF consumption and when she first reported her infant had consumed CF in the previous 7 days. CF included dairy foods other than milk (e.g., yogurt, cheese, ice cream); soy foods other than soy milk (e.g., tofu, frozen soy desserts); baby cereal; other cereals and starches (e.g., breakfast cereals, teething biscuits, crackers, pasta, rice); fruits; vegetables; French fries; meat, chicken, or combination dinners; fish or shellfish; peanut butter, other peanut foods, or nuts; eggs; and sweet foods (e.g., candy, cookies, cake). Additional child covariates were from Y6FU and included days per week that the child was physically active for at least 60 minutes, average minutes of daily screen time, and frequency per week of consuming sugar-sweetened beverages.
Statistical Analyses
A total of 1542 mother–child pairs were available in the study sample after linking Y6FU to IFPS II. We further sequentially excluded pairs with biologically implausible WAZ (<−6 or >5) at birth (n = 3), missing outcome variable (n = 132), implausible BMI z-score at year 6 (<−4 or >8, n = 28), missing main exposure variable (n = 82), missing mediator variable (n = 219), or missing covariates (n = 16). Note that two infants had biologically implausible WAZ for their last weight assessment between 6 and 12 months of age (at 12 months), but both of these infants did have plausible values at 6 months. Thus, for these two infants, WAZ at 6 months was used to calculate ΔWAZ from birth to later infancy. The final analytic sample consisted of 1062 observations.
To explore the association between bottle-feeding intensity during the first year postpartum and childhood obesity at age 6 years, we conducted causal mediation analysis. This analysis has been widely employed to examine the average direct effect of a main exposure variable (i.e., bottle-feeding intensity) on an outcome (i.e., childhood obesity at age 6 years), as well as the average causal mediation effect of a main exposure variable on an outcome through a mediator variable (i.e., ΔWAZ from birth to later infancy). 28 Several statistical packages in R, as well as a SAS macro, have been developed to facilitate application of this analytical approach in the fields of psychology, social, and biomedical sciences. 29
We first applied a multiple linear regression analysis with the mediator ΔWAZ from birth to later infancy regressed on bottle-feeding intensity, after adjusting for maternal and infant characteristics. We then applied a multiple logistic regression analysis with obesity status at age 6 years regressed on bottle-feeding intensity, after adjusting for all the covariates and the mediator, ΔWAZ from birth to later infancy. To estimate the average direct effect of bottle-feeding intensity on childhood obesity at age 6 years and the average causal mediation effect of ΔWAZ from birth to later infancy, the parameters from the multiple linear regression and from the multiple logistic regression were combined using methods previously described. 30
The proportion of the effect of bottle-feeding intensity mediated by ΔWAZ from birth to later infancy was calculated on a risk difference scale by
To further explore behavioral differences between bottle-feeding intensity trajectory groups at differing risk for greater ΔWAZ from birth to later infancy and obesity at age 6 years, general linear models with planned comparisons were used to examine group differences for infant-led bottle-emptying and maternal encouragement of bottle-emptying during the first 6 months of infancy. All aforementioned covariates were included in these models.
Two-sided p-values were used with statistical significance set at p < 0.05. All analyses were performed in SAS version 9.4 and R version 3.5.0. R mediation package version 4.4.6 was used for obtaining direct, indirect, and total effects of bottle-feeding intensity on childhood obesity at age 6 years. 31
Results
Sample characteristics are summarized in Table 1. Table 2 summarizes the results of regression models predicting ΔWAZ from birth to later infancy and childhood obesity at age 6 years. With respect to predicting ΔWAZ from birth to later infancy, infants in the Rapid Increase in Bottle Use group had significantly greater ΔWAZ from birth to later infancy compared with infants in the Low-Stable Bottle Use group (β = 0.46, 95% CI 0.11–0.80). In the model predicting childhood obesity at age 6 years, the only significant predictors of obesity were larger birth weight [adjusted odds ratio (AOR) = 4.27, 95% CI 2.42–7.64] and larger ΔWAZ from birth to later infancy (AOR = 1.59, 95% CI 1.29–1.98).
Percent (n) or Mean (SD) for Sample Characteristics (N = 1062)
Defined as BMI percentile ≥95th.
Defined as the difference between WAZ from birth to the last weight assessment between 6 and 12 months of age.
BMI, body mass index; CF, complementary foods; PIR, poverty–income ratio; WAZ, weight-for-age z-score.
Regression Analyses Predicting ΔWAZ during the First Year a and Child Obesityb at Y6 Assessment (N = 1062)
Defined as the difference between WAZ from birth to the last weight assessment between 6 and 12 months of age. bDefined as BMI percentile ≥95th.
Bolded estimates were significant at p < 0.05.
AOR, adjusted odds ratio; BMI, body mass index; CF, complementary foods; CI, confidence interval; PIR, poverty-income ratio; WAZ, weight-for-age z-score; Y6, Year 6.
Mediation analyses testing for the average indirect effect of bottle-feeding intensity trajectory group membership on childhood obesity at age 6 years, mediated through ΔWAZ from birth to later infancy, revealed a significant average causal mediation effect of larger ΔWAZ from birth to later infancy in the Rapid Increase in Bottle Use group (Table 3 and Fig. 2). Fifty-nine percent of the total effect for the Rapid Increase in Bottle Use group on childhood obesity at age 6 years came from the average causal mediation effect through ΔWAZ from birth to later infancy. There was no interaction between bottle-feeding intensity trajectory group membership and ΔWAZ from birth to later infancy on childhood obesity risk at age 6 years (p = 0.97).
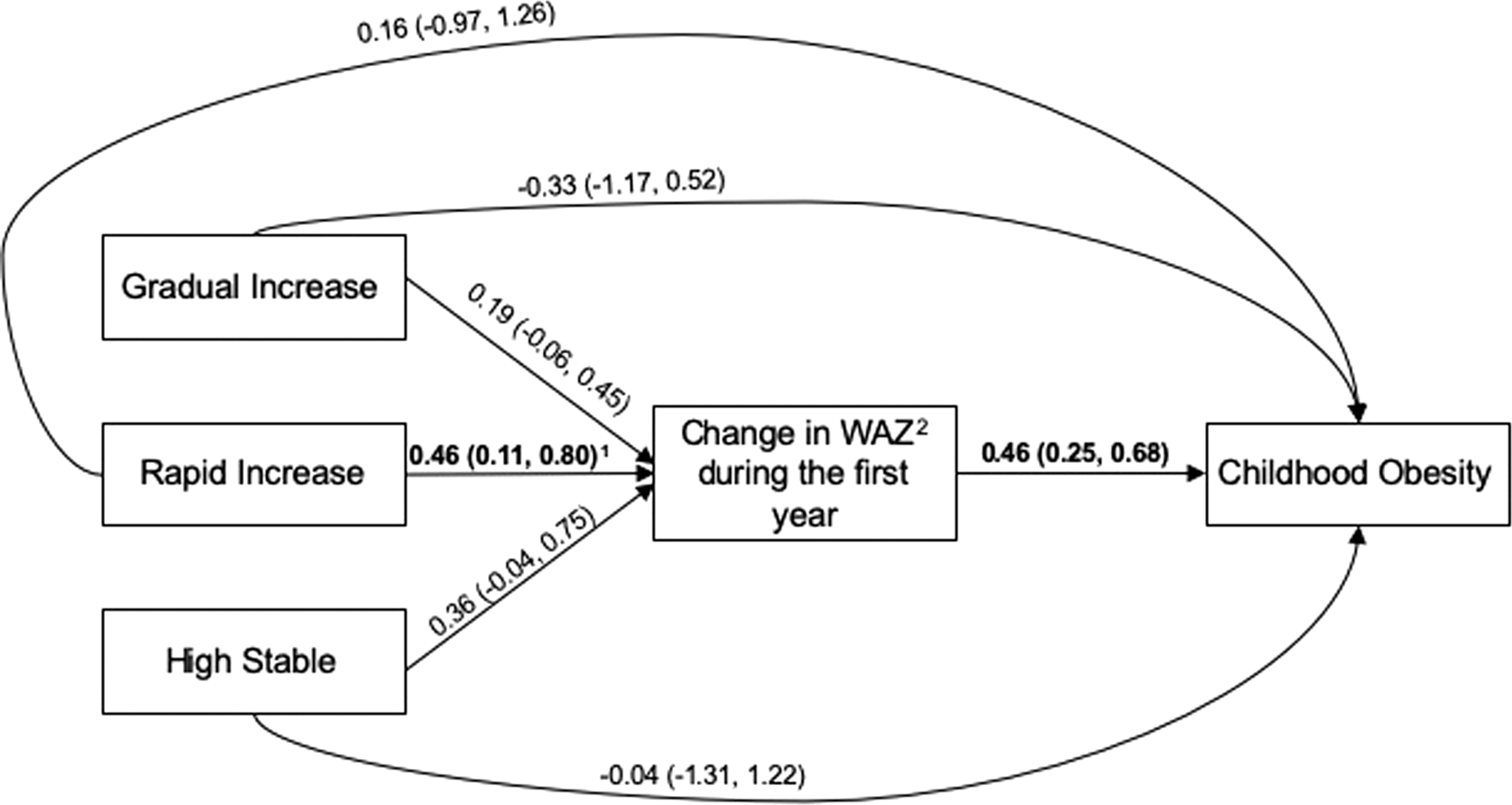
Estimated coefficients from mediation analysis predicting obesity risk at Year 6 assessment with change in WAZ as the mediator, and the trajectory group as the exposure variable, where the Low Stable is the reference group. Estimated coefficients along with 95% confidence intervals corresponding to the numbers are reported in Table 2. 1 Bolded estimates significant at p < 0.05; 2 WAZ, weight-for-age z-score.
Mediation Analysis Predicting Obesity a Risk at Y6 Assessment (N = 1062)
Defined as BMI percentile ≥95th.
Adjusted for maternal characteristics: maternal age, prepregnancy BMI, race/ethnicity, maternal education, marital status, PIR level, parity; child characteristics: sex, gestational age, birth weight, breastfeeding duration, age at CF introduction, duration from birth to the last weight assessment between 6 and 12 months of age, days per week physically active at 6 years old, average minutes of daily screen time at 6 years old, and frequency per week sugar-sweetened beverages were consumed.
Mediator was ΔWAZ during the first year, defined as the difference between WAZ from birth to the last weight assessment between 6 and 12 months of age.
Bolded estimates were significant at p < 0.05.
AOR, adjusted odds ratio; BMI, body mass index; CF, complementary foods; CI, confidence interval; PIR, poverty-income ratio; WAZ, weight-for-age z-score; Y6, Year 6.
Comparisons between the bottle-feeding intensity trajectory groups indicated that infants in the Rapid Increase in Bottle Use group more frequently emptied the milk in the bottles (
Discussion
Findings from the present study illustrate an indirect association between bottle-feeding intensity during infancy and risk for obesity at age 6 years, mediated by greater weight gain during the first year. Although a large and growing body of research illustrates that bottle-feeding is a significant predictor of rapid weight gain12,14 and rapid weight gain during the first year of life is a strong predictor of later obesity, 7 the present study adds to this body of research by connecting these dots with a longitudinal prospective study and decomposing the total effect of bottle-feeding on childhood obesity into direct and indirect effects mediated through change in WAZ from birth to infancy. It illustrates, comprehensively, that infants who experienced rapid increases in bottle-feeding intensity during the first 6 months exhibited a greater change in WAZ across the first year compared with infants who experienced consistently lower levels of bottle-feeding, which was subsequently predictive of significantly greater risk for obesity at age 6 years.
It is important to note that the focus of the present study was on bottle-feeding and not milk type, per se, yet the effects of bottles vs. effects of formula on WAZ change during infancy and risk for obesity at age 6 years could not be determined or separated given the correlational nature of the study design and the high correlation between use of bottles and use of formula (data not shown). However, breastfeeding duration was controlled for in models predicting WAZ change during the first year and risk for childhood obesity at age 6 years. Since breastfeeding duration represented the age when infants completely stopped breastfeeding or receiving pumped milk, controlling this variable in the model could account for potential effect of milk type on WAZ change, to some extent. Given both milk type32,33 and feeding mode12,34 are predictive of risk for rapid infant weight gain and later obesity, our findings may represent a synergistic effect of these two factors, rather than solely an effect of feeding mode. Further research using causal designs and analytical approaches to parse out the independent and synergistic effects of milk type and feeding mode is warranted.
Analysis of behavioral differences between infants who experienced rapid increases in bottle-feeding intensity during the first 6 months (the Rapid Increase in Bottle Use group) and infants who experienced consistently lower levels of bottle-feeding (the Low-Stable Bottle Use group) illustrated that infants in the Rapid Increase in Bottle Use group more frequently emptied the bottle and their mothers more frequently encouraged them to finish the bottle during early infancy. Previous research has used infant-led bottle-emptying as a proxy for low satiety responsiveness and poor self-regulation of milk intake for infants13,35 and maternal encouragement of bottle-emptying as a measure of pressuring feeding practices for mothers.13,36 Thus, these behavioral differences noted in the present study may represent differences in responsive eating by infants or responsive feeding by mothers that led to overfeeding, greater WAZ change, and subsequent risk for obesity for infants in the Rapid Increase in Bottle Use group. In a previous study, mothers who reported increases in their bottle-feeding intensity during early infancy also exhibited concurrent increases in the frequency to which they encouraged their infants to finish the bottle, suggesting that the shift from predominantly feeding from the breast to predominantly feeding from a bottle is accompanied by changes in feeding practices. 36 However, due to the correlational nature of these data, it is unclear whether mothers' perceptions of their infants' appetitive traits and weight gain37,38 and/or desire for increased control during feeding39,40 drove decisions to breastfeed vs. bottle-feed, or whether increased use of bottles influenced infants' eating behaviors and/or mothers' tendencies to exert more control over the feeding interaction. 41 Further research is needed to better understanding the direction of these associations and key drivers of overfeeding during early infancy.
Study limitations highlight opportunities for future research. Although the IFPS II included mothers and infants from across the United States, the sample demographics were not nationally representative. Additionally, mothers who completed the study were significantly older, had higher socioeconomic status, and were more likely to be non-Hispanic white, married, and intending to breastfeed compared with mothers who did not complete the study (data not shown), 14 which may limit generalizability of these findings. Weight measurements were reported by mothers within both IFPS II and Y6FU studies, which may have led to some reporting bias. As discussed above, the ability to parse out effects of milk type vs. feeding mode were limited due to the correlational nature of the study design and the high correlation between bottle-use and formula-use.
In addition, because this was a correlational study, we could only assess associations between bottle-use, infant weight gain, and childhood obesity risk; further research using causal designs is needed to understand the direction of effects (e.g., whether increases in bottle-use lead to greater infant weight gain or whether greater infant weight gain leads to increases in bottle-use). Finally, it is possible that our estimates of direct and indirect effects were biased because we used a multiple logistic regression model for a common binary outcome 28 ; a log-binomial model would have been a more desirable approach, but this type of model did not converge in our preliminary analyses. However, a recent simulation study examining the bias and efficiency of different mediation analysis methods using logistic regression suggested any bias would be minimal.49 Overall, further research with larger, more diverse, and representative samples, as well as additional measures of maternal and infant characteristics and objective measures of child weight status and growth will provide further insights into associations between early feeding patterns, risk for overfeeding and rapid weight gain, and later obesity risk.
Conclusions
Significant increases in bottle-use during the first 6 months postpartum were directly associated with greater weight gain during the first year and indirectly associated with obesity risk at age 6 years via the mediating effect of larger gain in WAZ during infancy. Additional research is needed to understand how infant self-regulation, maternal feeding practices, milk composition, and feeding mode interact to influence early feeding decisions and later feeding outcomes. Primary prevention efforts to support and protect mothers' abilities to breastfeed their infants directly from the breast as much as possible during early infancy are needed. In addition, evidence-based secondary prevention efforts to reduce risk for overfeeding may impact obesity risk for bottle-fed infants.
Disclaimer
The findings and conclusions of this report are those of the authors and do not necessarily represent the official position of the CDC.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.