
Abstract
Background:
Excessive weight gain in the first 2 years of childhood is a risk factor for future obesity. However, the current absence of clear, standardized identification and treatment guidelines may hinder primary care providers' (PCPs) ability to manage early excessive weight gain in children <2. The objective of this study was to explore PCPs' perspectives on evaluating and communicating about early excessive weight gain and to identify PCP-opined barriers to the care of children exhibiting such trends.
Methods:
A trained interviewer conducted 20 semistructured interviews with PCPs on identifying and communicating with families about early excessive weight gain in children <2 years old. A thematic analysis approach was used to analyze the transcripts.
Results:
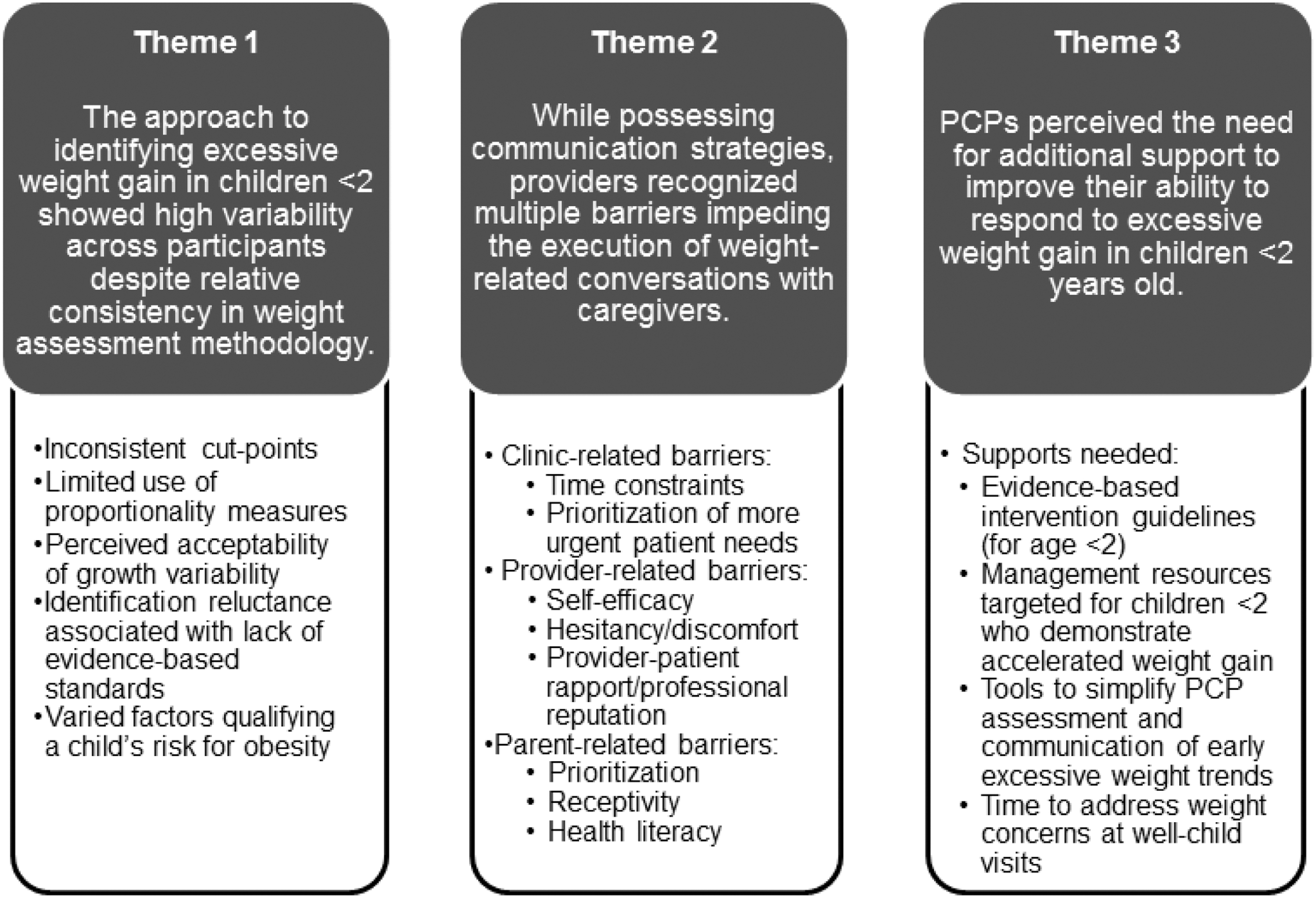
Interviews uncovered three major themes: (1) the approach to identifying excessive weight gain in children <2 showed high variability across participants despite relative consistency in weight assessment methodology, (2) while possessing communication strategies, providers recognized multiple barriers impeding the execution of weight-related conversations with caregivers, and (3) providers perceived the need for additional support to improve their ability to respond to excessive weight gain in children <2 years old.
Conclusions:
Variability exists in PCP-reported methods used and barriers faced when identifying, communicating, and responding to excessive weight gain in very early childhood. Introducing guidelines and resources to help standardize the assessment and communication of excessive weight gain in children <2 could augment PCPs' strategies for managing accelerated weight-gain trajectories to mitigate rates of childhood obesity.
Introduction
Childhood obesity is a widespread epidemic. 1 For some, excessive weight status starts in very early childhood; an estimated 8.1% of US children <2 years old have a weight-for-length ≥95%. 2 While numerous in utero (e.g., excessive gestational weight gain) and early life (e.g., birth weight) influences are important potential risk factors for future obesity,3,4 increasing evidence suggests that excessive weight gain before age 2 years augments a child's risk for later obesity.5,6 Because excessive early childhood weight gain is potentially modifiable, addressing it in the well-child setting may be an important part of attenuating the childhood obesity epidemic. 7
Despite clear guidelines for addressing excessive weight gain in children ≥2 years of age,8,9 primary care providers (PCPs) often delay management, failing to attend to escalating weight trajectories or discuss trends with families.10–12 For children <2 years old, delays and barriers impacting PCP management of excessive weight trajectories are likely magnified due to limited evidence and unclear management guidelines focused on this patient age group.
Although evidence linking early excessive weight with subsequent poor health outcomes exists,5,6 most current research has targeted prevention with limited focus on early weight-gain treatment interventions.7,13 As for guidelines addressing obesity in children <2, while the American Academy of Pediatrics (AAP), Institute of Medicine, and Endocrine Society advocate for weight-for-length screening and the World Health Organization provides BMI charts starting at birth, inconsistencies across guidelines and variability among recommended cut-points (differentiating healthy from unhealthy weight gain) likely complicate and therefore hinder PCPs' assessment and management strategies.8,9,14–17 Altogether, when addressing excessive weight gain in children <2, the limited evidence compounded by the current lack of clear, standardized strategies for identifying and treating excessive rates of weight gain may amplify the known challenges PCPs face when treating pediatric obesity and compromise PCPs' ability to assess, communicate, and care for very young children exhibiting early trends toward obesity. 14
Considering the limited evidence regarding management of early excessive weight gain and the varied existing guidance on this topic, the goal of this study was to understand the strategies and obstacles currently impacting PCP identification and communication of excessive weight gain in children <2. Because little is known about how PCPs are addressing this issue in clinical practice, we sought to explore, using qualitative methods, the perspectives of PCPs on their process for evaluating early childhood weight gain, their approach to communicating with parents about early excessive weight gain, and perceived barriers to caring for such children. In an area where evidence is currently lacking, understanding practitioners' processes and related barriers guiding the assessment and management of weight-gain velocities in children <2 could help inform future efforts aimed at treatment of excessive weight gain during the first 2 years of life.
Methods
Design
This study used a qualitative descriptive approach as described by Sandelowski18,19 to explore PCPs' perceptions about methods used to identify and communicate with families about weight trajectories in children <2 years old. This approach allowed for a comprehensive summary of participants' experiences and perspectives utilizing a low-inference approach to interpretation (i.e., participant statements were interpreted at face value with limited inferred meaning). The Colorado Multiple Institutional Review Board approved this study as exempt.
Participants
Participants were pediatricians, nurse practitioners, or physician assistants who met eligibility criteria of conducting at least 1 well-child visit/week for children <2 years old. Both purposive sampling (i.e., sampling to represent the views of providers in different states) and snowball sampling (i.e., participants sharing the research invitation with their colleagues) were utilized to recruit participants.
The research team created a list of potential participants known to the researchers at locations across the United States. Listed individuals were e-mailed a letter inviting them to participate in a study designed to explore methods and barriers to identifying and communicating about weight gain in children <2. E-mail recipients were asked to disseminate the invitation to other practitioners providing pediatric well-child care. Recruitment continued until saturation of thematic content, indicated by reemergence of the same themes and absence of new codes or themes across interviews.20,21
Data Collection
A semistructured interview guide was developed based on existing recommended intervention domains for obesity prevention and early treatment for children ≥2 in the primary care clinic, including: (1) assessment (evaluation of growth patterns, diet, and activity) and (2) communication (delivery of anticipatory guidance to caregivers related to child's weight, diet, physical activity, and behavior patterns). 8 Interview guide questions focused on PCP methods for and barriers to identifying and communicating with families about excessive weight gain in children <2 years (Appendix A1).
In-depth semistructured phone interviews were conducted from October 2017 to February 2018 by a nonpracticing general pediatrician trained to conduct qualitative interviews (L.M.A.). The majority (80%) of the participants had never previously interacted with the interviewer. Following an informed consent process, the interviewer administered demographic questions followed by open-ended questions. Follow-up questions were used to prompt further details and elicit response clarification. Interviews ranged in the duration from 25 to 60 minutes and participants were issued a gift card following interview completion. All interviews were audio recorded and transcribed verbatim. Identifying information was removed from the transcripts.
Data Analysis
A thematic analysis methodology, which is “a method for identifying, analyzing, and reporting patterns (themes) within data,” 22 was used to examine the transcripts using an inductive approach, as described below. The authors, both pediatricians not currently working in general pediatric clinics, read three transcripts and manually tagged the content, noting statements that were interesting or meaningful, from which they developed an initial codebook. The codebook was then further developed through an iterative process of independently reviewing the transcripts and tagging interesting content followed by jointly discussing the content, identifying codes, and then independently applying the codes to the transcribed material. Codes were refined throughout this process and finalized after establishing strong code assignment agreement.
Subsequently, the two researchers independently coded each transcript. Coding discrepancies were resolved by consensus. ATLAS.ti (v.8.1.3) was used for data organization and management. Through joint review of the data and in-depth discussions, the researchers thematically analyzed the coded data to find patterns and identify developing themes emerging from the data. Across the code set, themes were identified and notable quotes were highlighted.
Results
Participant characteristics are shown in Table 1. Sixteen participants (80%) identified as pediatricians and 4 (20%) as advanced practice providers. Primary care experience ranged from 1 to 29 years. The median number of well-child visits conducted per week for children <2 was 25 (n = 19).
Characteristics of Participants Completing Semistructured Interviews on Early Childhood Growth (n = 20)
Eleven participants (55%) practiced in continuity-based clinics in academic or hospital settings and the remainder (n = 9, 45%) worked in community or multispecialty groups. Participants' practices were in the western (n = 7, 35%) and the midwestern (n = 13, 65%) portions of the United States.
Three themes were identified from the interviews. Representative quotes for each theme are in Table 2; quotes within each theme are derived from different interviews. Findings are also shown in Figure 1.
Sample Quotes by Theme from Interviews with Pediatric Primary Care Providers (n = 20)
Theme 1: The Approach to Identifying Excessive Weight Gain in Children <2 Showed High Variability across Participants Despite Relative Consistency in Weight Assessment Methodology
Varying differentiating cut-points for excessive weight gain and trajectories
All participants reported use of assessment methods, including regular monitoring of weights and lengths for the purpose of evaluating and tracking weight gain for children <2 years old. Providers ubiquitously used weight and length growth charts to track weight-for-age and length-for-age for children <2. Yet, cut-points differentiating healthy from excessive weight gain for children varied across providers. Several providers designated excessive weight gain when weight-for-age percentiles surpassed the 95th percentile or when weight-for-age trajectories upwardly crossed two major growth curve percentile lines (especially when crossing the 95th percentile).
Proportionality data (i.e., weight-for-length or BMI) were utilized inconsistently, with several PCPs citing the perceived unreliability of length measurements as the rationale for forgoing proportionality measures in the assessment of weight gain for children <2. Only a few providers considered proportionality data (e.g., weight-for-length >95th percentile) when designating excessive weight gain in children <2. Several PCPs reported using visual cues as an adjunct tool for evaluation of a child's weight status.
Although some providers had set cut-points defining excessive weight gain, many providers expressed concerns about using growth chart data to differentiate healthy from excessive weight gain for children in this specific age group. Concerns included the following: (1) acceptability of growth variability in children <2 (especially in breastfed children), (2) lack of evidence-based data on the predictive value of growth chart trajectories in this age group, and (3) lack of evidence-based standards for identifying excessive weight gain for children <2.
Factors heightening providers' concern about excessive early childhood weight-gain velocity
Independent of a child's anthropomorphic measurements, most participants used an assessment strategy to qualify a child's susceptibility to accelerated weight-gain trajectories. Factors perceived as indicative of obesity risk fell into three major categories: (1) individual child factors, (2) parent factors, or (3) environmental factors.
Specific to the individual child, providers' level of concern for future obesity increased with advancements in a child's age. Many providers delayed assessment of weight-gain trajectories until children were >1 or >2 years of age, with several PCPs qualifying their identification reluctance rationale with predictions that the forthcoming age-associated advancement in mobility would interrupt trends toward obesity for children <2.
Pertaining to a child's immediate family, providers' level of concern for a child's risk for the development of obesity increased when a parent had a history of obesity, expressed a dismissive attitude toward weight, or perceived normalcy of an obese phenotype. Provider level of concern also increased according to environmental factors, including a lower socioeconomic status, multiple child caregivers, and perceived cultural preferences for an obese phenotype. Together, these child-focused, parent-focused, and environmentally focused factors modified most providers' level of concern about a child's weight status and augmented providers' determinations of whether a weight or weight trajectory warranted further management for a child <2.
Theme 2: While Possessing Communication Strategies, Providers Recognized Multiple Barriers Impeding the Execution of Weight-Related Conversations with Caregivers
Utilized communication strategies
Providers possessed methods to communicate pediatric weight-related concerns with parents of children <2. Many providers used motivational interviewing techniques for weight-related conversations, focusing on the following: (1) developing a relationship with the parent, (2) assessing parental perceptions on weight, (3) determining parental perceived responsibility related to their child's weight, and (4) establishing parental readiness to modify weight-related behaviors. Most providers emphasized the importance of conducting discussions with sensitivity to weight-related verbiage in an effort to avoid offending parents.
Recognized communication barriers
All providers recognized clinic-, provider-, and parent-associated barriers to conducting weight-related discussions with parents of children <2 with excessive weight gain. Time constraints or prioritization of more urgent patient needs were commonly reported as clinic-associated factors compromising PCP ability to conduct weight-related discussions with families at well-child visits. Specific to the provider, identified communication barriers included a PCP's: (1) perceived low self-efficacy to conduct weight-related discussions, (2) hesitancy to discuss the topic of weight, (3) discomfort in conveying potential long-term consequences of early childhood weight gain, (4) concern for jeopardizing provider/parent rapport, and (5) concern for compromising the professional reputation (e.g., patient satisfaction reports) by conducting weight-related conversations.
PCPs also identified communication barriers associated with parents, including perceived parental (1) prioritization of immediate concerns above weight issues, (2) lack of openness to the topic of early childhood unhealthy weight gain, and (3) level of health literacy. Providers reported that many of these barriers led to delays in communicating about excessive weight gain with families of children <2.
Theme 3: PCPs Perceived the Need for Additional Support to Improve Their Ability to Respond to Excessive Weight Gain in Children <2 Years Old
Providers discussed the need for additional tools to support the early management of excessive weight trends in children <2. Some providers felt that evidence-based guidelines recommending when and how to intervene on excessive weight gain for children <2 would improve their ability and self-efficacy to address early trends toward obesity. Many providers cited the lack of management resources for very young children with excessively escalating weight trajectories, and almost all reported the need for additional time to address weight concerns at well-child visits. A few providers suggested the need for specific, but different, tools (e.g., growth charts aligning color-coded designations with growth rates) to simplify assessment and communication related to excessive weight gain in this age group.
Discussion
Little is known about PCPs' strategies for addressing excessive weight gain in children <2 years of age despite existing evidence delineating various challenges impacting obesity management in older children (≥2).10–12 Based on evidence suggesting that early weight trends predict future risk of developing obesity5,6 and the role of PCPs in providing lifestyle-oriented primary management for children ≥2 with obesity, 8 this study gathered the opinions of PCPs regarding methods used and barriers faced when identifying and communicating with families about excessive weight gain specific to children <2.
Not surprisingly, many of the findings from this study overlap with findings of previous research focused on PCP management of excessive weight velocities in children ≥2 (e.g., clinical time constraints, parent prioritization).10–12 However, this study identified numerous challenges that may add unique complexity to efforts addressing excessive weight gain in children <2.
A multitude of factors may complicate the identification of escalating weight trajectories for children <2. In this study, PCPs reported inconsistent approaches to the identification of excessive weight and weight gain for children younger than the age of 2.
Although participants described regularly assessing diet, weight-for-age, and length-for-age in this age group, few reported consistently assessing growth proportionality (either weight-for-length or BMI-for-age) or using a weight-for-age cut point to identify an excessive weight or abnormal weight-gain velocity. Concerns about the reliability of length measurements 23 as well as the general acceptance of weight variability in this age group (especially in younger infants and breastfed babies) may have contributed to the inconsistent focus on numeric growth indicators. The use of visual assessments may also reduce a PCP's level of concern despite evidence suggesting that visualization alone is suboptimal for discerning weight status. 24
Overall, inconsistent risk stratification guidance from leading health organizations (with varied screening and cut point recommendations to differentiate healthy from unhealthy measures of growth in children <2) may be limiting PCPs' assessment of weight gain in very early childhood.14,25 These myriad of factors potentially diminish PCPs' confidence or clarity in assessing weight-gain trajectories and stratifying risk in the <2 age group, thereby compromising PCPs' identification and assessment of early childhood weight trends potentially predisposing to subsequent obesity.
Further complicating PCPs' strategies to address excessive weight or weight trajectories in children <2, existing treatment guidelines to positively impact childhood weight outcomes are specifically designated for children ≥2.8,15 PCPs lack guidance for managing weight trends that emerge before age 2.
Without treatment guidelines to apply to children <2, providers deciding to intervene on early excessive weight gain appeared to be extending the obesity management techniques established for children ≥2 to the <2 population (e.g., utilizing the AAP-endorsed motivational interviewing strategy to encourage provider/parent communication to modify lifestyle behaviors associated with obesity risk). 9 Empowering PCPs with strategies to communicate risk and direct caregivers regarding dietary behavior change (irrespective of child age) could encourage PCPs' advancement of parental self-efficacy and ultimately serve to modify behaviors associated with obesity risk for children <2. 26
Although the importance of early intervention was recognized by study participants, many opted to wait until a child was 2 years or older before initiating obesity-related discussions or management. PCPs need specific strategies to apply to children <2 with excessive weight or weight gain to avoid assessment and management delays and potentially mitigate the future health risk to affected children.
Participants requested standardized guidelines and additional tools directed at children in this age group, which may help address current gaps in care, steer assessment, and ultimately discourage postponement of management. Resources to address excessive weight and weight gain in children <2 could enhance PCP confidence when responding to early excessive rates of weight gain (including discriminating monogenic/polygenic/syndromic etiologies from other causes of weight gain), helping PCPs overcome low levels of provider self-efficacy for responding to excessive weights during early childhood currently described in numerous prior studies.10,12,27
Several tools are currently available to optimize dietary intake, including AAP responsive feeding parent information, 28 the Pregnancy and Birth to 24 Months (P/B-24) project, 29 and responsive feeding guidelines. 30 Future availability of additional tools and resources could improve PCP self-efficacy in managing early childhood weight status, potentially translating into an enhanced ability for PCPs to mitigate excessive escalation of weight trends among children <2. While evidence supports the connectivity of early excessive weight gain with future obesity risk,5,6 a paucity of guidelines, strategies, and tools tailored to this age group appears to hinder pediatric PCPs' ability to disrupt trends toward obesity during the earliest stages of abnormality.
A few limitations of the current study warrant mention. First, the recruitment approach used to identify the 20 study respondents may limit the generalizability of the findings, with all respondents representing practices in the western and midwestern United States, and 55% describing work in academic or hospital-affiliated practice settings. Moreover, recruitment may have selected for respondents with a heightened interest in managing early childhood weight gain, effectively overestimating provider self-efficacy and underestimating the need for heightened support. Second, although the qualitative nature of this study has numerous strengths, including the ability to explore provider perceptions on this topic, additional research is needed to understand the prevalence of these findings across pediatric providers. Last, this study focused exclusively on opinions related to early excessive weight gain without explicitly addressing the consequence of high birth weight. Weight-gain velocity is a well-established risk factor for obesity5,6 and was selected as the focus in this study to inform efforts to address PCP responsiveness to early excessive weight gain.
Conclusions
Early rapid weight gain is a risk factor for later obesity.5,6 PCPs are well-positioned to assess and manage early excessive weight-gain trends. Findings from this study suggest that PCPs face unique challenges when caring for children <2 with excessive rates of weight gain, compounding the numerous known challenges encountered in the management of excessive weight gain or weight velocity in older children.
To maximize early intervention strategies, PCPs need tools to improve their identification criteria, communication strategies, and management approaches for excessive weight gain in children <2. To support this, evidence promoting early risk stratification as well as the impact of early treatment is also needed. Interrupting early trends toward obesity has the potential to reduce long-term morbidity and mortality. 31 Further work addressing this topic is critical to prevent delays in care and improve health outcomes for children with early excessive weight gain.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.