
Abstract
Background:
Few studies have published mediation analyses to quantify the role concurrent BMI plays in the relationship between growth and cardiometabolic risk (CMR) outcomes.
Methods:
We used data from a longitudinal cohort study conducted in children aged 0–60 months through The Applied Research Group for Kids (TARGet Kids!) in Canada. Four age and sex standardized BMI (zBMI) trajectories were identified using latent class mixed models. CMR were assessed using a CMR score. Concurrent zBMI was the zBMI measured on the same visit as CMR. Mediation analyses were performed comparing each trajectory with the reference trajectory.
Results:
One thousand one hundred sixty-five children were included. On average, compared with being in the stable low trajectory, being in the catch-up trajectory was associated with an increased CMR score of 0.42, 0.28 of which was mediated through concurrent zBMI [95% confidence interval (CI) 0.17 to 0.41, p = 0.001]; being in the stable high trajectory was associated with an increased CMR score of 0.23, 0.24 through concurrent zBMI (95% CI 0.18 to 0.31, p < 0.001). Similarly, being in the rapid accelerating trajectory was associated with an increased CMR score of 1.43, 1.18 of which was through concurrent zBMI (95% CI 0.89 to 1.50, p < 0.001).
Conclusions:
There was a strong evidence that the effect of BMI trajectories on CMR was indirect via concurrent BMI. It is important for researchers to choose the most appropriate analytic method based on the study hypothesis to understand the total or direct effect of growth patterns on cardiometabolic disease risk in children.
Introduction
Childhood obesity is a global public health concern. 1 Children with obesity are at increased risk of cardiometabolic diseases and obesity in adolescence and adulthood.2–4 Rapid childhood growth, often assessed using repeated measures of height, weight, or BMI, is associated with later adverse cardiometabolic outcomes.5–13 Cardiometabolic risk (CMR) is a composite measure for monitoring children's cardiovascular and metabolic risk, including obesity, hypertension, hyperglycemia, and dyslipidemia. 14 Studies by our group15,16 and others5–13,17–22 have suggested that rapid growth during childhood and adolescence is associated with higher CMR, including larger waist circumference (WC)8,11,16 and higher systolic blood pressure (SBP).5–7,15
There are variations in researchers' approaches when addressing BMI measured concurrently with CMR outcomes. Some studies did not include concurrent BMI in any of their models,23,24 while most of the studies used a stepwise approach.6,7,15,17–22,25 They first assessed the association between growth and CMR outcomes without including concurrent BMI in the model, and then included concurrent standardized BMI (zBMI) as a confounder by adjusting for it in a separate model.6,7,15,17–22,25 After the further adjustment, except for two studies,6,21 most studies found that the association either attenuated or disappeared entirely compared to their previous models without adjusting for concurrent zBMI.7,15,17–20,22,25
As demonstrated by the attenuation of the associations shown in these studies7,15,17–20,22,25 and a review by Tu et al., 26 concurrent BMI is recognized as a mediator, rather than a confounder, of the relationship between BMI trajectories and CMR. Different approaches have been used to address concurrent BMI in the relationship between growth and CMR outcomes, producing different results. To our knowledge, few studies have published mediation analyses to quantify the intermediate role concurrent BMI plays in the relationship between growth and CMR. 27 Quantifying the role of concurrent BMI may help elucidate the effect of growth patterns on CMR and inform our understanding of the impact of growth patterns on chronic disease risk in children.
The objective of this study was to determine the extent to which age and sex zBMI concurrent with CMR score was a mediator in the relationship between growth trajectories and CMR, by performing a mediation analysis using longitudinal data from an ongoing cohort study. We hypothesized that concurrent zBMI largely mediates the relationship between zBMI trajectories and CMR in young children.
Methods
Study Design and Participants
We used data from a longitudinal cohort study conducted in children aged 0–60 months through The Applied Research Group for Kids (TARGet Kids!) in Canada between December 2008 and October 2018. 16 TARGet Kids! is the largest practice-based research network in Canada, enrolling healthy children from primary health care settings and following them into adolescence. 28 BMI measurements were taken at various time points during participants' well-child visits, and standardized using the WHO Growth Standards. 29 All available BMI data (n = 9908, with 60,297 observations) were used to estimate the latent zBMI trajectories and subjects with at least two measures of zBMI were included in the analysis between zBMI trajectories and CMR score (n = 1166).16,30–32 Among the 1166 participants eligible for analysis, 1 child was excluded as the participant's concurrent zBMI was missing (n = 1165). Parents of all participating children provided written informed consent. This study was approved by the Research Ethics Boards at The Hospital for Sick Children and St. Michael's Hospital (Registered at www.clinicaltrials.gov; NCT01869530).
zBMI Trajectories, CMR Score, and Concurrent zBMI
zBMI trajectories in children 0–60 months were estimated using latent class mixed modeling based on our previous study using the lcmm package in R.16,33 Bayesian Information Criterion (BIC), Akaike Information Criterion (AIC), mean posterior probabilities, entropy, and interpretability were used to select the optimum model. 16 Four trajectories were identified: a catch-up trajectory (trajectory 1; n = 47, 4.0%), a stable high (trajectory 2; n = 269, 23.1%), a stable low trajectory (trajectory 3; n = 838, 71.9%), which was the reference trajectory, and a rapidly accelerating trajectory (trajectory 4; n = 12, 1.0%). 16 Each trajectory was named based on its visual appearance. 16
The CMR outcome was assessed using a continuous CMR score quantified as the sum of age- and sex-standardized WC, SBP, blood tests for glucose, log-triglycerides, and the negative of high-density lipoprotein cholesterol (HDL-C), divided by the square root of 5: CMR score = (z-WC + z-log-triglycerides + z-SBP + z-glucose − z-HDL-C)/
Concurrent zBMI was the zBMI measured on the same visit as the CMR score. Concurrent zBMI, which was the last BMI measurement, was included in the estimation of the trajectories, since using all available BMI measures leads to a more precise estimate of the trajectories, and current weight status and growth trajectories cannot be separated conceptually since trajectories are derived from repeated measures of body size. All potential confounders were determined a-priori from the literature, and included child age, sex, family income, birthweight, breastfeeding duration, maternal education, maternal ethnicity, smoking during pregnancy, gestational age, maternal BMI, hypertension in pregnancy and gestational diabetes, family history of cardiometabolic diseases, and fasting time. 16
Statistical Analysis
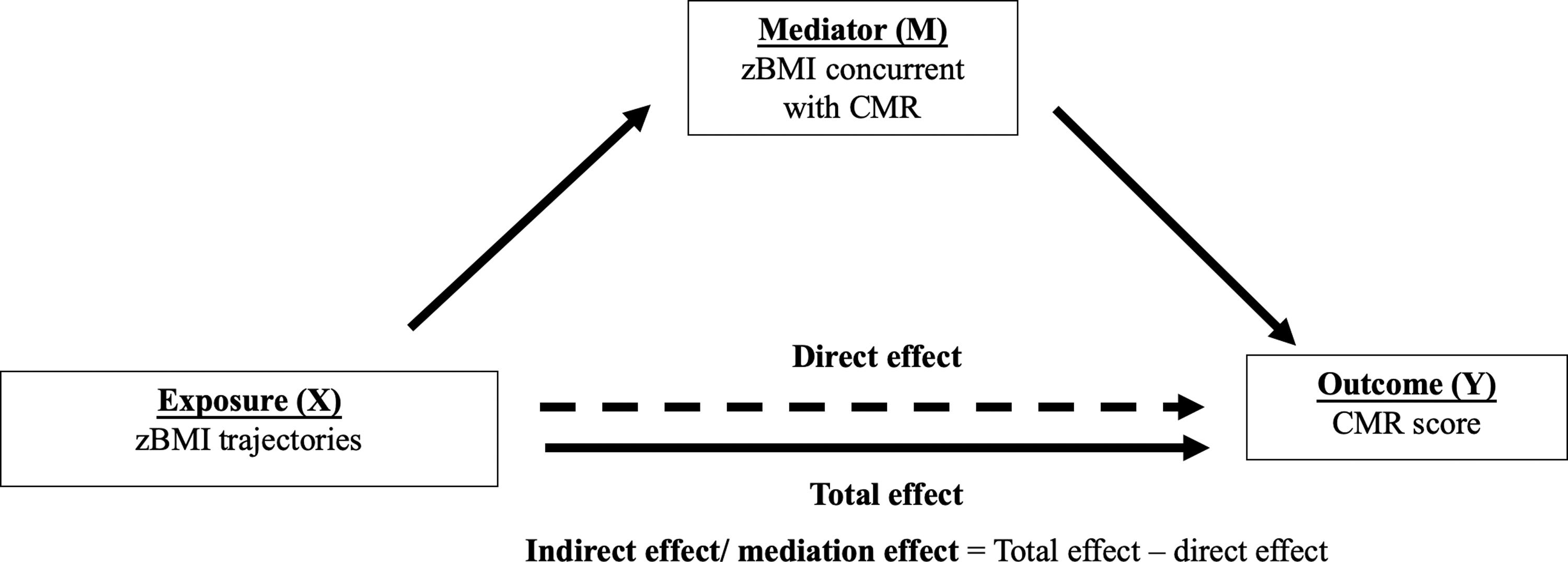
Our approach to mediation analysis assumes that control has been made for exposure-outcome confounding, mediator-outcome confounding and exposure-mediator confounding, and that none of the mediator-outcome confounders are affected by the exposure. 34 We used the difference in coefficients approach to test mediation. 35 This approach compared the association between the exposure (zBMI trajectories) and the outcome (CMR score) before and after accounting for the mediator (concurrent zBMI). The conceptual model is shown in Figure 1. The total effect represents the association between the exposure and the outcome before accounting for the mediator. The direct effect represents the association after accounting for the mediator. The indirect/mediation effect was estimated as the difference between the estimated total effect and direct effect.
Linear regression was used for the mediation analysis comparing each trajectory with the reference trajectory in the same model. We also tested for exposure-mediator interactions. 34 We used a combination of bootstrap resampling and imputation, performing 1000 bootstrap and imputation pairs for each analysis to estimate the 95% confidence intervals (CIs) and p-values for the three models used in the mediation analysis. 36 Imputations were performed using the mice package in R. 37 Missingness for each covariate was under 15%. 16 All p-values were two-tailed. R version 3.5.0 was used for all analyses (https://www.R-project.org). 38
Results
One thousand one hundred sixty-five children were included in this study. Participant characteristics stratified by the four zBMI trajectories are shown in Table 1. Children in the rapid accelerating trajectory (trajectory 4) had the highest CMR score (1.30 ± 0.90) and concurrent zBMI (3.50 ± 0.94), which is 1.30 standard deviations and 3.50 standard deviations above the mean, respectively. Children in the stable low trajectory (trajectory 3) had the lowest CMR score (−0.07 ± 1.09) and concurrent zBMI (0.05 ± 0.82).
Participant Characteristics
Reference trajectory.
Measured at various time points between 36 and 60 months of age.
CMR, cardiometabolic risk; SD, standard deviation; zBMI, standardized BMI.
Mediation analysis results are shown in Table 2. On average, compared to being in the reference trajectory, the CMR score among individuals in the catch-up trajectory (trajectory 1) was associated with an increased CMR score of 0.42 units, 0.28 of which was mediated through concurrent zBMI (95% CI 0.17 to 0.41, p = 0.001); being in the stable high trajectory (trajectory 2) was associated with an increased CMR score of 0.23 units, 0.24 of which was mediated through concurrent zBMI (95% CI 0.18 to 0.31, p < 0.001). Similarly, compared to being in the reference trajectory, being in the rapid accelerating trajectory (trajectory 4) was associated with an increased CMR score of 1.43 units, 1.18 of which was through concurrent zBMI (95% CI 0.89 to 1.50, p < 0.001). There was strong evidence that the effect of zBMI trajectories on later CMR was mainly indirect via concurrent BMI, providing little evidence for a direct effect of the zBMI trajectories on CMR. We did not calculate the proportion of the mediation effect, as this measure is not meaningful to interpret when the direct effect and the mediation effect operate in the opposite direction and the proportion of mediation is larger than 100%, 34 as was the case for trajectory 2. There was no evidence of exposure-mediator interactions (p = 0.79; 0.61; 0.89). We have also examined the multicollinearity between zBMI trajectories and concurrent zBMI. The variance inflation factors were checked and all were below 2.0, therefore multicollinearity was unlikely to be an issue in the final models.
Mediation Analysis Results Using Linear Regression
Trajectory 3 (stable low trajectory) is the reference. Bold values indicate significance p < 0.05.
Adjusted for child age, sex, family income, birthweight, breastfeeding duration, maternal education, maternal ethnicity, smoking during pregnancy, gestational age, maternal BMI, hypertension in pregnancy and gestational diabetes, family history of cardiometabolic diseases, and fasting time.
CI, confidence interval.
Discussion
In this study, we confirmed that there is strong evidence that concurrent zBMI is a mediator, mediating the association between growth trajectories and CMR in young children. To our knowledge this is the first study that quantified the role of concurrent zBMI in the relationship between BMI trajectories and CMR in young children using mediation analysis.
Strengths of the present study were the relatively large sample size of young children with repeated BMI measurements and blood biomarkers, allowing for a more accurate trajectory estimation and measurements on glucose, triglycerides (TG), HDL-C, and non-HDL-C. Further, each subject's weight and length/height were measured by a trained research assistant, which helped eliminate self-reporting error and response bias.
This study has several limitations. There were few children in the rapidly accelerating trajectory, which reduced the statistical power for detecting differences with other trajectories and detecting interactions. However, the rapidly accelerating trajectory group persists in both the 3-trajectory, 4-trajectory, and 5-trajectory models, 16 therefore, this trajectory was retained as a unique group, despite its small sample size. 16 Furthermore, although we believe that we have adequately adjusted for confounders between the exposure, mediator, and outcome, unobserved residual confounding still might have occurred. Finally, we did not adjust for clustering within clinics, and we had trained research assistants and standardized methods and equipment across all clinics.
Our results are in line with the results of a mediation analysis conducted by Slining et al., 27 who found no direct effects of infant weight velocity on adult insulin resistance in a Filipino cohort, but significant indirect effects mediated through adult BMI and WC. 27 However, the absence of direct effect of growth pattern on later CMR outcomes does not mean that growth pattern has no contribution to CMR outcomes. Since the current body size is essentially the last measure of multiple body size measures forming the trajectory, growth and current body size cannot be separated conceptually. 26 Both growth patterns in early childhood, as well as BMI have important influence on chronic disease risk in young children. It is important for clinicians to consider both growth pattern and current weight status when evaluating the risk of cardiometabolic diseases in young children. Further analysis is needed to evaluate the relative importance of the contribution of these two factors.
Previous growth studies included concurrent BMI as a confounder in their models, resulting in an attenuation or disappearance of effect of growth on CMR.7,15,17–20,22,25 To understand the true total effect of growth patterns on CMR, concurrent BMI should not be included in the model as a potential confounder. According to Schisterman et al., controlling for an intermediate variable on a causal pathway from exposure to outcome may introduce overadjustment bias. 39 If the researcher is interested in the total effect but still adjusts for concurrent BMI in the model, then they may introduce overadjustment bias, and ultimately inadvertently estimate the direct effect, instead of the total effect of growth on later cardiometabolic health outcomes, resulting in an underestimation of the total effect. However, it is not incorrect to adjust for concurrent BMI in the model in all circumstances, since the choice of method depends on the researchers' questions of interest. 40 If the research question is about the direct effect rather than the total effect of growth on later CMR, concurrent BMI should be included in the model. Most of the studies mentioned above were not explicit about whether their goal was to examine the total effect or the direct effect of growth on CMR outcomes7,15,18–20,22,25; only one study mentioned that the total effects were estimated in its method section. 17 Given the significance of early prevention of obesity and chronic diseases in children, it is important for future obesity and growth researchers to present a clear study hypothesis and to choose the most appropriate method based on the hypothesis to understand either the total or direct effect of growth patterns on chronic disease risk in children. Further growth studies are needed to replicate our findings, with CMR as well as other child health outcomes.
Footnotes
Acknowledgments
We thank all the participating families for their time and involvement in TARGet Kids! and are grateful to all practitioners who are currently involved in the TARGet Kids! practice-based research network. Members of the TARGet Kids! Collaboration: Co-Leads: Catherine S. Birken, MD, and Jonathon L. Maguire, MD. Advisory Committee: Ronald Cohn, MD; Eddy Lau, MD; Andreas Laupacis, MD; Patricia C. Parkin, MD; Michael Salter, MD; and Shannon Weir-Seeley, MSc. Science Review and Management Committees: Laura N. Anderson, PhD; Cornelia M. Borkhoff, PhD; Charles Keown-Stoneman, PhD; Christine Kowal, MSc; and Dalah Mason, MPH. Site Investigators: Murtala Abdurrahman, MD; Kelly Anderson, MD; Gordon Arbess, MD; Jillian Baker, MD; Tony Barozzino, MD; Sylvie Bergeron, MD; Gary Bloch, MD; Joey Bonifacio, MD; Ashna Bowry, MD; Caroline Calpin, MD; Douglas Campbell, MD; Sohail Cheema, MD; Elaine Cheng, MD; Brian Chisamore, MD; Evelyn Constantin, MD; Karoon Danayan, MD; Paul Das, MD; Mary Beth Derocher, MD; Anh Do, MD; Kathleen Doukas, MD; Anne Egger, BScN; Allison Farber, MD; Amy Freedman, MD; Sloane Freeman, MD; Sharon Gazeley, MD; Charlie Guiang, MD; Dan Ha, MD; Curtis Handford, MD; Laura Hanson, MD; Leah Harrington, MD; Sheila Jacobson, MD; Lukasz Jagiello, MD; Gwen Jansz, MD; Paul Kadar, MD; Tara Kiran, MD; Holly Knowles, MD; Bruce Kwok, MD; Sheila Lakhoo, MD; Margarita Lam-Antoniades, MD; Eddy Lau, MD; Denis Leduc, MD; Fok-Han Leung, MD; Alan Li, MD; Patricia Li, MD; Jessica Malach, MD; Roy Male, MD; Aleks Meret, MD; Elise Mok, MD; Rosemary Moodie, MD; Katherine Nash, MD; Sharon Naymark, MD; James Owen, MD; Michael Peer, MD; Marty Perlmutar, MD; Navindra Persaud, MD; Andrew Pinto, MD; Michelle Porepa, MD; Vikky Qi, MD; Noor Ramji, MD; Danyaal Raza, MD; Alana Rosenthal, MD; Katherine Rouleau, MD; Caroline Ruderman, MD; Janet Saunderson, MD; Vanna Schiralli, MD; Michael Sgro, MD; Hafiz Shuja, MD; Susan Shepherd, MD; Barbara Smiltnieks, MD; Cinntha Srikanthan, MD; Carolyn Taylor, MD; Stephen Treherne, MD; Suzanne Turner, MD; Fatima Uddin, MD; Meta van den Heuvel, MD; TheaWeisdorf, MD; PeterWong, MD; John Yaremko, MD; Ethel Ying, MD; Elizabeth Young, MD; and Michael Zajdman, MD. Research Team: Marivic Bustos, RPN; Pamela Ruth Flores, MD; Mateenah Jaleel, BSc; Tarandeep Malhi, MLT; Ataat Malick, MD; Michelle Mitchell, BA; Martin Ogwuru, MBBS; Frank Ong, MSc; Rejina Rajendran, BE; Sharon Thadani, MLT; Julia Thompson, SSRP; and Laurie Thompson, MLT. Project Team: Mary Aglipay, MSc; Imaan Bayoumi, MD; Sarah Carsley, PhD; Katherine Cost, PhD; Karen Eny, PhD; Laura Kinlin, MD; Jessica Omand, PhD; Shelley Vanderhout, BASc; and Leigh Vanderloo, PhD. Applied Health Research Centre: Christopher Allen, BSc; Bryan Boodhoo, MSc; Peter Juni, MD; Gurpreet Lakhanpal, MSc; Gerald Lebovic, PhD and Audra Stitt, MSc. Mount Sinai Services Laboratory: Rita Kandel, MD, and Michelle Rodrigues, BSc.
Funding Information
This work was supported by the CIHR.
Author Disclosure Statement
Dr. John L. Sievenpiper has received research support from the Canadian Foundation for Innovation, Ontario Research Fund, Province of Ontario Ministry of Research and Innovation and Science, Canadian Institutes of Health Research (CIHR), Diabetes Canada, PSI Foundation, Banting and Best Diabetes Centre (BBDC), American Society for Nutrition (ASN), INC International Nut and Dried Fruit Council Foundation, National Dried Fruit Trade Association, The Tate and Lyle Nutritional Research Fund at the University of Toronto, The Glycemic Control and Cardiovascular Disease in Type 2 Diabetes Fund at the University of Toronto (a fund established by the Alberta Pulse Growers), and the Nutrition Trialists Fund at the University of Toronto (a fund established by an inaugural donation from the Calorie Control Council). He has received in-kind food donations to support a randomized controlled trial from the Almond Board of California, California Walnut Commission, American Peanut Council, Barilla, Unilever, Unico/Primo, Loblaw Companies, Quaker, Kellogg Canada, and WhiteWave Foods. He has received travel support, speaker fees and/or honoraria from Diabetes Canada, Mott's, LLP, Dairy Farmers of Canada, FoodMinds, LLC, International Sweeteners Association, Nestlé, Pulse Canada, Canadian Society for Endocrinology and Metabolism (CSEM), GI Foundation, Abbott, Biofortis, ASN, Northern Ontario School of Medicine, INC Nutrition Research & Education Foundation, European Food Safety Authority (EFSA), and Physicians Committee for Responsible Medicine. He has or has had ad hoc consulting arrangements with Perkins Coie LLP, Tate & Lyle, and Wirtschaftliche Vereinigung Zucker e.V. He is a member of the European Fruit Juice Association Scientific Expert Panel. He is on the Clinical Practice Guidelines Expert Committees of Diabetes Canada, European Association for the Study of Diabetes (EASD), Canadian Cardiovascular Society (CCS), and Obesity Canada. He serves or has served as an unpaid scientific advisor for the Food, Nutrition, and Safety Program (FNSP) and the Technical Committee on Carbohydrates of the International Life Science Institute (ILSI) North America. He is a member of the International Carbohydrate Quality Consortium (ICQC), Executive Board Member of the Diabetes and Nutrition Study Group (DNSG) of the EASD, and Director of the Toronto 3D Knowledge Synthesis and Clinical Trials foundation. His wife is an employee of Sobeys, Inc. These agencies had no role in the design, collection, analyses, or interpretation of the results of this study or in the preparation, review, or approval of the article. Dr. Jonathon L. Maguire received an unrestricted research grant for a completed investigator-initiated study from the Dairy Farmers of Canada (2011–2012) and Ddrops provided nonfinancial support (vitamin D supplements) for an investigator-initiated study on vitamin D and respiratory tract infections (2011–2015). These agencies had no role in the design, collection, analyses, or interpretation of the results of this study or in the preparation, review, or approval of the article. The remaining authors declare that they have no competing financial interests.