
Abstract
Background:
Community coalitions often lead and coordinate “whole-of-community” childhood obesity prevention interventions. A growing body of work suggests that coalition network ties, which facilitate transmission of information and advocacy, may be a key part of how such leadership operates. This study provides an understanding of the structure of coalition networks and how this structure changes over time.
Methods:
We administered semiannual network surveys during a pilot whole-of-community intervention in Somerville, MA (2015–2017). Participants included 16 multisector coalition members and their nominated discussion partners (“first-degree alters”) related to childhood obesity prevention. Coalition and first-degree alter respondents named up to 20 discussion partners and reported ties' interaction frequency and perceived influence. Networks were assessed with visualization, descriptive analysis, and exponential random graph models.
Results:
Total network included 558 stakeholders representing community-based organizations, parents, health care, childcare, universities, among others. Size and membership varied over time. We observed the largest network (n = 256) during intervention planning, and the largest proportion of stakeholders communicating frequently (daily/weekly) about childhood obesity prevention during the peak intervention period. Networks were sparsely interconnected (1%–3% of possible ties observed) and most and least centralized at baseline and follow-up, respectively. Over time, ties were increasingly perceived as influential and siloed within community groups.
Conclusions:
The network's extensive evolving membership may indicate access to a wide range of resources, ideas, and an ability to broadly disseminate intervention messages. The attenuating network hierarchy over time may have supported more equal participation and control over intervention efforts. Future research should assess generalizability of network patterns, network influences on implementation processes, and possible network interventions.
Introduction
Complex public health issues such as childhood obesity require systems-oriented action.1–3 “Whole-of-community” childhood obesity prevention interventions hold promise by synergistically targeting multiple weight-related behaviors at varying levels of influence (e.g., families, organizations, and local policy).4–6 Although whole-of-community interventions may benefit children of all ages, they may be of particular value for young children. Early childhood is a critical life stage for obesity prevention with opportunities to shape developing preferences, habits, and weight trajectories.7,8 Serving this age group also offers opportunities to unite diverse potentially fragmented stakeholders from across settings and sectors to work collectively toward improving child health.
Community coalitions can help achieve collective efforts by involving interorganizational and multisector stakeholders collaborating to affect community and/or individual-level change.9–11 Coalitions have held leadership and coordination roles in several whole-of-community childhood obesity prevention trials, contributing to local capacity building, social change in addressing childhood obesity, and intervention sustainability. 12 The organizational structure of coalition relationships—their networks—is an understudied but potentially key component for intervention success. Network ties may shape the creation of new collaborative activities, transmission of information and advocacy, and access to resources distributed throughout the coalition and community.
Coalition Characteristics and Social Network Analysis
Social network analysis (SNA) offers a framework and toolkit to understand coalition structure.13–15 SNA has been used to study coalitions in several public health prevention contexts16–20 and is an emerging area of investigation in childhood obesity—although to date, studies are limited to retrospective 21 and cross-sectional designs.22,23 Drawing on coalition effectiveness literature and theory,9–11 we briefly describe what is known and unknown about coalition network structure, which may help optimize future efforts.
In a study of substance abuse prevention coalitions, networks with more connections among members (greater density) had lower rates of adopting evidence-based programs—perhaps due to challenges in accessing and mobilizing innovative thinking and resources external to the coalition that would benefit implementation.9,11,17 Others have suggested that less hierarchical coalitions (lower centralization) are able to build members' trust and agency.13,16,24,25 As documented by Bess, coalition network structures evolve throughout interventions. 16 Yet, optimal structures may differ at various intervention stages—for example, a well-connected less hierarchical network during early planning efforts may facilitate information spread.16,19,26
In the context of coalitions engaged in whole-of-community obesity prevention, a retrospective study of two interventions in the United States 27 and Australia 28 revealed similarities in coalition network structures—particularly the tendency for high clustering or cohesion among members. 21 Another study demonstrated that centrally positioned coalition members took “central actions” within the mapped obesity prevention system. 23 To our knowledge, however, no studies to date have prospectively examined changes in a coalition network during a childhood obesity prevention intervention. Understanding these coalition dynamics and how they relate to intervention processes may provide key insights for eventual “network interventions” 29 that aim to change network structure to improve implementation and sustainability.
Coalition effectiveness theory suggests that coalitions are increasingly effective as membership grows and diversifies in represented ideas, interests, and organizations.9,11 This relates to the concept of heterophily, in which coalition members seek relationships with those dissimilar to themselves, or the opposite, homophily, often framed as the tendency to “silo” within organizations and sectors.16,30,31 Prior coalition network studies provide mixed evidence of heterophily and homophily patterns. Similar investigation in obesity prevention interventions may reveal insights about how stakeholders might improve multisector collaboration to achieve goals such as diffusion and sustainability.12,32,33
Building on prior theory and research on coalition network structure and dynamics, this study provides the first empirical prospective examination of a coalition network during the design and implementation of a pilot whole-of-community intervention to prevent early childhood obesity. Over time, we expected to observe increasing network membership, cohesion, tie strength, and likelihood of multisector ties—characteristics that may improve intervention planning, implementation, and sustainability.11,12,33 Our study also provides a framework for future prospective studies of coalition network dynamics in chronic disease prevention.
Methods
Shape Up Under 5
We analyzed social network data from community stakeholders involved in Shape Up Under 5 (SUU5): a pilot whole-of-community early childhood obesity prevention intervention in Somerville, MA (2015–2017). Somerville is a small urban city (4.1 mi 2 = 6.6 km2) in the greater Boston area with ∼81,000 residents in 2019, of which ∼4% were under age 5 years. 34 The 2018 population included 76% White, 11% Hispanic or Latino, 10% Asian, and 7% Black or African American residents. 34 In 2014–2018, 24.0% of residents were foreign born. 34
With Shape Up Somerville and other community-wide health initiatives, Somerville has received international recognition for “establishing comprehensive, multi-sector partnerships to achieve systems, environmental, and policy change” with the goal “that everyone who lives, works, plays and eats in Somerville has access to healthful food options and active living opportunities.”27,35–37
SUU5 study design and methods are described elsewhere.38,39 In brief, SUU5 investigated the attributes and processes of a newly formed coalition (the “Committee”38,39) that was convened for the study and comprised largely director/manager-level stakeholders from diverse organizations serving young children and their families.
As reported previously, Committee recruitment was informed by key informant interviews, community knowledge and partnerships, recommendations from obesity content experts, and an agent-based model of the 2003–2005 Shape Up Somerville intervention.38,39 Stakeholders also made referrals throughout the interview and recruitment process. Sixteen of 29 contacted stakeholders agreed to join the Committee (n = 9 no response and n = 4 declined). Reasons for declined participation included involvement in a separate ongoing research study, health condition, time barrier, and department already represented.
As part of SUU5, the Committee met approximately monthly and led the design and community-wide dissemination of an evidence-based campaign (“Small Steps: Eat, Play, Sleep”) toward the Committee's prioritized goals of “healthy family culture,” “intersystem communication,” “community participation,” among others. 39 In a mixed methods evaluation, Committee members reported that their participation in SUU5 helped draw connections across multiple community issues (e.g., obesity and upstream social determinants of health), facilitated awareness of other organizations' work and the challenges they face, and reduced barriers to collaborating across sectors. 39
Table 1 includes a timeline and description of SUU5 intervention phases—which we (post hoc) refer to as Convening, Priority Setting, Creating, Implementing, and Planning for Sustainability—and corresponding social network measurement waves (W1–W5; described hereunder) to contextualize findings (e.g., Convening phase at W1). Readers are referred elsewhere for greater detail of the Committee's work together during SUU5. 39
Shape Up Under 5 Intervention Timeline, Somerville, MA, 2015–2017
Intervention phases were named to be familiar to community-engaged researchers and practitioners. Campaign materials (“Small Steps: Eat, Play, Sleep”) are publicly available at http://somervillehub.org/downloads in English, Spanish, Portuguese, and Haitian-Creole.
Subgroups of Committee members met periodically with the research team to advance intervention objectives.
Additional data collection points among Committee members only are denoted with an asterisk. Committee data collected at baseline in Fall 2015 (W1) and at 24 months “follow-up” in Fall 2017 (W5) were kept as is. Committee data collected in Winter 2016 (W2*), Summer 2016 (W3*), and Winter 2017 (W4*) were aggregated with W2, W3, and W4, respectively, to create an analytic data set with five waves.
SUU5, Shape Up Under 5.
Social Network Data Collection: Sampling and Participants
Overview and definitions
We employed a snowball sampling approach initiating from Committee members with the goal to observe community-wide connections related to early childhood obesity prevention. 15 The network included Committee members, nominees of Committee members (“first-degree alters”), and nominees of first-degree alters (“second-degree alters”)—collectively named “stakeholders” when describing all network members. Hereunder we further distinguish between “respondents” and “nonrespondents” of the network survey administered among Committee members and first-degree alters (second-degree alters were not invited to participate).
Committee survey
Committee members completed eight web-based network surveys, nominating up to 20 individuals each survey (described in Measures).21,40 The first seven surveys were administered quarterly during the 18-month intervention period. The eighth survey was administered at 24 months (“follow-up”).
First-degree alter survey
Nominees of Committee members were subsequently recruited to participate in up to five network surveys, also nominating up to 20 individuals (described hereunder) at baseline, 6, 12, 18, and/or 24 months. Nominators' identity(ies) were not disclosed. The first-degree alter survey was administered less frequently than the Committee survey to minimize survey fatigue and encourage repeat responses.
Survey respondents reported nominees' community affiliation from a drop-down list (e.g., health care, center-based childcare; Table 2) and were also asked to provide nominees' organization/department and title. Respondents did not report nominees' contact information or characteristics (e.g., gender) to minimize respondent burden and potential discomfort of reporting nominees' personal information. Using the data provided, successful recruitment of first-degree alters was contingent on the research team's ability to obtain accurate email addresses through online searches (e.g., organization websites) and existing contacts. Supplementary Figure S1 shows survey distribution, exclusions, and response rates among first-degree alters.
Definitions of Community Affiliations, Shape Up Under 5 Early Childhood Obesity Prevention Network
SUU5, Shape Up Under 5; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children. Except for the “other” category, community affiliations are listed in descending order by representation in the overall discussion network (Fig. 1).
The Tufts University Institutional Review Board approved all study procedures. Committee members provided written informed consent and received a stipend. First-degree alters provided consent electronically and were offered a $20 gift card per survey.
Measures
Network structure
Survey respondents were asked to “provide the names of people with whom you discuss issues related to early childhood obesity in Somerville” with up to 20 nominations in an effort to capture broad community connections.15,21,40 We refer to these nominations as “discussion ties” and they are the foundation of the overall network structure. To facilitate name generation, survey respondents were provided a list of community affiliations. Committee members were also prompted with a list of nominees from their prior survey response and were instructed to renominate any current discussion partners.
Tie strength
Survey respondents characterized the strength of each relationship (“tie”) by two qualities common in the SNA literature and hypothesized to support whole-of-community childhood obesity prevention efforts15,21: interaction frequency about childhood obesity prevention (1 = yearly; 2 = quarterly; 3 = monthly; 4 = weekly; 5 = daily) and perceived influence in shaping one's understanding of childhood obesity prevention efforts (1 = not influential to 5 = very influential).
Stakeholder characteristics
Survey respondents reported their age, gender, highest education level, years of relevant work experience, and community affiliation. For nonrespondents, nominator(s) reported their community affiliation as already described. When different affiliations were reported for the same nonrespondent, we used the most frequently assigned affiliation. Stakeholders in the “other” category (n = 66) were recategorized when possible using the second-most-frequently assigned affiliation or descriptive information collected to facilitate recruitment (e.g., organization/department; data not otherwise used in analyses).
Data Preparation and Analysis
Data were cleaned to match names of stakeholders nominated multiple times but with different spellings. To analyze Committee and first-degree alter data congruently, we reduced the Committee data set from eight to five survey waves to align with the timing and frequency of the first-degree alter survey (Table 1 and Supplementary Appendix).
We treated ties as undirected (visually, a line without arrowheads)15,31,41 and retained all ties and stakeholders (survey respondents and nonrespondents) in analyses as our best approximation of Somerville's “true” network structure related to childhood obesity prevention. 15 Observed stakeholders and ties emerged from three scenarios: (1) stakeholders A and B both responded to the survey and nominated each other (counts as one tie); (2) A and B responded, but A nominated B or B nominated A; (3) only A or B responded and nominated the other. The Supplementary Appendix includes additional data preparation detail.
Using statnet 42 and igraph 43 packages implemented in RStudio (v1.2.5019), we used descriptive network statistics, visualization, and statistical network models to examine networks over time. Analyses focused on the overall discussion network (“discussion ties”) and two subsets: “frequent ties” (weekly or daily interaction) and “influential ties” (4 = influential or 5 = very influential).
For each wave and tie type (discussion, frequent, and influential), we described network size, number of ties, Jaccard index, density, centralization, and mean ± standard deviation (SD) interaction frequency and perceived influence. The Jaccard index represents network change: the proportion of ties maintained across pairs of successive waves, compared with total ties created, maintained and dissolved. 44 Density is the proportion of observed versus possible ties (all pairs of stakeholders) and typically decreases with increasing network size. 13 Centralization describes variability in stakeholders' centrality—higher values indicate more hierarchical “top-down” network structures. 13 We calculated two forms of centralization: degree centralization based on stakeholders' connections and betweenness centralization based on stakeholders' positions—the latter often interpreted as the extent of “gatekeeping” abilities for communication and information flows.
Lastly, we fit exponential random graph models45,46 to examine community affiliation homophily: the tendency for stakeholders in the same group to have ties with each other as an indication of siloing.30,47 We expected a negative homophily effect or heterophily (mixing) across affiliations. Models also controlled for parameters that may contribute to network structure16,46: Committee membership (extent that Committee members are more “active” in the network vs. nonmembers), Committee homophily (tendency for Committee members to have ties with each other), degree (tendency for stakeholders with more connections to have ties with others), and transitivity (tendency for two connected stakeholders to have shared partners in groups of three, indicating local clustering or cohesion).
Separate models were fit for discussion, frequent, and influential ties at each wave to identify potentially common or distinct patterns. We modeled networks in serial cross sections, due to varying sample sizes and network membership over time that prove challenging for SNA longitudinal models. 48 Analytic strategies to include stakeholders present across all waves (9%), most waves (23%), or any two consecutive (35%) waves 49 would omit most observations and obscure community structure. Models have a binary dependent variable (two stakeholders having a tie or not) and estimates are presented as log odds with corresponding standard errors. Estimates >0 indicate increased odds of having a tie based on a given network property, whereas estimates <0 indicate decreased odds.
We assessed model goodness-of-fit using standard procedures, in which observed network properties were compared with that of 100 simulated model runs (Supplementary Appendix).42,50
Results
The cumulative survey response rate was 98.4% among Committee members and 39.4% among first-degree alters (Supplementary Fig. S1). Respondents nominated a median of 5 (interquartile range: 3–9) individuals per survey; 3.4% of respondents nominated the maximum 20 individuals. Committee membership was steady throughout SUU5 (n = 16), except one member moved before W5.
Most Committee members (87.5%) and first-degree alter survey respondents (85.2%) were female and had a graduate degree (75.0% and 62.5%, respectively). At baseline, on average (±SD), Committee members were 50 ± 13 years old with 20 ± 13 years of work experience. First-degree alter survey respondents were younger, on average, than the Committee members (43 ± 13 years) and had fewer years of work experience (14 ± 11 years)—likely reflecting the intentional recruitment of Committee members in director/manager-level positions.
Network Characteristics
Throughout SUU5, the early childhood obesity prevention network included 558 unique stakeholders (n = 16 Committee members; n = 201 first-degree alters; n = 341 second-degree alters) representing community-based organizations (16.8%), parents (14.0%), health care (13.3%), city (10.9%), public school district (10.9%), early education (10.6%), home-based childcare (6.3%), university (5.0%), center-based childcare (3.9%), Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) (2.5%), and other settings/sectors (5.7%) (Fig. 1).

We observed the largest discussion network at W2 (Priority Setting phase) when the intervention was in its planning stages and gaining momentum (Table 3). Networks were sparsely interconnected with 1%–3% of possible ties observed. Betweenness centralization in the discussion network decreased between W1 and W2 and reached a nadir at W5, suggesting that stakeholders' control over communication and information flows was most evenly distributed at follow-up. The W5 discussion network was also least centralized based on stakeholders' connections (degree centralization), although levels fluctuated over time.
Descriptive Network Statistics by Survey Wave and Tie Type (Discussion, Frequent, Influential), a Shape Up Under 5 Early Childhood Obesity Prevention Network
W1–W5 correspond to the following intervention phases described in Table 1: Convening, Priority Setting, Creating, Implementing, and Follow-up (the Planning for Sustainability phase occurred between W3 and W5).
Discussion ties represent the overall network structure, in which respondents were asked to “provide the names of people with whom you discuss issues related to early childhood obesity in Somerville.” Frequent (daily/weekly interaction) and influential (“influential” or “very influential”) ties are subsets of the discussion ties. Analyses include stakeholders who did and did not respond to the survey.
Number of unique stakeholders in the network at each wave (or in other words, the sample size) including Committee members, first-degree alters, and second-degree alters. Network statistics described in this table (e.g., density) are derived from these network sizes. In a network diagram, network size is represented by the number of nodes.
Number of discussion ties, frequent ties, and influential ties between stakeholders. In a network diagram, ties are represented by lines between nodes.
Proportion of ties maintained across pairs of successive waves, compared with the total number of ties created, maintained, and dissolved. The value presented in the W2 column represents stability from W1 to W2, and so forth.
Proportion of ties observed compared with the total number of possible ties (all pairs of stakeholders) [0, 1].
Normalized variability of stakeholders' degree centrality (number of connections); higher values indicate more hierarchical network structures [0, 1].
Normalized variability in betweenness centrality, or stakeholders' position in communication paths; higher values indicate more hierarchical network structures with a small group of prominent actors that may have greater control over information flows [0, 1].
Mean tie strength is calculated from the 5-point scales for interaction frequency about childhood obesity prevention (1 = yearly, 2 = quarterly, 3 = monthly, 4 = weekly, 5 = daily) and perceived influence in shaping one's understanding of childhood obesity prevention efforts in Somerville (1 = not influential to 5 = very influential).
As shown in color in Figure 2A–C, network membership shifted throughout SUU5, with the largest proportion of stakeholders entering the network for the first time at W2 during the Priority Setting phase. These new stakeholders at W2 are represented by blue nodes and make up 63%, 45%, and 55% of the discussion, frequent, and influential networks, respectively (Supplementary Table S1 includes corresponding counts). W1 stakeholders (orange) were prevalent in later waves and generally had the greatest betweenness centrality scores (larger nodes). Approximately one-third of W5 stakeholders (black) were new to that measurement period.
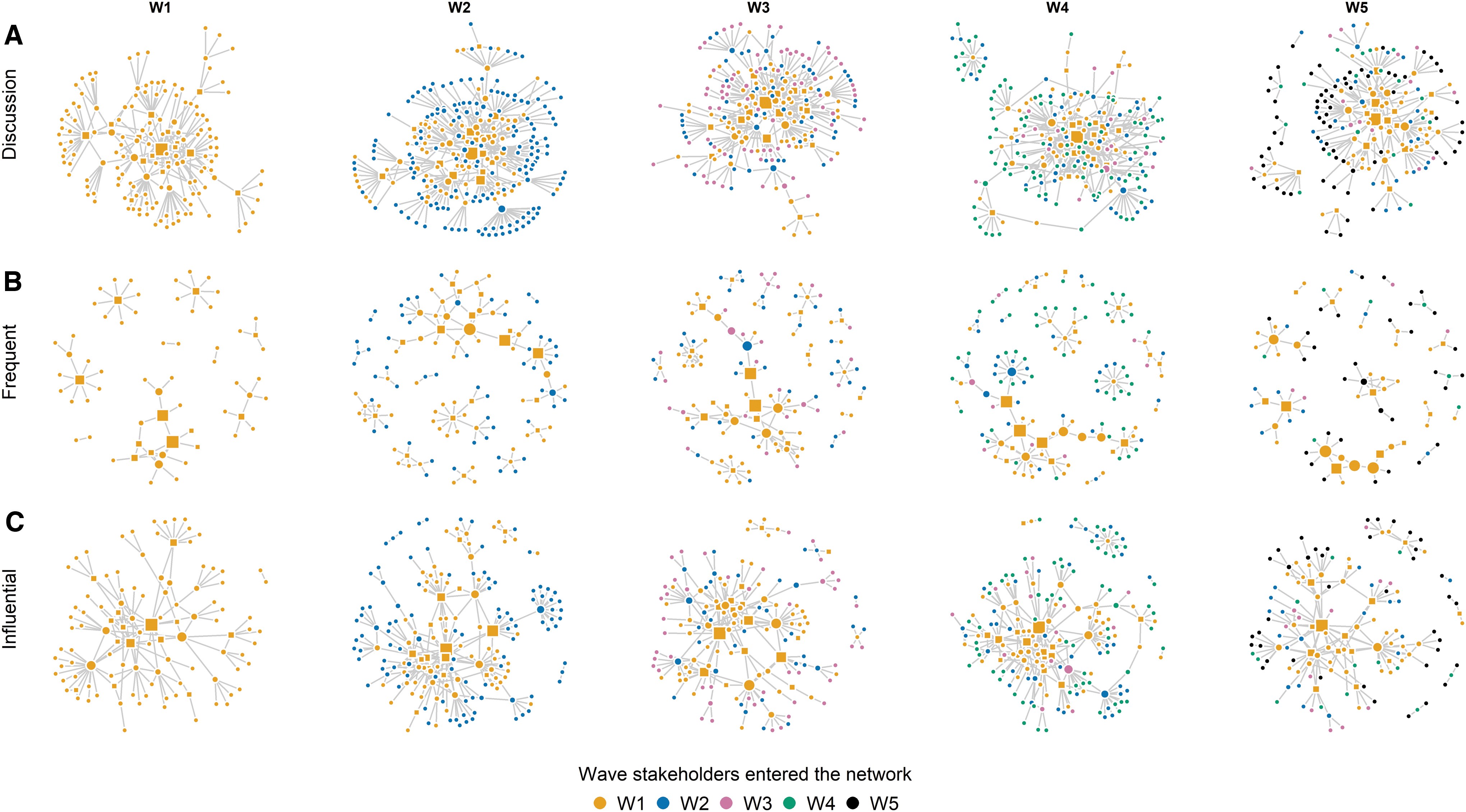
On average, stakeholders interacted about childhood obesity prevention approximately monthly (Table 3). Ties were increasingly perceived as influential, with a 0.4-unit increase in mean rating between W1 and W5. Frequent networks were smaller and more fragmented than influential networks (Fig. 2B, C). The largest proportions of stakeholders interacted frequently between W3 and W4: the peak intervention period (Creating and Implementing phases).
Predictors of Network Ties
We examined the likelihood of ties within versus across community affiliations as an indication of cross-sector collaboration on childhood obesity prevention efforts (Table 4). Controlling for other model parameters, the significant positive community affiliation homophily estimates indicate that stakeholders had greater odds of having ties within versus across community affiliations. The community affiliation homophily effect magnitude was greater for the subset of frequent ties [Table 4(B)] than the subset of influential ties (C) and overall discussion ties (A). Consistent across tie types, the effect magnitude generally increased over time (e.g., among discussion ties, log odds estimates (standard error) of 1.17 (0.13) at W1, 1.37 (0.09) at W3, and 1.62 (0.12) at W5).
Predictors of Network Ties (Discussion, Frequent, Influential) by Survey Wave, Shape Up Under 5 Early Childhood Obesity Prevention Network
Estimates from cross-sectional exponential random graph models. Dependent variables are (A) having a discussion tie between two stakeholders, (B) having a frequent discussion tie (daily/weekly interaction about childhood obesity prevention), and (C) having a discussion tie with a stakeholder perceived as “influential” or “very influential” in shaping one's understanding of childhood obesity prevention efforts in Somerville. Frequent and influential ties are subsets of the discussion ties. Each column represents one model with six predictors (or covariates) of network structure. Estimates >0 indicate increased odds of a tie based on a given network effect, whereas estimates <0 indicate decreased odds. Goodness-of-fit diagnostic plots are available in the Supplementary Appendix. W1–W5 correspond to the following intervention phases described in Table 1: Convening, Priority Setting, Creating, Implementing, and Follow-up (the Planning for Sustainability phase occurred between W3 and W5). *p < 0.05; **p < 0.01; ***p < 0.001.
Number of stakeholders in the network at each wave, or in other words, the sample size.
Tendency for dense network structures. Negative estimates indicate a tendency for sparsely interconnected network structures (<50% of possible ties observed).
Tendency for ties within community affiliations than across affiliations.
Tendency for Committee members to have ties, relative to other stakeholders.
Tendency for Committee members to have ties with each other, relative to other stakeholders.
Tendency for stakeholders with more connections to have ties with others (“geometrically weighted degree” parameter).
Tendency for two connected actors to have shared partners in groups of three (“geometrically weighted edgewise shared partner” parameter). Models additionally controlling for dyadwise shared partners had poor fit and were not included in final models.
We also examined the role of Committee membership in network structures. All else equal, the significant positive estimates indicate that Committee members were more “active” in the network than nonmembers, with two exceptions—in W3 and W5, Committee members were not more or less likely than nonmembers to communicate frequently about childhood obesity prevention. The significant negative Committee homophily estimates between W1 and W3 among frequent ties [W1: −0.84 (0.32); W2 − 1.06 (0.33); W3: −1.23 (0.43)] indicate that Committee members frequently interacted with nonmembers during the Convening, Priority Setting, and Creating phases.
Across most waves and tie types, with other parameters held constant, we observed significant tendencies for stakeholders with more connections to have ties with others (degree parameter). The increasing transitivity estimates between W1 and W3 in the discussion network [W1: 0.92 (0.11); W3: 1.39 (0.10)] and frequent network [W1: 0.44 (0.25); W3: 1.02 (0.14)] indicate an increasing tendency for local clustering (groups of three) during Convening, Priority Setting, and Creating phases.
Model fit
The Supplementary Appendix includes goodness-of-fit diagnostic plots. Across waves and tie types, observed network statistics did not differ significantly from that of 100 simulated networks, suggesting good fit overall. The observed proportion of stakeholders with one tie exceeded expected values. This reflects the study design—not all nominated stakeholders had the chance to nominate others.
Discussion
We examined the evolution of a coalition network during a pilot whole-of-community intervention aiming to prevent early childhood obesity. As expected, the network grew as the intervention was in its planning stages and gaining momentum. During Convening, Priority Setting, and Creating phases, we observed increasing tendencies for local clustering or cohesiveness among discussion ties and the subset of frequent ties communicating at least weekly about childhood obesity prevention. During these phases, Committee members frequently interacted with nonmembers, perhaps indicating the spread of intervention information to their colleagues and professional contacts within their network. The large proportion of frequent ties during the Creating and Implementing phases likely represent core workforces, including Committee members and other stakeholders, that drove the intervention forward.
Between W4 and W5, the decreasing discussion network size and increasing fragmentation (Fig. 2A) likely reflect the network returning to its “natural” state postintervention when the Committee did not meet formally. However, at W5, we observed some evidence of sustained and potentially beneficial network characteristics: continued introduction of new stakeholders engaged with the issue; on average, maintained monthly interaction frequency about childhood obesity prevention (same frequency of Committee meetings); and on average, stakeholders' perceptions of ties as influential. Since stakeholders increasingly tended to silo within community affiliations, these “stronger” W5 ties may have supported sustained intervention efforts within stakeholders' organizations, settings, and sectors.
Stakeholders at baseline represented a substantial proportion of later network membership and were among the most powerful gatekeepers throughout SUU5 as evidenced by their higher betweenness centrality (larger orange nodes; Fig. 2A–C). Although confirmation is needed in other studies, we expect that membership of early stage networks captures a certain threshold of influential stakeholders who are likely to have sustained intervention engagement. Baseline network assessments may offer utility as a diagnostic to identify (and subsequently “activate”) dedicated prominent stakeholders.51,52 Given that the Committee mostly included directors and managers, future research should examine these patterns by organizational position and work experience.
Multisector and interorganizational collaboration is a pervasive goal of many public health systems and networks.18,30,53 Similarly, the success of whole-of-community childhood obesity prevention interventions relies on stakeholders' abilities to coordinate and collaborate across sectors.12,32,33 Throughout SUU5, however, stakeholders tended to silo within community affiliations. McGlashan and colleagues observed a similar homophily effect in a community-based childhood obesity prevention network in Australia. 23
Outside of obesity prevention, other coalition network studies have found evidence of collaboration patterns within and across similar types of organizations or agencies.16,31 In SUU5, the propensity to have within-affiliation ties likely facilitated campaign dissemination to stakeholders' own colleagues and professional contacts, but perhaps would inhibit collaboration and resource sharing across diverse community groups.
Future studies should investigate how various levels of homophily—such as few strategic cross-sector ties versus extensive mixing—affect stakeholders' behaviors and abilities to implement systems-wide changes. This could include examination of specific sector-to-sector patterns. 30 For example, we might expect that health care-to-WIC ties are important for integrating cohesive messaging about healthy eating and beverage consumption, whereas ties across early education and childcare settings might facilitate kindergarten readiness.
The emerging concept of “network interventions,” 29 most readily adopted in studying health behaviors, 54 offers a useful framework for achieving cross-sector communication and collaboration goals. One way of doing this is through the purposeful “alteration” 29 of network structures. Although SUU5 did not study network interventions, our analytical approach would facilitate such efforts in the future by using relational data to carefully demarcate network boundaries and observe changes after an intervention.
Networks at baseline and follow-up were similar in size and density, yet communication patterns differed. The higher centralization at baseline may reflect existing leadership structures in the community—perhaps benefiting early planning efforts with efficient top-down sharing of information and resources. 55 The shift toward a less hierarchical network (based on betweenness centralization) may indicate greater equality in stakeholders' gatekeeping abilities to disseminate intervention-related information across segments of the network, potentially contributing to greater intervention ownership, shared decision making, and sustainability.24,25
During SUU5, 16 dedicated community leaders worked together to address early childhood obesity, yet overall, we observed 558 stakeholders engaging with the issue. This large and evolving constituency represents the network's ability to broadly disseminate intervention messages and access diverse resources and ideas. Somerville has a strong history of whole-of-community health promotion efforts, multisector partnership development, and interagency coalition building.27,35–37 Similar prospective research is underway in other communities as a step toward drawing generalizations across geographies, population groups, and coalitions with varying histories (e.g., new vs. established), meeting frequencies, and activities.
We observed extensive shifts in network membership, with 34%–63% new stakeholders each wave. The paucity of longitudinal coalition network studies makes it difficult to assess generalizability of this finding, requiring further research. A 5-year study of a youth violence prevention coalition found membership to vary slightly each year (84 ± 6 organizations). 16 Consistent with SUU5, the greatest growth in the violence prevention coalition occurred early in the intervention. 16
Study Limitations
Several limitations must be considered. First, the unknown “network boundary” of community-wide stakeholders involved in childhood obesity prevention efforts precluded use of a roster-based name generator. 15 We relied instead on a Committee-initiated snowball sampling approach, yielding a ∼40% response rate among first-degree alters (similar to other web-based surveys 56 ). Nonresponse and lack of sampling among more distal stakeholders (≥2 degrees removed from the Committee) likely decreased observed connectivity.
Second, first-degree alter survey response was weakest among stakeholders interacting with children the most—namely, parents and childcare providers (Fig. 1). Future whole-of-community research should focus on improving recruitment of these critical harder-to-reach groups, particularly if additional studies yield similar nonresponse patterns. Alternative approaches beyond web/email-based surveys may be required.
Third, interpretation of observed network changes must consider the potentially intervening role of the research study. Although we did not utilize network data to inform intervention efforts, several study activities could be seen as “network interventions” 29 —particularly the Committee convening and meetings offering opportunities for tie formation. 39 In addition, some changes may reflect organizational turnover.
Lastly, we did not examine associations between stakeholders' network characteristics and their implementation behaviors, 17 which in future research could help optimize networks embedded in whole-of-community obesity prevention interventions. Toward this goal, McGlashan and colleagues used multilevel models to examine how stakeholder networks relate to intervention actions mapped onto a qualitative system dynamics diagram. 23 Integrating complex systems tools may generate helpful implementation insights—for example, that central stakeholders work on “central activities” highly connected to the intervention system. 23
Conclusions
Whole-of-community interventions hold promise in preventing childhood obesity,4–6 yet the backbone of such efforts—stakeholder networks—is understudied. Throughout SUU5, we observed several network characteristics that may support coalition effectiveness in achieving its goals toward community-wide systems change. The network's extensive evolving membership may indicate access to a variety of resources, ideas, and an ability to broadly disseminate intervention messages. The attenuating network hierarchy over time may have supported more equal participation and control over intervention efforts. Future research should assess the generalizability of observed network patterns, associations with intervention implementation, and if and how to intervene on coalition networks—for example, by promoting multisector collaboration—to optimize obesity prevention approaches.
Footnotes
Acknowledgments
We are grateful to the study participants who generously contributed to this research. We also thank the Childhood Obesity Modeling for Prevention and Community Transformation (COMPACT) team for their contributions to the SUU5 study.
Funding Information
This study was supported by a grant from the National Institutes of Health, “Systems Science to Guide Whole of Community Childhood Obesity Interventions” (R01HL115485 to C.D.E. and R.A.H.) and the New Balance Foundation (A.R.K. doctoral fellowship). The funders were not involved in the study conception, research design, data collection, analysis, or article writing nor in the decision to submit the article for publication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.