
Abstract
Background:
The purpose of this study was to evaluate the effectiveness of a 10-week blended family-based childhood obesity management program, relative to a wait-list control, in improving child body mass index (BMI) z-scores, child lifestyle behaviors, parental support for healthy eating and physical activity, and self-regulation for healthy eating and physical activity support.
Methods:
This study was registered as a randomized wait-listed controlled trial; however, due to low recruitment and program delivery logistics, this study transitioned into a quasi-experimental design. Families with children 8–12 years of age with a BMI ≥85th percentile for age and sex were recruited (October 2018 to March 2019) in British Columbia, Canada. The intervention provided families 10 weeks of in-person and online support on improving lifestyle behaviors.
Results:
Children's BMI z-scores were not significantly changed. Intervention group significantly improved their days of moderate-to-vigorous physical activity relative to control (0.75 ± 1.5; p < 0.01; ηp2 = 0.15); however, child dietary behaviors were not significantly changed. Relative to control, intervention group showed significant improvements in parental support for healthy eating (0.13 ± 0.36; p < 0.05; ηp2 = 0.06) and physical activity (1.0 ± 1.6; p < 0.05; ηp2 = 0.09) and self-regulation for healthy eating (2.0 ± 3.5; p < 0.01; ηp2 = 0.11) and physical activity support (2.0 ± 3.2; p < 0.05; ηp2 = 0.28).
Conclusions:
Preliminary evidence showed that the intervention was not effective in improving child BMI z-scores, but it was effective in promoting children's physical activity and parents' support behaviors. A longer study period may be required to change BMI z-scores.
Clinical Trial Registration number: NCT03643341.
Introduction
Childhood obesity remains one of the most common pediatric health issues in Canada. Approximately one-third of Canadian children and over one-fourth of children in British Columbia (BC) are either overweight or obese.1,2 Concerns about the long-term negative health and economic outcomes associated with childhood obesity have prompted public health and policy support for the development and testing of interventions for both childhood obesity prevention and management. 3
Family-based weight management interventions have become a primary approach for achieving weight management among children and adolescents.4–6 The premise of family-based interventions involves removing the focus from the child with overweight or obesity, and instead encouraging the whole family to make lifestyle behavior changes. Interventions that engage with the entire family are critical for improving a child's behaviors because family-level attitudes and behaviors related to eating and physical activity play a large role in shaping a child's lifestyle behaviors and health status. 7 However, in-person family-focused childhood weight management interventions have limited flexibility, and scalability.8,9 Recent studies have shown that web-based interventions can address these existing delivery challenges facing family-based childhood obesity management programs.3,4,10 However, participants enrolled in a stand-alone Internet-based intervention may not feel as supported as an in-person intervention. Thus, a blended family-based intervention approach incorporating face-to-face and web-based components may improve program reach, decrease volunteer and staff time, and provide flexibility for families. 3 Currently, no study has evaluated the efficacy of blended family-based interventions addressing childhood obesity delivered in a community-based setting. 1 Thus, it is critical to evaluate this approach in a “real-world” setting.
This study evaluated the effectiveness of a 10-week, Early Intervention Program (EIP) in managing obesity in children 8–12 years of age. The EIP development was guided theoretically by the multiprocess action control (M-PAC) framework, 11 a unique meta-theoretical approach that addresses the “intention to behavior” gap. The M-PAC framework consists of operational constructs portraying the process of behavior change from intention formation to action control (i.e., translating intention into behavior), adoption, and maintenance. Particularly, these constructs align with phases of behavioral initiation and continuation throughout the framework and correspond with behavior change techniques (BCTs). 12 Intervention activities were designed to support children and parents in learning behavioral change skills that will enable them to improve their health-related lifestyle behaviors.
The study objective was to evaluate the effectiveness of EIP relative to a wait-listed control. The primary outcome was changes in children's body mass index (BMI) z-score. Secondary outcomes included changes in children's lifestyle behaviors (e.g., dietary, physical activity, sedentary, and screen time), changes in parental support for healthy eating and physical activity, and self-regulation for healthy eating and physical activity support. We hypothesized that EIP would be more effective relative to the control in improving the primary and secondary outcomes.
Methods
Study Design
This 10-week randomized wait-listed control study took place in B.C., Canada, from October 2018 to March 2019. The initial study design was based on a 2:1 randomization, anticipating a 20% dropout. The 2:1 allocation was intended to assist in enrolling the required number of participants to run the program at each site; however, in the event where a site's recruitment was too low (a minimum of five participants were needed to run the intervention at each program site), some participants were allocated to the intervention group instead of the control to allow the program to run. Thus, due to both low recruitment and program delivery logistics (i.e., working with multiple stakeholders and different regions across the province), this trial became a quasi-experimental design. Overall, EIP was delivered in program cycles starting October 2018 and January 2019, at one of the local community centers in B.C. (Prince George: YMCA of Northern B.C.; Kelowna: YMCA of the Okanagan; Surrey: YMCA of Greater Vancouver; Burnaby: City of Burnaby; and Greater Victoria: Westshore Parks and Recreation). Participants were recruited using social media platforms, stakeholder engagement, local newspaper advertisements, and posters and rack cards displayed in recreation centers, as well as mailed packages to physician offices. Interested participants were asked to contact the central site to determine study eligibility. This study adhered to the CONSORT statement reporting guidelines and was registered with www.ClinicalTrials.gov. The full trial protocol can be accessed on BMJ Open (https://dx-doi-org.web.bisu.edu.cn/10.1136/bmjopen-2018-027183). Informed consent was obtained from all parents, and children were asked to complete an ascent form confirming that they understood the terms of participating in the study. Participant consent and ascent were obtained before baseline data collection. Participants were informed that their participation in the study is voluntary and they are permitted to withdraw at any point in time without explanation. In addition, participant confidentiality was maintained throughout the study by having no participant names on any of the data. Ethics approval was obtained from the University of Victoria and University of British Columbia Research Ethics Boards (BC18-024).
Participants
Children who met the following eligibility criteria were recruited: (1) 8–12 years old; (2) at or above 85th percentile BMI-for-age and sex; (3) had no known health issues such as cardiovascular disease, mental health issues, or eating disorders, and (4) had one parent, caregiver, or legal guardian who was able to attend program sessions with the child. In the event that a child was above the 97th percentile BMI-for-age and sex, the parent was informed that the Shapedown program (a community-based program designed for children with higher levels of excess weight) may be better suited for their family; however, these families were still eligible to register for EIP. Ineligible participants included individuals who were unable to participate in physical activity and communicate fluently in English.
Intervention: Family Healthy Living EIP
The EIP was a community-based delivery model designed using evidence from previous implementation of family-based weight management interventions3,13–16 and feedback from community stakeholder consultations across five health regions of BC, Canada. See Supplementary Appendix SA for a breakdown of program sessions, activities, and weekly topics. The EIP provided face-to-face and remote support through the online family portal. Overall, the program provided 10 weekly face-to-face 90-minute sessions, four community-based activities (i.e., family grocery store tour), and the interactive web-portal. Topics covered throughout the intervention included physical activity, healthy eating, screen time, sleep, and positive mental health. 1 Intervention activities were designed to support parents and children in learning behavioral change skills, which provided them with the skills necessary to improve their health-related lifestyle behaviors. The EIP curriculum incorporated the M-PAC constructs as a strategy to introduce and guide families in initiating and maintaining healthy lifestyle behavior changes. The M-PAC framework introduces seven constructs that are precursors of health behaviors: (1) instrumental attitude as the knowledge on health consequences, (2) affective judgment relating to intrinsic motivation (i.e., benefits or enjoyment associated with executing a behavior), (3) perceived capability relating to self-efficacy, (4) perceived opportunity relating to perceptions of the social and physical environment (time and access), (5) behavioral regulation relating to tactics that people use to translate their intentions into behavior (e.g., goal setting, self-monitoring, and cognitive and emotional regulation), (6) identity as a standard of conscious self-comparison (i.e., making the behavior part of oneself), and (7) habit as a stimulus-enacted behavioral response under lowered conscious awareness, which enables an individual to maintain a behavior. Furthermore, all the M-PAC constructs correspond with a variety of BCTs defined throughout the behavior-change taxonomy. 12 BCTs, such as behavioral practice, goal setting, and self-monitoring, enable researchers to translate the M-PAC theory into specific intervention activities and lessons (see Supplementary Appendix SA and Supplementary Appendix SB for a full summary aligning the intervention activities/lessons, BCTs, and M-PAC constructs).
The weekly in-person sessions were delivered by trained facilitators. The sessions began with a fun physical activity and/or gratitude circle (each participant gives example of something he/she is thankful for) and were followed by activities and discussions. Generally, 15–20 minutes into the session, parents and children were separated into two groups. During the parent-only time, facilitators discussed how to utilize BCTs as tools for modifying families' dietary or physical activity behaviors. Particularly, the program emphasized setting S.M.A.R.T goals, which refer to a goal that is specific, measurable, achievable, realistic, and time sensitive. 17 Children participated in a variety of fun physical activities focused on developing basic physical literacy skills such as throwing, kicking, and catching. Toward the end of the session, parents and children would regroup and set at least one family goal for the upcoming week related to family mealtime, physical activity, or reducing sedentary behaviors.
The online family portal included 10 weekly lessons to be completed by families following the in-person session. Lessons on the portal included additional resource information on family healthy recipes, physical activity challenges, and mental-health related activities. Families were encouraged to complete at least 60 extra minutes per week of self-directed healthy lifestyle activities aimed at promoting healthy living. The online family portal also acted as a repository of materials covered in each in-person session.
Waitlist Control Group
The waitlist control group had access to a modified 10-week EIP: four group sessions and full access to the 10-week online family portal following the waitlist period. The four group sessions incorporated a condensed version of the content provided across the 10 weeks of the full EIP intervention; also, the waitlist control group was given access to the same online portal as the intervention group.
Procedure
Study outcomes were collected by research assistants at baseline and at 10-week follow-up at our program delivery sites. Demographic information was collected at baseline and included child's age and ethnicity, in addition to parents' annual household income and education. Furthermore, reliabilities were established for the following instruments with the present cohort of participants.
Primary Outcome
Child BMI z-score was calculated using the World Health Organization (WHO) criteria. 18 Child weight was measured to the nearest 0.1 kg and height was measured to the nearest 0.1 cm using standardized protocols and valid and reliable tools.
Secondary Outcomes
Children's moderate-to-vigorous physical activity was measured using a question drawn from The Physical Activity Questionnaire for Older Children (PAQ-C), which is a valid and reliable questionnaire for assessing children and adolescent (children 8–14 years old) PA levels (this study α = 0.79). 19 The questionnaire assessed the number of days in the past week that the children engaged in at least 60 minutes of moderate-to-vigorous physical activity (MVPA). Specifically, the question stated, “during the past week (7 days), on how many days were you physically active for a total of at least 60 minutes per day? Count all the time you spent doing activities that increase your heart rate or made you breathe hard” (response options were 0–7 days).
Children's screen-time and sedentary behavior were assessed using the Physician-based Assessment & Counseling for Exercise (PACE) Adolescent Psychosocial Measures (this study α = 0.75). 20 Four items from this questionnaire assessed the number of hours on a school day and a weekend day that children engaged in sedentary (i.e., sitting on the couch) and screen time (i.e., using a smartphone, TV, iPad, or computer) behaviors; responses ranged from zero hours to six or more hours. The items were, “on a school day, how many hours do you do sedentary habits? (like being a couch potato)?” and “on a school day, how many hours do you use smartphone, TV, iPad, computer, etc.?” The same two items were repeated for days children are not in school.
Child dietary behaviors (i.e., fruit and vegetable [FV] intake, sugary beverage and pre-packaged, non-nutritious, food consumption) were assessed using questions drawn from the Centre for Disease Control and Prevention Behavioral Risk Factor Surveillance System (BRFSS) 7-day recall (interclass correlation coefficient [ICC] = 0.50). 21 The BRFSS survey included a 7-day recall with questions such as, “in the last 7 days, how many times did you eat a green leafy or lettuce salad, with or without other vegetables” and “in the last 7 days, how many times did you eat doughnuts, brownies, pies, or cakes?” Responses represented the number of times in the past week that the child consumed fruits or vegetables (1: none, 2: 1–3 times, 3: 4–6 times, 4: 1 time per day, 5: 2 times per day, 6: 3 time per day, and 7: 4 or more times per day).
Parental support for healthy eating and physical activity was measured using subscales drawn from the FLASHES-EAT surveys (α = 0.77)22,23 and Parent Physical Activity Support Survey (α = 0.72).24,25 The healthy eating items (five-point Likert Scale: 1 strongly disagree and 5 strongly agree) were “I have to make sure that my child eats enough fruits and vegetables,” “I encourage my child to try different kinds of fruits and vegetables,” and “Bought fruit or vegetables you know your child likes.”22,23 The parental support for physical activity items (five-point Likert Scale: 1 strongly disagree and 5 strongly agree) were “I go out of my way to enroll my child in sports and other activities that get him/her to be physically active (e.g., after school programs, programs at the YMCA),” “I often watch my child participate in sporting activities (e.g., watch your child perform at a softball game or dance recital),” and “I take my child to places where he/she can be active” (see Supplementary Appendix SC for a full break-down of the measures used to assess the aforementioned secondary outcomes).
Self-regulation for healthy eating and physical activity support was assessed using questionnaires adapted from previous research for measuring self-regulation for eating (α = 0.86) and physical activity (α = 0.89).26–28 We assessed goal setting (for the behavior), review of behavioral goals, problem solving/coping planning, and action planning using a Likert scale (1: strongly disagree and 5 strongly agree). Specifically, the items included the following “I set short-term (daily or weekly) goals for how I could support my child's (healthy eating/leisure-time physical activity) behaviors last month,” “If I did not reach (my goal/one of my goals) for supporting my child's (healthy eating/physical activity) last month, I analyzed what went wrong,” “I made plans regarding what to do if something made it difficult to support my child's (healthy eating/physical activity) last month,” and “I made regular plans concerning “when,” “where,” “how,” and “what” kind of support “I could provide for my child's (eating behaviors and food choices/physical activity) last month” (see Supplementary Appendix SD for additional secondary outcomes that were assessed).
Process Evaluation
The EIP process evaluation assessed program reach (i.e., effectiveness of marketing strategies, recruitment, the extent to which the intervention is reaching intended populations, adherence, and attrition) and implementation (i.e., program satisfaction, program fidelity, attendance, engagement with the online portal, and barriers to program participation). Specifically, we assessed program reach by documenting site-specific recruitment plans, recruitment tracking forms, screening and phone calls tracking, demographic questionnaires, and program attendance tracking forms. Program implementation was examined by the following; screening tracking forms, facilitators preworkshop and postworkshop surveys, program attendance tracking forms, web portal analytics (i.e., total time, number of logins, and content accessed), facilitator feedback surveys, parents and children satisfaction surveys, and postprogram interviews with parents, facilitators, and stakeholders. This article briefly describes the results for program attendance and parent and child satisfaction; a comprehensive process evaluation report is provided elsewhere.
Statistical Analysis
The sample size calculation was modeled from results of a randomized controlled trial assessing the efficacy of a family-based intervention to reduce child BMI z-score compared to a control.1,3 According to the 2:1 group allocation, the predicted sample size was n = 70 for the intervention group and n = 35 for the waitlist control group (using a two-parallel group design, type 1 error = 5% and 80% power). We followed a stringent intention-to-treat protocol for analyzing our data. We conducted a sensitivity analysis to examine the impact of missing data on the outcomes of our analyses and thus (1) analyzed outcomes with only complete cases, (2) imputed the data using baseline observations carried forward (BOCF) and repeated the analyses, (3) used multiple imputation methods and repeated the analyses, and then (4) compared findings from the analyses conducted in scenarios 1, 2, and3.29,30 Overall, there were no differences in the results using the various methods to account for missing data, which, compared to prior research, is not an unusual finding. 31 Previous studies have suggested that BOCF is a more conservative approach than multiple imputation and multiple imputation should be used with caution when sample sizes are small and the proportion of missing data is high.31–34 Therefore, we used the BOCF method in our study.
Analysis of group differences at baseline was conducted with independent t-tests for continuous variables, and with chi-square tests for categorical variables. Distributions of the continuous variables were assessed for normality. Univariate linear regressions were used to compare the change in primary (BMI z-score) and secondary outcomes (changes in children's dietary, physical activity, sedentary and screen time, parental support for healthy eating and physical activity, and self-regulation for healthy eating and physical activity support) between groups. In addition, the univariate linear regressions were adjusted for baseline measures. To account for nesting of the family system, one child per family was included in the final analysis. Statistical significance criterion was defined as p < 0.05. We also used effect size to determine intervention effects. Effect sizes were reported using partial eta squared (ηp 2 ), whereby 0.01, 0.06, and 0.14 were benchmarks for small, medium, and large effect sizes, respectively. 35
Results
The flow of the participants through the study is displayed in Figure 1. Of those contacted, 53 of 170 (31%) did not meet the inclusion criteria. Of those remaining eligible, 39 of 117 (33%) dropped out before program commencement and 7 of 117 (6%) did not attend baseline assessment. Finally, a total of 48 children were allocated to the EIP and 23 children were assigned to the wait-listed control. Demographic characteristics of the study participants are displayed in Table 1. The child participants included 33 (45%) females and 39 (54%) males with an average age of 10.13 years (standard deviation = 1.49; age range = 7.25–13.25). The program reached a demographic representing the BC population, 36 whereby more than a third of children were white, almost a 10th were Indigenous, approximately one-fifth were Asian (South Asian, East Asian, Chinese, and South East Asian), one fourth were multiple ethnicities, and almost one-10th were black or Latin American. Baseline BMI z-score, dietary behaviors, physical activity-related outcomes, and parental support regulation for child's healthy eating and physical activity were similar between the groups (Table 2).
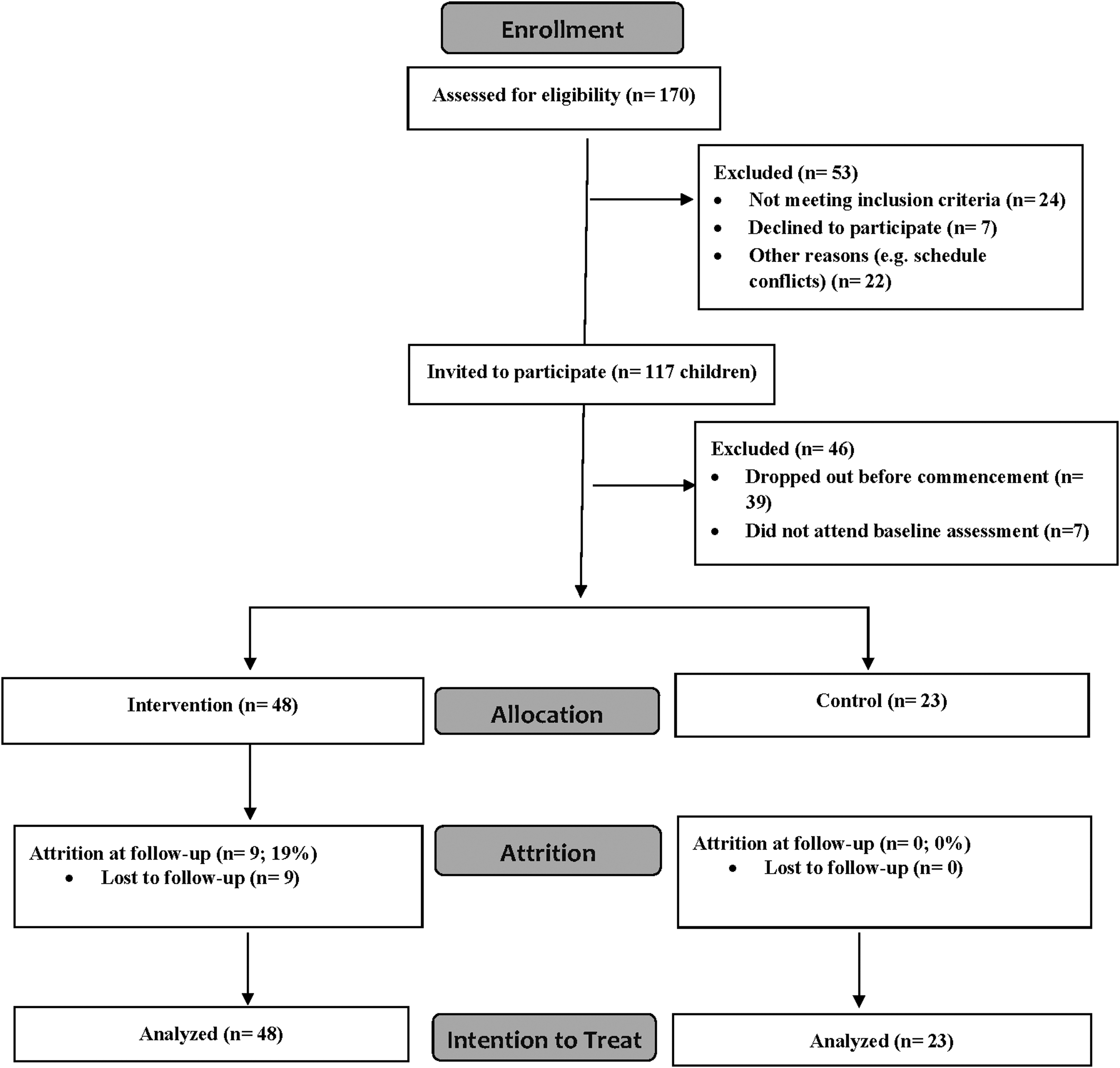
CONSORT diagram participant flow.
Demographic Characteristics
Data are presented as mean ± SE or number of participants (%).
Asian = South Asian, East Asian, Chinese, and South East Asian.
Other = Black, Latin American.
Six participants prefer not to answer this question.
Three participants prefer not to answer.
SE = standard error.
Baseline Characteristics
Data are presented as mean ± SE.
These items were reverse coded (i.e., a lower score indicates a low sugary drink intake).
BMI, body mass index; MVPA, moderate-to-vigorous physical activity; PA, physical activity.
Changes in primary and secondary outcomes at 10 weeks relative to baseline are displayed in Table 3. BMI z-scores were not significantly different between the intervention and control group (p > 0.05; ηp 2 = 0.01). However, the intervention group significantly improved the children MVPA level relative to control (p < 0.01; ηp 2 = 0.10). The reduction in screen time observed following the intervention relative to control also approached significance (p = 0.07; ηp 2 = 0.05). There was no statistical significance between group differences for changes in child fruit, vegetable, and sugary drink intake (p > 0.05). Parental support for healthy eating (n 2 = 0.06) and physical activity (n 2 = 0.06) significantly improved in the intervention group relative to the control (p < 0.05). Self-regulation for healthy eating behaviors (p < 0.01; ηp 2 = 0.11) and physical activity (p < 0.05; n2 = 0.28) significantly increased among the intervention group relative to the control with a large effect size (Table 3).
Changes in Primary and Secondary Outcomes at 10 Weeks Relative to Baseline
Data are presented as Δ mean ± SE.
These items were reverse coded.
Significant outcome (p < 0.05).
PA, physical activity.
Program attendance at the weekly in-person sessions was 58%, which included participants who dropped out of the program (92% of children who dropped out did so during the first 3 weeks). In-person sessions were well attended by families who completed the program, whereby 85% of children attended 70% or more of the weekly sessions. Finally, 92% of children who dropped out of the program did so during the first 3 weeks (two children dropped out after week 4). Feedback from parents and children who completed the postprogram satisfaction surveys was positive. Overall, families reported that they were highly satisfied, enjoyed participating, and felt that the program went well. Particularly, parents reported that the program provided a safe and inclusive environment, as well as multiple opportunities and tools to make positive lifestyle changes. Parents who completed the satisfaction surveys also found that the information given in handouts was easy to understand, respectful, adequate, and timely for their families and the population of British Columbia (see Supplementary Appendix SE for tables displaying the results of all additional outcomes).
Discussion
This study evaluated the effectiveness of a 10-week blended, family-based weight management intervention on improving children's BMI z-scores, lifestyle behaviors, and parental support behaviors. To our knowledge, this is one of the first blended family-based childhood obesity management program developed using the MPAC framework.11,26,37,38 Our results showed that relative to control, the EIP significantly improved children's self-reported MVPA and parental support for healthy eating and physical activity, as well as self-regulation for healthy eating and physical activity support. However, child BMI Z-scores and dietary behaviors did not significantly change relative to control.
There are a few factors that may have contributed to the intervention's null effect on child BMI z-score. First, the EIP differed from many obesity management interventions as it shifted its focus from weight loss to making healthy lifestyle behavior changes. 3 Second, a 10-week program may be too brief to expect child participants' BMI to significantly reduce. A meta-analysis examining the effectiveness of family-based lifestyle interventions reported that larger effect sizes for child weight outcomes were associated with longer intervention (i.e., treatment) duration, a greater number of intervention sessions, and total amount of time the child spent engaged in the intervention. 14 Additional research is needed to determine optimal program content and mode of delivery (i.e., frequency of in-person sessions and smartphone application versus web-based platform designed for computers) for a blended family-based intervention.
Furthermore, child BMI z-scores are typically the primary measure used for assessing adiposity at one time point; however, this measure does not necessarily account for changes in child adiposity since within-child variability across time depends on the child's initial level of adiposity. 39 Nevertheless, we chose to measure and report child BMI z-scores as opposed to measuring waist circumference or bioelectric impedance to assess fat mass versus lean mass, due to its low cost, minimal equipment requirement, and less invasive nature for participants. Future interventions should explore the possibility of using measurement tools that are more sensitive to changes in child body composition, while continuing to protect children's mental and emotional health and minimize participant burden.
Our results showed a large magnitude of increase for child MVPA was significantly greater in the intervention group than control. On average, the intervention group added almost 1 day per week of at least 60 minutes of MVPA compared to control, which is comparable to previous findings.3,40 One of the reasons for this improved physical activity outcome was because the EIP provided multiple opportunities during each session for children to engage in physical activity games or skills and the online portal incorporated weekly family-based physical activities for families to complete at home. Furthermore, the EIP taught families to use planning and goal setting to increase physical activity. This is reflected in the improvement in parental support physical activity as well as self-regulation for physical activity support. These findings are similar to a family-based intervention for child physical activity, whereby children with parents that participated in the “planning” intervention condition significantly increased MVPA compared to the “education” condition. 37
The EIP did not show a significant change in children's dietary behaviors. However, the improvements in parental support for healthy eating and self-regulation for healthy eating support are noteworthy findings, given parents' substantial impact on children's lifestyle behaviors.27,41–44 The lack of significant change in children's dietary behaviors may be due to a ceiling effect as children are already consuming fruit and vegetables about five times per day in a typical week at baseline. Similarly, a ceiling effect may have occurred for child sugary drink intake, whereby, on average, children in both groups reported, at baseline, consuming no sugary drinks or consuming sugary drinks 1–3 times in the last 7 days. Thus, beginning the intervention, many children were already consuming few sugary drinks. Furthermore, the unit of measure for dietary change in this study (times per day in a typical a week) may not be as sensitive to detect change over the 10-week period compared with instruments that measure servings of fruit and vegetable intake per week. 45 Future research may also consider investigating new dietary assessment protocols such as ecological momentary assessment that use smartphone applications or web-based programs. This method may reduce participant burden and improve the accuracy of dietary intake data. 46
There are several limitations to this study that require consideration. First, we did not achieve our a priori sample size goal due to low recruitment. The 2:1 allocation may have reduced our statistical power. Thus, when reporting study outcomes, we also interpreted effect size. We choose this analytical and data presentation strategy because effect size is independent of sample size, whereas p values depend upon both sample size and effect size. 47 Several participants dropped out before baseline assessment and commencement of the study, which contributed to not reaching our desired sample size. One potential reason for these dropouts was the program had a specific start date. Some families may lose interest while waiting for program to start. Future studies may consider facilitating a preintervention phase with families during which they explore participants' expectations regarding treatment goals and forms of support provided by the program in an effort to maintain participants' interest and engagement in the full 10-week program. Furthermore, this study was developed and evaluated using the M-PAC framework, a meta-theory that has been extensively tested with physical activity behavior,48,49 and has recently been extended to explain sleep and sedentary behaviors. 26 Thus, because the M-PAC framework has not been tested as a model for describing intentions and behaviors related to parent and child dietary behaviors or parent feeding practices, our findings should be interpreted with caution. Further research is needed to test the efficacy of the M-PAC framework for delivering and evaluating nutrition interventions. The generalizability of our findings is limited due to our small sample size and the short study follow-up period. A larger scale randomized control study with a longer follow-up period (1 year) is needed in the future.
Conclusion
This study evaluated the effectiveness of the EIP, a 10-week blended family-centered intervention aimed to promote healthy lifestyle for children who are overweight and obese. Blended interventions, incorporating face-to-face and web-based components, have the potential to improve the flexibility, and scalability of intervention delivery. Our results showed that the EIP, relative to control, significantly improved children's MVPA, parental support for healthy eating and physical activity, and self-regulation for healthy eating and physical activity support. The short study duration may have contributed to the nonsignificant changes in BMI z-score. A randomized controlled study design with a longer evaluation period is warranted.
Footnotes
Authors' Contributions
M.P., S.L., R.R., and P.-J.N. contributed to the data analysis, data interpretation, and article writing. S.L., K.S., and P.-J.N. contributed to the study design, data collection, and analysis. M.P., T.H., and K.S. contributed to data collection and analysis. All authors read and approved the final article.
Funding Information
This study was supported by the Childhood Obesity Foundation with funding from the British Columbia Ministry of Health and MITACS accelerate grant.
Author Disclosure Statement
Authors M.P., S.L., and R.R. have no conflicts of interest relevant to this article to disclose. Authors T.H. and K.S. disclose that the Province of BC provided funding to the Childhood Obesity Foundation for the delivery and evaluation of the Early Intervention Program. Author P.-J.N. reports grants and nonfinancial support from the Childhood Obesity Foundation during the conduct of the study, and P.-J.N. volunteers as a board member of the Childhood Obesity Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.