
Abstract
Background:
Obesity leads to serious health consequences in children and is potentially associated with increased adverse childhood experiences (ACEs). Nationally representative studies examining associations between obesity and ACEs are lacking. Therefore, we aimed to determine the relationship between ACEs and childhood obesity.
Methods:
We performed a retrospective cross-sectional study of children 10–17 years of age, who participated in the 2018 National Survey of Children's Health (NSCH), a national population-based survey. Obesity was determined by CDC definitions using BMI calculated by the NSCH from self-reported height/weight. Logistic regression, adjusted for key sociodemographic factors, determined differences in rates of ACEs between children with obesity (BMI ≥95th percentile) and those without (BMI <95th percentile).
Results:
Weighted NSCH data included 29,696,808 children 10–17 years of age, 15% with obesity. Obesity was associated with having more ACEs compared to other children (p < 0.01). In adjusted analyses, children with obesity were more likely than other children to report most ACEs, including food/housing insecurity [adjusted odds ratio (aOR) 1.64, confidence interval (95% CI) 1.26–2.13], parental divorce [1.67 (1.32–2.13)], witnessing physical violence [1.49 (1.03–2.16)], be a victim of violence [1.99, (1.27–3.12)], or live with a person with drug/alcohol abuse [1.65, (1.24–2.2)]. Children with obesity were also more likely to report ≥4 ACEs compared to other children (p < 0.001).
Conclusion:
Children with obesity are more likely to report ACEs overall and have more ACEs compared to other children. Obesity negatively affects child health; in combination with ACEs, health outcomes of children may be disproportionately affected, highlighting the importance of preventive screening and social interventions in childhood.
Introduction
Adverse childhood experiences (ACEs) are common among children in the United States, with >20% experiencing some form of ACE (e.g., economic hardship, parent/guardian divorce, and child maltreatment) during childhood, 1 and ∼61% of adults reporting experiencing an ACE in their lifetime. 2 ACEs are associated with poor health, economic, and social outcomes across the lifespan, with risk of poor outcomes for many of the leading causes of morbidity and mortality in adults increasing as the number of ACEs experienced increases.3–6 Particular groups have been found to experience ACEs at higher rates, including children who are older, non-Hispanic blacks, those with special health care needs, and those living in rural areas. 1
Obesity is also associated with increased risk of poor health outcomes in children and into adulthood. Prior studies examining children with obesity have shown they experience higher rates of morbidity and mortality from medical problems (e.g., hyperlipidemia and diabetes mellitus), mental health problems (e.g., depression and anxiety), and psychosocial stressors (e.g., bullying and poor self-esteem).7–9 Despite public health efforts to abate the childhood obesity epidemic, rates continue to climb in children, now affecting an estimated 18.5% of youth 2–19 years of age, with adolescents and minority children experiencing obesity at disproportionately high rates. 10
While ACEs and obesity are each more likely to affect minority children and children of lower socioeconomic status, there is some evidence to suggest that ACEs may independently increase the risk of obesity in both children and adults, perhaps tied to physiologic changes resulting from chronic toxic stress. 2 Adults who reported experiencing ACEs were more likely to have obesity than adults who did not report ACEs.11,12 In addition, studies of children found associations between having experienced ACEs (even early in childhood) and having obesity as a child.13,14 However, existing studies examining the links between ACEs and childhood obesity are limited in size and scope, unable to provide detailed information representative of the general US pediatric population and lacking analysis of some patient clinical characteristics (e.g., diverse age groups and chronic illness). Therefore, we aimed to examine associations between ACEs and childhood obesity utilizing a nationwide representative sample of the US population, the National Survey of Children's Health (NSCH). We hypothesized that having obesity would be associated with having ACEs, and children with more ACEs would be more likely to have obesity than children with no ACEs.
Methods
Study Design
This retrospective cohort study examined all children 10 to 17 years of age included in the NSCH administered in 2018. The NSCH is a large, nationally representative survey conducted and funded by the Maternal and Child Health Bureau and Health Resources and Services Administration, and conducted by the Census Bureau that aims to provide state- and national-level data on the physical and mental health of American children 0–17 years of age. 15 These survey data, reported by a parent/guardian on behalf of a child within their household through either paper or web-based survey, contain a wealth of information on many aspects of children's health and wellbeing, including demographics, anthropometric information (height and weight), chronic health conditions (medical and mental health), and ACEs. The 2018 NSCH survey was completed by >30,000 households across the United States, and weighted estimates can be used to generalize to state- and national-level child populations. 16 The data are made publicly available on the Data Resource Center for Child and Adolescent Health website, and through the Census Bureau. This study was deemed nonhuman subjects research by the Institutional Review Board at Children's Mercy Hospital (Kansas City, MO).
Study Population
We included data collected on all children 10–17 years of age in the 2018 weighted NSCH dataset. Younger children 2–9 years of age were excluded because there was no anthropometric information collected in this group, as prior work has shown that parental reporting of weight information is poor compared to that of older children and adolescents. 17 We also excluded any child with incomplete data for individual NSCH ACE survey items (e.g., if a participant answered some, but not all, of the ACE questions). This included ∼6.5% of the overall NSCH cohort. When comparing this group of excluded children to the included cohort, some differences existed between the two groups. Excluded children were more likely to have been minority (non-Hispanic Black and Hispanic) children (p = 0.001), children in the lowest median household income quartile (p = 0.001), and children with public insurance (p < 0.001). No differences existed between included and excluded children based on age, sex, or clinical characteristics.
Demographic characteristics collected included age, sex, race/ethnicity, insurance payer, and median household income quartile (as measure of socioeconomic status). Clinical characteristics collected included presence of chronic medical and mental health conditions reported in the NSCH. Chronic medical conditions included asthma, diabetes, epilepsy, deafness, brain injury, intellectual disability, and cerebral palsy. Chronic mental health conditions included learning disability, attention-deficit and hyperactivity disorder, depression, anxiety, behavioral problems, autism, developmental delay, speech disorders, and Tourette syndrome. These conditions were included to provide clinical information regarding the overall health of the included population, as obesity is known to be associated with chronic medical and mental health conditions. All chronic medical and mental health condition information was collected on the 2018 NSCH using the question stem “Has a doctor or other health care provider EVER told you that this child has [health condition].”
Study Measures
The primary exposure for our study was weight category. The NSCH-determined weight category is based on BMI calculated from caregiver-reported height and weight measurements. Publicly available reported weight categories included underweight, healthy weight, overweight and obese based on Centers for Disease Control and Prevention definitions. To achieve the objectives of this study focused on obesity, we categorized participants as either children with obesity (BMI percentile ≥95th for age/sex) or children without obesity (BMI percentile <95% for age/sex) according to current Centers for Disease Control and Prevention definitions.
Our primary outcome measures were the proportion of children experiencing any ACE, and the proportion of children experiencing each individual ACE collected in the NSCH. We also examined the association between having obesity and the number of ACEs reported. ACEs included in the NSCH and our analysis were childhood experiences of having difficulty covering basics (e.g., food/housing), parent/guardian divorced, parent/guardian died, parent/guardian spent time in jail, being a victim of violence, witnessing violence (adults slap, hit, kick, or punch others), living with person with mental illness, living with person with alcohol/drug problem, and being treated unfairly because of race. We also assessed the number of ACEs reported by weight category, ranging from 0 to ≥4.
It is important to note that instruments used to measure ACEs differ somewhat in the variables/ACEs included, and the NSCH is no exception. For example, the NSCH includes one ACE that is a surrogate for poverty (i.e., having difficulty covering basics), which is not included in some other commonly used ACE measurement tools, but has been studied as an ACE in the past. 18 The NSCH ACEs do not include questions regarding all forms of child maltreatment (e.g., physical abuse and neglect), which are commonly measured ACEs. However, following the addition of ACEs to the NSCH in recent years, this tool has shown to have good predictive validity for measuring ACEs and for the use of ACE cumulative risk scoring. 19
Statistical Analysis
Demographic, anthropometric, and clinical characteristics were summarized using frequencies and percentages. For the purposes of analysis, survey responses of “somewhat often” and “very often” were considered “Yes” for having difficulty covering basics like food/housing. Statistical differences in unadjusted outcomes across weight categories were calculated using the chi-square test. Logistic regression was used to determine differences in (1) the unadjusted proportion of children having any ACE between weight categories and (2) proportions of children having individual ACEs between weight categories, with adjustments for covariates with statistically significant differences between weight categories in chi-square analyses: race/ethnicity, and presence of chronic medical and/or mental health condition. We did not adjust for median household income or insurance to avoid introducing multicollinearity between these factors and ACEs highly correlated with income/poverty (i.e., having difficulty covering basics). All statistical analyses made use of the sampling weights provided in the NSCH and were performed using SAS 9.4 (SAS Institute, Cary, NC), and p-values <0.05 were considered statistically significant.
Results
Cohort Characteristics
The NSCH included weight data for 29,696,808 children 10–17 years of age for the year 2018 (Table 1). Most children were 10–14 years of age (62.2%), male (51%), and identified as non-Hispanic white (51.1%), and had private insurance (59.8%). Approximately 4,460,654 (15.0%) children had obesity. Statistically significant differences existed between demographic groups by weight category for race/ethnicity (minority groups more likely to have obesity, p < 0.001) and insurance payer (publicly insured children more likely to have obesity, p < 0.001). Differences were also across weight category for median household income, with children with obesity more likely to be in the lower income quartiles than other children (p < 0.001).
Cohort Demographics
Weighted percentages.
CI, confidence interval; OR, odds ratio.
A majority of children (67.7%) were reported as having no chronic medical and/or mental health conditions, including 7.5% with medical conditions, 18.8% with mental health conditions, and 6.0% with both (Table 1). Children with obesity were more likely to experience chronic medical and mental health conditions compared to other children (p < 0.001).
Proportion of Children with Any ACE by Weight Category
Overall, 14,656,253 children (49.4%) were reported as having experienced any ACE (Table 1). Children with obesity were more likely to experience any ACE compared to children without obesity [odds ratio (OR) 2.25 confidence interval (95% CI 1.82–2.78), p < 0.001], with certain groups of children with obesity experiencing particularly high odds of having any ACE (Table 1). For example, children with obesity 10–14 years of age [OR 2.74 (2.13–3.53), p < 0.001], females [OR 2.65 (1.91–3.68), p < 0.001], Hispanic children [OR 2.55 (1.55–4.21), p < 0.001], children in the lowest median household income quartile [OR 3.31 (1.99–5.5), p < 0.001], and those with both mental and medical chronic health conditions [OR 2.8 (1.5–5.2), p = 0.001] had higher odds of having any ACE compared to other demographic or clinical groups. No demographic or clinical groups of children with obesity possessed a lower risk of having any ACE compared to children without obesity.
Unadjusted Proportions of Individual ACEs by Weight Category
Proportions of each ACE reported occurred variably, ranging from 4.6% of all children experiencing the death of a parent/guardian to 32.8% of children having a parent/guardian divorced (Table 2). Children with obesity were more likely than other children to have experienced any ACE (66.1% vs. 46.4%, p < 0.001). Of the nine ACEs examined in this study, all were more likely to be experienced by children with obesity (p < 0.03 for all) (Table 2). The most common ACE was parental divorce, reported by 43.8% of patients with obesity (compared to 30.9% of other children, p < 0.001). Other ACEs with larger differences in proportions between weight categories included being a victim of violence (11.4% of children with obesity vs. 5.4% of other children, p < 0.01) and having lived with a person with an alcohol/drug problem (16.1% vs. 10.2%, p < 0.001).
Unadjusted Percentages a of Adverse Childhood Experiences by Weight Category
Weighted percentages.
Chi-square test analysis.
Association of Obesity and Number of ACEs
Overall, 15,040,527 children (50.6%) were reported to have no ACE, while only 33.9% of children with obesity had no ACEs (Fig. 1). Children with obesity were significantly more likely to experience a large number of ACEs compared to other children, with 12.3% of children with obesity reporting ≥4 ACEs compared to 7.5% of children without obesity (p < 0.001).

Number of ACEs by weight category*. *p < 0.01 denoting a statistically significant difference in the proportion of children with and without obesity by number of ACEs. This shows that children with obesity were more likely to experience higher number of ACEs compared to children without obesity. ACEs, adverse childhood experiences.
Adjusted Associations between Individual ACEs and Weight Category
When adjusting for key sociodemographic factors that are known to be associated with obesity (race/ethnicity and presence of a chronic health condition) we found that five of the ACEs examined (55.6%) were independently associated with obesity, including hard to cover basics like food/housing [adjusted OR (aOR) 1.64 (95% CI 1.26–2.13), p < 0.001], parent/guardian divorced [aOR 1.67 (1.32–2.13), p < 0.001], witnessing violence [aOR 1.49 (1.03–2.16), p = 0.034], being a victim of violence [aOR 1.99 (1.27–3.12), p = 0.003], and living with a person with drug/alcohol problems [aOR 1.65 (1.24–2.2), p < 0.001] (Fig. 2).
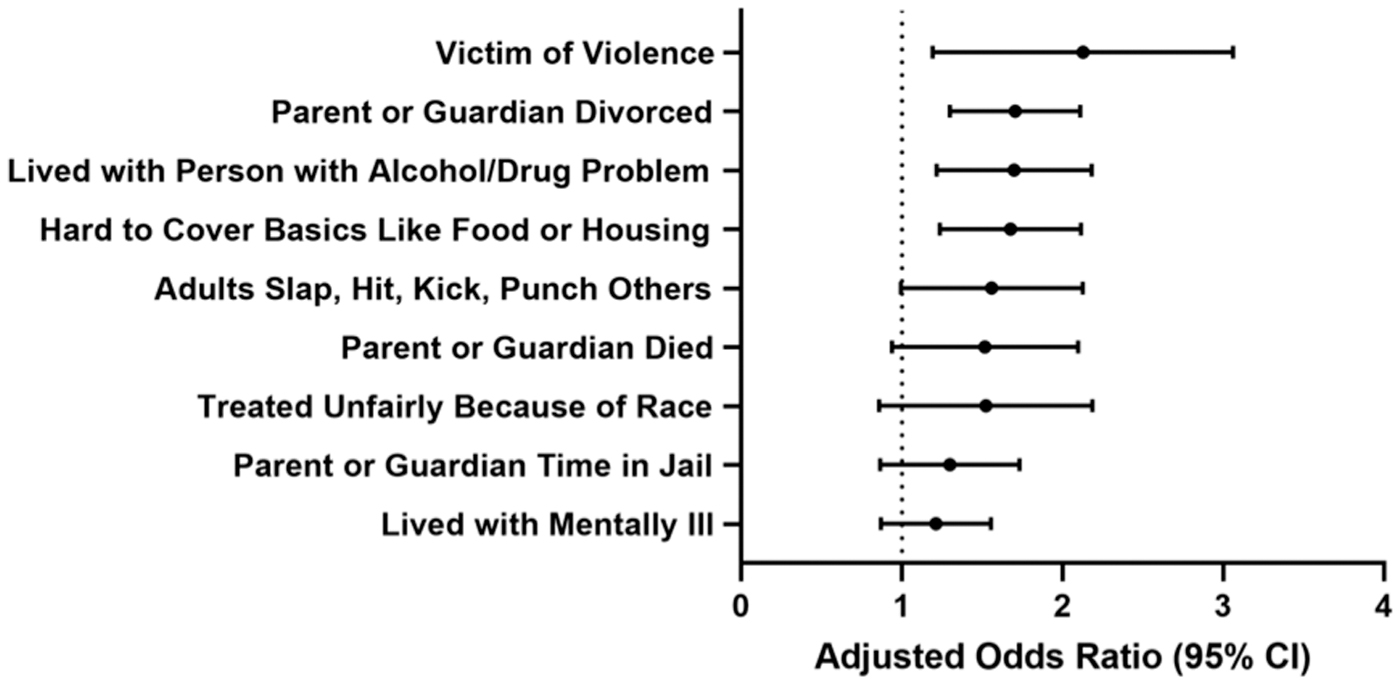
Adjusted⋄ odds ratios* of ACEs by weight category. ⋄Analysis was adjusted for race/ethnicity and number of chronic medical and mental health conditions. *Reference category: no ACE, except for “Hard to cover basics like food or housing” for which the reference value includes “Never” and “Rarely” experienced. CI, confidence interval.
Discussion
In this study of a nationally representative weighted sample of >30 million US children 10–17 years of age, we found that children with obesity were more likely to have experienced both any ACE and individual ACEs compared to children without obesity. When controlling for important demographic and clinical factors known to be associated with obesity, the association between having experienced ACEs and obesity remained for five of nine ACEs examined. As the number of ACEs experienced increased, the likelihood of having obesity also increased.
This study adds to existing literature regarding ACEs and obesity by providing an analysis of a nationwide sample of children for multiple reported ACEs. A prior state-level analysis by Davis et al. similarly demonstrated that children reporting ACEs were more likely to have obesity than those who had not experienced ACEs. 13 Another study by McKelvey et al. showed that even ACEs experienced during infancy and early childhood were associated with having obesity later in childhood. 14 Our findings show that ACEs experienced at any point in childhood may be associated with having or developing obesity in childhood/adolescence. In addition, we found that some demographic and clinical characteristics are associated with higher odds of a child with obesity reporting any ACE. These findings are overall similar to demographic associations seen in the general population, but add information about the degree of the association seen for different groups of children with obesity.
Our results also align with prior work demonstrating that those who experience higher numbers of ACEs may be more likely to experience poor health outcomes. 2 Our results showed an increasing association with having obesity as the number of ACEs experienced increased. Prior literature has proposed the mechanism for development of chronic disease linked to ACEs as a result of physiologic changes from toxic stress, including alterations in circulating hormone levels (e.g., cortisol) and proinflammatory cytokines, 2 negatively affecting an individual's physical and emotional response to stress. Similar physiologic changes occur in individuals with obesity, which may contribute to their overall risk of chronic disease.20,21 The physiologic consequences of this negative cumulative effect of multiple ACEs may drive the development of obesity and many other chronic diseases in late childhood and adulthood.
Both ACEs and obesity are each known to lead to substantial negative health outcomes across the life span, in addition to considerable psychosocial and economic costs. Although prior work has estimated that the population attributable fraction of cases of obesity that may result from ACEs is small (just 1.7%), 2 the combination of ACEs and obesity may put children and adults experiencing both at disproportionately higher risk of adverse health outcomes. Also, children with obesity are more likely to experience bullying and other psychological traumas, which may cumulatively affect their overall health and well-being.22,23 Considering the high prevalence of both obesity and ACEs in childhood, these issues are imperative to address as the combination of obesity and ACEs may disproportionately affect an individual's health outcomes into adulthood.
Many ACEs are preventable events, with studies demonstrating substantial reductions in some ACEs (e.g., physical abuse) through targeted early childhood interventions, including parental education and other social services.23,24 Nationwide initiatives exist to provide strategies and goals for reduction in ACEs through alteration of risk factors,25,26 and the American Academy of Pediatrics has provided many screening tools for primary care providers to assess for social needs and resiliency in families. 27 Both ACEs and obesity are closely tied to socioeconomic factors, disproportionately impacting poor families and children.2,10 Focusing continued implementation of screening measures and interventions aimed at reduction of poverty will help mitigate the increased risks experienced by those suffering ACEs and obesity.5,6 Continued advocacy and health policy efforts aimed at reduction of poverty and other risk factors for experiencing ACEs are also imperative for reduction of risk on a larger scale.
This study should be viewed in light of several limitations. First, the ACEs measured by the NSCH are not comprehensive and lack important and frequently measured ACEs like child physical abuse or neglect, and include some ACEs that are less frequently studied, including measures of poverty and racism experienced outside the home. In addition, all NSCH data are reported by parents/guardians, including anthropometric measures used to determine obesity as well as ACEs, introducing the possibility of recall bias. This may explain the difference in obesity rates in our sample (15.1%) compared to other nationally representative samples (e.g., NHANES, obesity rate of 18.5% 10 ). The reporting of ACEs included in the NSCH is also likely limited by the fact that they are reported by the child's parent/guardian. Due to a lack of complete ACE survey data, 6.5% of children 10–17 years of age were excluded, and some differences existed between this group and the included cohort, namely minority children, children with public insurance and those belonging to the lowest median household income quartile were more likely to be excluded, which may introduce some bias into our results. Our study only included ages 10–17 due to lack of anthropometric data for children 2–9 years of age, limiting generalizability of our results for younger children. In addition, reporting of chronic medical and mental health conditions was limited to only some examples of common conditions. The population of children experiencing chronic conditions was oversampled in the NSCH survey to improve accuracy of analysis of this smaller group, but the list of conditions is not exhaustive and may therefore limit application of our results. Finally the data collected in the NSCH for ACEs are collected at a single point in time, but might have been experienced at any point in the child's life.
Conclusions
Children with obesity are more likely to have experienced ACEs compared to children without obesity. Additionally, the association with obesity increased as the number of ACEs reported increased. With ACEs and obesity leading to serious negative health, social, and economic outcomes, these results highlight the importance of widespread implementation of ACE screening in all health care settings, as well as preventive interventions for obesity and ACEs on both the individual and policy level.
Footnotes
Authors' Contributions
K.E.K. proposed the study idea, participated in the study design, analysis, and interpretation of the data, and was the primary author of the article. M.H. participated in the study design, acquisition, analysis, and interpretation of the data, and has provided critical intellectual content in the revision of the article. E.H. and A.D. participated in the study analysis and interpretation of data, and have provided critical intellectual content in the revision of the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.