
Abstract
This project characterized the system of childhood obesity-related programs and functions based on a socioecological framework within the Kansas City region to determine strengths, weaknesses, and leverage points for informing collective impact. A mixed-method approach was employed to identify and collect data ∼260 childhood obesity-related programs provided by 89 organizations. Findings indicated no major gaps in population or location served although few programs specifically focused on service to minority groups or neighborhoods. The region has many programs working within the system, yet the distribution of programs does not occur as expected throughout the dimensions of a standard socioecological model or community health system. In addition, several organizations perform certain leadership functions such as coordination, resource allocation, or monitoring, but none perform all, indicating the lack of a traditional “backbone” organization. These findings demonstrate how a region's childhood obesity prevention and treatment programs can be evaluated using a socioecological framework.
Introduction
It is without dispute that childhood obesity is one of the most serious public health problems of the 21st century, given the prevalence, global reach, and widespread health, economic, and social consequences. Socioecological models have been developed over the past two decades to facilitate an understanding of multiple levels of influence on various health behaviors including eating and physical activity, 1 and consequently they can be used to inform comprehensive childhood obesity interventions. One of the key aspects of socioecological models is that they highlight the need for multiple levels of interaction to create enduring widespread change within systems impacting obesity.2,3 A systems approach to obesity prevention has been emphasized2–8 to highlight interactions and feedback loops among the elements within such systems, and underlines the importance of including leadership and policy change.2,9,10 However, this can be challenging from a practical perspective, given that many levels of influence consist of organizations that are formed to function as independent entities, not as components of a larger comprehensive system.
Purpose and Objectives
Kansas City's childhood obesity prevention and treatment system, similar to other regions, is not a predesigned planned system. It has emerged in an ad hoc organic way that inevitably exhibits inconsistencies and overlaps. The purpose of this project was to identify and document the programs within the naturally occurring system of childhood obesity prevention and treatment in the Kansas City region. This study employed a socioecological approach to identify programs and characterized each regarding system functions, populations served, and level(s) and forms of intervention. Any program that reported it and addressed one or more functions relevant to the prevention or treatment of childhood obesity was included. In addition, we examined whether any existing entity has the capacity to serve as a backbone organization capable of guiding the obesity prevention and treatment system and address overlaps, gaps in coverage, and planning and coordination issues.
Methods
This mixed-methods study was designed to identify and characterize all childhood obesity programs that operated in the Kansas City region that includes five counties (Jackson, Clay, Platte, Wyandotte, and Johnson) and spans two states (Missouri and Kansas). The population of the region is 1,825,207, the population of White residents ranged from 67.1% in Wyandotte County to 86.6% in Johnson County, the population of Black residents ranged from 4.9% in Johnson County to 23.7% in Jackson County, and the population of Hispanic/Latino residents ranged from 6.3% in Platte County to 29.8% in Wyandotte County. 11 The percentage of the population in poverty ranged from 5.3% in Johnson County to 20.6% in Wyandotte County. 11
To inform the development of our schema for characterizing our region's childhood obesity intervention system, we began with a core framework drawn from the conceptual models employed in several widely accepted socioecological models and community health system function (Fig. 1).12–15 Formal definitions of the community health system dimensions are provided later in the Methods section. We then refined this framework with the advice of an advisory council of 18 key informants to determine the specific socioecological dimensions of the childhood obesity system and program functions to be mapped. This advisory council included expert members from various facets of this field, including the local YMCA, local, county, and state departments of health, weight management clinic medical directors, and nonprofit early childhood and family support programs. The advisory council helped define the key functions and which agencies performed those functions related to prevention (healthy eating and active living) and treatment of childhood obesity, identified the various community leaders, professional resource people and agencies engaged in related functions and activities, encouraged and facilitated communication and connections between the project team and appropriate community entities to be reflected on the map, and provided advice and feedback to the project team on the development, content, and format of the report.

Conceptual framework to describe the relationship between community health system dimension and socioecological model level. Color image is available online.
Regional childhood obesity program identification and data collection began with an extensive Internet web search. Research staff first used program and organization websites and literature to complete as many fields in the data framework as possible, and then gathered data for the remainder of the fields for each program through telephone interviews with program leaders or other key informants to confirm or correct the data collected for each program. Snowball sampling was also conducted based on solicitation from program leaders, the project advisory council, and other key informants in the system. Sampling continued until saturation was achieved (no new programs identified).
All data were collected in a Microsoft Access database to guide the data collection process and store the data in a uniform manner. Program information was collected for the following categories: geographic scope, delivery setting, client focus, system function, and socioecological dimension. Information also was gathered about each program's host organization, including annual budget, funding sources (government and/or private), and organization type (nonprofit, for-profit, government, or collaboration). Multiple research staff coded all programs for each category, and any discrepancies in coding were resolved through consultation with additional staff. Geographic scope or jurisdiction was determined by choosing their service area from a list of 10 location options (national, state, bistate, region [federal designation], city/municipality, Greater Kansas City, multiple cities, county, multiple counties, and neighborhood). Delivery setting was determined based on where the program was administered (e.g., school, community center, and health care facility). Client focus or intended recipients for services (e.g., infant, early childhood, pregnant and childbearing ages, and professional), as well as whether the program especially targeted particular types of clients (e.g., all income levels or primarily low income; focus on clients of specific race or ethnicity) was determined for each program.
Community health system function refers to the role a program serves within the larger childhood obesity system in the Kansas City region. System functions were identified based on concept mapping and community health systems literature, 14 and modified to reflect obesity-specific considerations.8,15,16 Programs were classified according to 13 system functions that were ultimately arrived upon by the research staff and advisory council. The 13 functions were systems organization and service integration, systems monitoring and accountability, research/knowledge management/system innovation, funding/finance/resource allocation, law and policy, advocacy and mobilization, professional education and workforce development, physical infrastructure development, communication and information dissemination, consumer education, preventative care, treatment and intervention, and food and beverage provision.
Programs were also classified by the research staff and advisory council based on their system function as it relates to one or more of three different community health dimensions of the socioecological system (Fig. 1). 17 “Formal Structure and Systems” refers to programs that develop or enforce laws, rules, or other structural elements of the system; “Social and Physical Environment Infrastructure” refers to programs that create, influence, or shape the social, physical, or structural environment; and, “Transmission of Behavior and Practice” includes programs that have an impact on individuals' behaviors (e.g., peers, family members, and professionals).
Lastly, organizations were classified by the research staff according to their system function based on the collective impact framework 18 with the goal of identifying coordinating or “backbone” support. These system support functions are system monitoring and accountability; advocacy and mobilization; communication and information dissemination; funding, finance, and resource allocation; and research and knowledge management.
Results
The characterization process identified 260 programs provided by 89 organizations, with most organizations administering multiple programs. Most organizations (65%) had budgets of >$2.5 million per year. Nonprofit organizations (56%) and government (34%) were the most common organization type. Nonprofit organizations tended to address a smaller geographic scope, and 30% reported annual budgets <$500,000.
The largest number of programs served school-aged children (n = 169 [65.0%]), with nearly all operating at the city/municipality geographic level (e.g., public school services; Table 1). Many programs' client focus targeted expecting mothers (82 [31.5%]) and their families (118 [45.4%]). The most common geographic scale of programs for each population group was the city/municipal level. A relatively large share of programs also had a client focus of targeting low-income populations, although programs for school-aged children spanned all income categories. There were relatively few programs that had a client focus of targeting any specific racial or ethnic population.
Geographic Scope, Income, and Racial/Ethnic Focus of Programs by Client Type
The total number of programs listed in this table vary by column as many programs operate in more than one geographic category, racial/ethnic focus, or client type or a response could not be properly categorized.
The greatest share of programs targeted the social and physical environment (195 [75.0%]) dimension of the socioecological model/community health system, followed by individual behaviors and practices (164 [63.0%]) and formal structures (110 [42.3%]) (Table 2; Fig. 2). The distribution of program function within each socioecological dimension varied, with those addressing formal structures being more likely to serve the functions of system organization (17 [6.7%]), funding (46 [18%]), and law and policy (12 [4.7%]); those addressing social and physical environments being more likely to serve the functions of food/beverage services (24 [9.4%]), professional education (32 [12.5%]), and infrastructure (17[6.7%]); and those addressing individual behavior and practices are more likely to serve the functions of consumer education (141 [55.3%]) and disseminating information (66 [25.9%]). Lastly, no single organization was identified as providing all six system functions typically performed by a “backbone” organization (per the collective impact framework); two provided five of six functions, two additional organizations provided four of six functions.
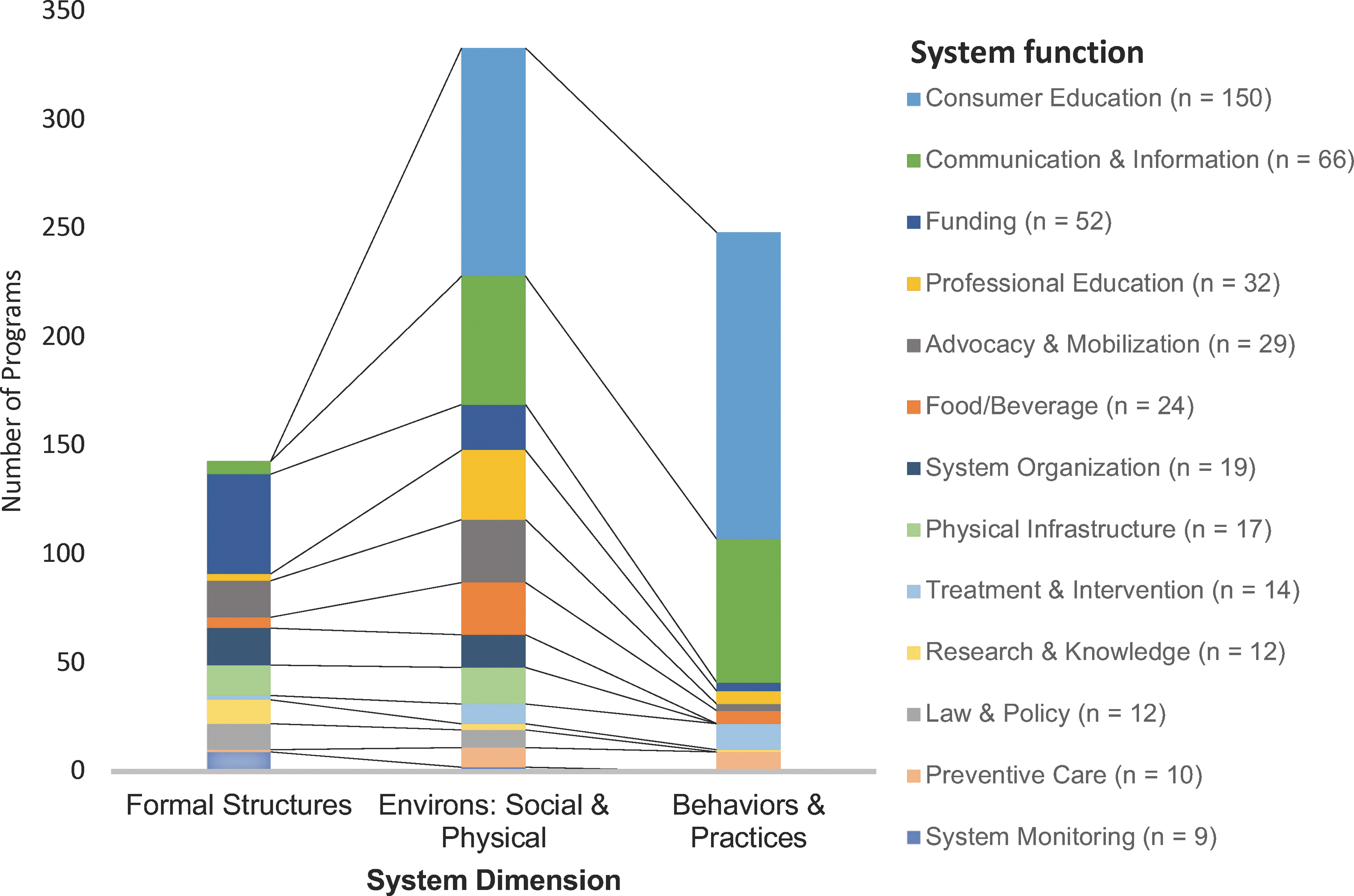
Frequency of Kansas City-based obesity prevention programs organized by community health system dimension and function. Color image is available online.
Kansas City-Based Obesity Prevention Programs by System Function and Dimension
The number of programs listed in each row or column exceeds the actual total because most programs operate in more than one system dimension.
Discussion
The systems characterization project described here suggests that Kansas City has a robust naturally occurring system in place for addressing the challenges and issues of childhood obesity, although there are opportunities for improvement. We observed that the region has a large number of programs working within the system, yet the distribution of programs does not occur as expected throughout the dimensions of a standard socioecological model/community health system. Specifically, we observed the largest number of programs targeting the social and physical environment socioecological dimension, when it would be expected that the largest number would be focused on individual behaviors and practices given large amount of resources needed to target individuals. 19 This suggests that there may be duplication of efforts and opportunities for collaboration between organizations. In addition, although there is a large number of programs targeting every dimension of the socioecological model/community health system, there is no true unifying organization that performs traditional “backbone” functions, potentially limiting the impact on childhood obesity due to lack of coordinated efforts between the organizations. These findings hold many public health implications for the organizations working to address childhood obesity in the Kansas City region.
Most childhood obesity programs in the region serve all eligible individuals who are within the general geographic scope of their organization, without a specific income or racial/ethnic target population. The finding that many programs served low-income populations is promising due to the high need of those populations, but that few programs focused on racial/ethnic minority groups are noteworthy considering the diverse demographic constitution of the city (40.8% of the population is nonwhite). This raises concerns about equitable access given that minority children experience obesity at a higher than other children and may be ideal targets for obesity prevention efforts. 20
When examined from the perspective of a socioecological model/community health system, the programs addressing childhood obesity treatment and prevention system in the Kansas City region are not distributed across levels/dimensions as often described theoretically (Fig. 2).1,19 Traditional socioecological models of health behavior describe a framework consisting of multiple levels of influences, with individual or interpersonal focused activities or interventions such as counseling or education as being resource intense (i.e., large number of programs delivering one-on-one educational services) and limited population impact. Conversely, programs targeting policy or the environment will have a large population-level influence, yet may be fewer in number given they are directed toward policy makers (i.e., a single program advocating city council for Complete Streets policy). In the Kansas City region, we identified the largest number of programs targeting the social and physical environment as opposed to behaviors and practices as would be expected based on traditional models. As previously described, the childhood obesity system is naturally occurring so it is likely that this distribution of programs occurred organically to meet the specific needs of the region. Given that Kansas City is historically one of the most segregated cities in the United States (11th in 2000 according to the Brookings Institute) while at the same time has low density and is incredibly vehicle dependent (the highest freeway miles per capita in the United States), there is likely a high need for programming related to the social and physical environment. However, given the disproportionately high number of programs targeting this ecological dimension, there may be duplication of efforts and opportunities for collaboration between organizations.
Four organizations providing programs fulfilled certain “backbone” organization functions in the region, but no single entity performed all functions. An effective backbone organization typically provides strategic direction, facilitates dialogue between partners, coordinates data collection and analysis, ensures effective stakeholder communications, coordinates community outreach, and mobilizes funding. The four organizations performing some of these functions in Kansas City are quite diverse in their structure and include a regional quasi-governmental planning council, a hospital-based regional childhood obesity coalition, a regional advocacy-based nonprofit focused on childhood healthy eating/active living, and a regional maternal, infant, and family health-focused coalition. This diversity provides opportunities to improve collaboration across the system and better use finite resources to enhance collective impact to increase the proportion of children at a healthy weight. Key to this collaboration is interorganizational coordination among these quasi-backbone organizations that aim to support and connect the entire system. There also may be value in the creating of a more formal backbone organization or oversight body with representatives from these organizations. If established, this oversight could lead to identification of key data still needed and collective planning on how the system could more effectively address obesity.
The collective impact approach offers a framework useful for organizing and guiding the mobilization of a myriad of community programs and initiatives that help address a shared goal. 18 This approach highlights the need for structure, coordination, and integration rather than isolation among community organizations. In addition, this approach articulates the importance of a “backbone” entity to facilitate the collective change process. 21 These functions may be shared across organizations, if one organization that serves all of these functions does not exist. Importantly, building on existing structures and engaging the naturally occurring system are necessary. This suggests that identifying the naturally occurring system and identifying potential system leaders are crucial initial steps in mobilizing organizations to achieve in community-wide change.
Other projects have used similar information to build partnerships among members of the pre-existing system. An Australian initiative identified diverse members of the obesity prevention network and used this information to create a public searchable database for members to identify cross-sector partners. 22 Cardazone, Sy, Chik, and Corlew also used naturally occurring system information related to the existing child abuse and neglect prevention system in Hawaii. 23 A social network analysis was conducted to depict and analyze the degree of connectedness among partners with the intention of identifying areas where developing coalitions would be beneficial to existing partners.
There are several noteworthy limitations to this project. First, the data collected were descriptive and not adequate to examine the effectiveness of the system in terms of program reach or if they had a positive impact on recipients' health. In addition, this study did not collect information regarding existing communication networks among system members. This information would have been helpful in characterizing the existing coordination within the naturally occurring Kansas City system. Also, it is unclear the extent that the characteristics of the programs described here are aligned with the needs of the region. As with many regions, external funding typically dictates organizational programming, and it is not clear the extent program characteristics are driven by funders, the organizations in which they reside, or the specific needs of the region. Lastly, level of collaboration between organizations and project was not assessed, which limits the understanding of coordination particularly among the four organizations that serve “backbone” organization functions.
This project demonstrates a process that can be used in other regions to identify the systems involved in a variety of health behaviors and treatments. Future research is needed to understand additional system metrics such as effectiveness, depth, and adequacy of programs and organizations. As evidence builds on effective interventions, the insights gathered from this system characterization project will enable organizations to identify opportunities to improve the reach of programming and improve health equity. In addition, attention should be focused on best approaches to improving collective impact given insights into current organizations that fulfill leadership functions. Defining leadership and collective next steps will facilitate a more cohesive network of services in this region.
Footnotes
Acknowledgments
The authors wish to thank the Community Advisory Committee and the Midwest Center for Nonprofit Leadership.
Funding Information
This work was funded by an unrestricted grant from the Health Forward Foundation (previously the Healthcare Foundation of Greater Kansas City).
Author Disclosure Statement
The authors have no disclosures to report.