
Abstract
Background:
Positive neighborhood environments may promote healthier behaviors, yet few studies have examined associations between neighborhood social environment and diet. We examined associations of neighborhood perceived safety, collective efficacy, and violent crime with dietary intake among preschool-aged children and their mothers.
Methods:
We administered a cross-sectional survey to 300 mothers/female caregivers of Medicaid-enrolled 2- to 4-year-old children in Philadelphia. Mothers reported their own and their child's dietary intake using the validated Dietary Screener Questionnaire. Mixed-effects linear regression models assessed associations of perceived neighborhood safety, collective efficacy, and census tract-level violent crime with parent and child dietary intake, adjusted for individual, family, and neighborhood covariates.
Results:
Among mothers, higher perceived neighborhood safety and collective efficacy were associated with higher daily intake of fruits/vegetables (β = 0.35 cups, 95% CI: 0.12–0.58 and β = 0.30 cups, 95% CI: 0.08–0.52, comparing the highest with lowest tertile). Higher neighborhood-perceived safety was also associated with higher whole-grain intake among mothers (β = 0.14 ounces, 95% CI: 0.02–0.27) and children (β = 0.07 ounces, 95% CI: 0.01–0.13, comparing the highest with lowest tertile). Neighborhood social exposures were not associated with intake of added sugars or sugar-sweetened beverages for mothers or children, nor were lower levels of violent crime associated with any outcome.
Conclusions:
More favorable perceptions of neighborhood safety and collective efficacy were associated with a slightly higher consumption of some healthy foods among mothers and their young children. Future prospective research is needed to confirm these findings, explore potential mechanisms, and determine whether intervening on the social environment improves diet.
Introduction
In the United States, many children have suboptimal dietary patterns that do not meet national guidelines. 1 Parents play a key role in establishing young children's dietary patterns through feeding practices, food purchasing decisions, and modeling dietary habits. 2 Parental stress may also impact child diet, as demonstrated by past studies reporting associations between higher parental stress and unhealthy food-related parenting practices,3,4 poorer child dietary quality, 5 and greater fast-food consumption among children. 3
The socioecological model offers insights into how factors at multiple levels influence diet. 6 Parent and child dietary patterns are influenced by individual characteristics and by characteristics at the family level (e.g., family socioeconomic status [SES] 7 ) and the neighborhood level, including neighborhood SES, 8 availability of healthy vs. unhealthy food retail outlets, 9 and the neighborhood social environment. 10 The neighborhood social environment is composed of social interactions and processes, such as the relationships between residents (e.g., collective efficacy 11 ) and social stressors (e.g., crime, perceptions of safety, disorder 12 ).
Neighborhood collective efficacy is a construct that incorporates both social cohesion (trust and willingness to help between neighbors) and informal social control (willingness to intervene to maintain public order). 11 Collective efficacy might impact dietary intake through increasing social support,13,14 which could help to support families in accessing healthy foods and maintaining healthier diets. Higher neighborhood collective efficacy may also buffer the adverse effects of stress among mothers,15,16 which could help to support healthier behaviors and parenting practices. In contrast, neighborhood social stressors such as crime may increase maternal stress. 17 This might increase mothers' own stress-related consumption of unhealthy foods 18 and make it more challenging to implement healthy food-related parenting practices.3,4
Although neighborhood safety, crime, and collective efficacy have been found to be associated with obesity among both children and adults in some studies, 10 few studies to date have examined their associations with diet. Our objective was to determine the association of neighborhood safety, collective efficacy, and crime with dietary outcomes among Medicaid-enrolled preschool-aged children and their primary female caregivers. We hypothesized that parents and children living in a neighborhood with (1) greater perceived safety, (2) greater collective efficacy, and (3) lower violent crime rates would have better dietary outcomes compared with parents and children in neighborhoods with more adverse social environments.
Methods
Study Population
We enrolled a convenience sample of 300 mothers/female caregivers of Medicaid-enrolled 2- to 4-year-old children in Philadelphia. We restricted enrollment to mothers/female caregivers because neighborhood social perceptions may differ by gender, 19 and to Medicaid-enrolled families (public health insurance for people with low incomes) to enroll a primarily lower income population. Mothers were enrolled between October 30, 2019, and August 26, 2020, through the Children's Hospital of Philadelphia (CHOP) Pediatric Research Consortium (PeRC) primary care research network 20 and Recruitment Enhancement Core (REC).
Mothers were initially enrolled in-person at their child's primary care visit using electronic health record (EHR)-based rosters of scheduled visits at two urban clinics. At the start of the COVID-19 pandemic, we switched to a remote process. The REC e-mailed invitations to potentially eligible participants based on lists of contact information pulled from the EHR to identify parents of patients aged 2–4 years who lived in Philadelphia zip codes. Eligible caregivers were the mother/female legal guardian of a 2- to 4-year-old child, English-speaking, ≥18 years old, and lived within the city of Philadelphia.
We administered a survey on dietary intake, neighborhood perceptions, and sociodemographic characteristics. The survey was pilot tested for length and comprehension in the target population before data collection and revised based on feedback elicited from families after completion. The CHOP Institutional Review Board approved this study. All participants provided written informed consent and received $25 as compensation.
Dietary Intake
The primary outcomes were maternal and child dietary intake, assessed by mothers' report using the Dietary Screener Questionnaire (DSQ) from the National Health and Nutrition Examination Survey (NHANES) 2009–2010.21,22 The DSQ is a 26-item screener that assesses consumption in the past month of foods and beverages selected for their relevance to key dietary categories (e.g., fruits/vegetables, added sugars, whole grains). The DSQ has been validated against 24-hour dietary recalls in adults and children aged ≥2 years.21,23,24 We selected the DSQ for its rigorous development, inclusion of dietary factors relevant to obesity risk, and feasibility of use with both adults and children.
Neighborhood Social Environment
We examined three neighborhood social environment exposures: perceived safety, collective efficacy, and crime. Perceived neighborhood safety was assessed using 2 items that have good test/retest reliability in urban populations (Supplementary Table S1).25,26 Perceived neighborhood collective efficacy was assessed using the Collective Efficacy Scale developed by Sampson et al. 11 in the Project on Human Development in Chicago Neighborhoods study, which has been used in prior studies on obesity.27–29 The measure includes 5 items related to social cohesion and 5 items related to informal social control (Supplementary Table S1). Items for both measures were assessed using 5-point Likert scales and averaged to create summary scores.
Participant home addresses were geocoded to enable linkage of objective neighborhood violent crime rates. Violent crime rates within each participant's residential census tract were calculated using publicly available data from the Philadelphia police department 30 and reflected the total number of violent crimes (homicide, assaults, robberies, sex offenses) in 2019 per 1000 residents. Violent crime rates were mapped with participant addresses (randomly jittered to ensure confidentiality) overlaid to demonstrate participant spread across Philadelphia. Neighborhood social environment measures were categorized into tertiles for ease of interpretation, to enable us to compare neighborhoods with low, medium, and high levels of each exposure, and due to evidence of nonlinear relationships with dietary outcomes.
Covariates
Covariates included potential confounders a priori hypothesized to relate to diet and neighborhood social exposures. We selected covariates at the individual-, family-, and neighborhood-level based on a socioecological framework 6 (Fig. 1). Details on how these measures were categorized for analysis are presented in Table 1. Maternal covariates included self-reported age, race/ethnicity, country of birth, marital status, education, and employment. Child covariates included age, sex, and day care attendance. Family-level covariates included household income, receipt of Supplemental Nutrition Assistance Program and Special Supplemental Nutrition Program for Women, Infants, and Children benefits, and household size.

Conceptual model of the relationship between neighborhood social environment exposures and dietary intake. Hypothesized mechanisms in the dashed box reflect potential mediators not included in the analysis. NEMS-P, Perceived Nutrition Environment Measures Survey; SSB, sugar-sweetened beverages; SNAP, Supplemental Nutrition Assistance Program; WIC, Women, Infants, and Children.
Characteristics of Study Population (n = 300)
Some percentages sum to less than 100% due to missing responses.
Range 1–5 on a Likert scale (1 = strongly disagree, 5 = strongly agree).
Range 1–14, created by summing 4 items scaled from 1 to 2 (mode of transportation) or 1 to 4 (travel time to food store, importance of store proximity to home or other places in decision-making).
Range 1–4 on a Likert scale (1 = not at all important, 4 = very important).
Range 1–4 on a Likert scale (1 = very expensive, 4 = very inexpensive).
Per 1000 census tract residents.
NEMS-P, Perceived Nutrition Environment Measures Survey; SNAP, Supplemental Nutrition Assistance Program; WIC, Women, Infants, and Children.
Neighborhood-level covariates included neighborhood poverty and food environment. Neighborhood poverty was assessed as the proportion of the census tract population with household incomes below the federal poverty line using 5-year estimates from the 2014–2018 American Communities Survey 31 and was included because neighborhood-level poverty may exert influences on diet independent of individual-level SES. 8 Finally, we used the Perceived Nutrition Environment Measures Survey (NEMS-P) to assess mothers' perceptions of their neighborhood food environment. 32 The NEMS-P included questions on food store access (4 items, score range 1–14), store availability of healthy food choices (6 items, score range 1–5), store motivation (3 items, score range 1–4), price of fruits/vegetables (1 item, score range 1–4), and placement/promotion of healthy and unhealthy food items (5 items, score range 1–5).
Statistical Analysis
Missing data were rare (Supplementary Table S2). However, a complete case analysis would have reduced our total sample size by 15%, and so, we used multiple imputation with chained equations to impute missing data. 33 Scoring algorithms from the National Cancer Institute were used to convert DSQ responses to estimated daily intake of fruits/vegetables, whole grains, total added sugars, and sugars from sugar-sweetened beverages (SSB) for mothers and their children. Spearman correlation coefficients were used to calculate correlations between parent and child intake, and between the neighborhood social environment measures.
There was some evidence of clustering of dietary outcomes by census tract (highest intraclass correlation coefficient: 0.06), and so, mixed-effects linear regression was used to estimate associations of each neighborhood social measure—perceived safety, collective efficacy, and crime—with mother and child dietary intake. Each dietary outcome was modeled separately for mothers and children. Models included census tract random intercepts to account for lack of independence between participants living in the same neighborhood.
We ran separate models for each neighborhood social environment exposure, because these exposures might have mediating or bidirectional relationships (e.g., collective efficacy might influence crime rates and perceived safety, 11 while safety might in turn influence perceptions of collective efficacy), and the cross-sectional design limits our ability to fully explore these pathways. Models were progressively adjusted for covariates as follows: unadjusted (Model 1), adjusted for demographics and family SES (Model 2); further adjusted for neighborhood poverty (Model 3); and finally, further adjusted for perceived neighborhood food environment (NEMS-P, Model 4).
The NEMS-P measures were conceived as potential mediators between the neighborhood social environment and dietary intake, but due to the cross-sectional design of our study, we cannot determine temporality of relationships between these variables. We examined Spearman correlation coefficients and variance inflation coefficients to check for collinearity.
To determine whether findings were robust to a different neighborhood specification, we conducted a sensitivity analysis using census block groups to define neighborhoods. Statistical analysis was performed using R version 3.6.1, STATA version 16, and ArcGIS version 10.5.1. Study hypotheses and the analytic plan were prespecified before data collection.
Results
Study Population
Of the 756 parents approached, 153 did not meet the eligibility criteria and 184 did not complete the screening process. Among the remaining 419 parents, 300 were enrolled for a 72% response rate. Of the remainder, 11 refused and 108 started, but did not complete, the survey.
Mothers who enrolled were 60% Black/African American, with a mean age of 31 years (Table 1). Mothers were primarily born in the United States (94%), never married (53%), and had some college or an associate's degree (40%). Children had a mean age of 3.8 years and 56% were male. Income varied, but the largest proportion reported a household income of $25,000 to $49,000 (39%). Mothers who refused or did not finish the survey were younger on average, more likely to report non-Hispanic black or Hispanic/Latina race/ethnicity, less likely to be married, and reported lower educational attainment and income.
Mothers' mean scores on the perceived neighborhood safety and collective efficacy scale were both 3 (on a scale ranging from 1 to 5, with higher numbers indicating more favorable neighborhood perceptions). Participants lived in 192 census tracts (Fig. 2, range 1–6 participants per tract). Census tract-level violent crime rates ranged from 0 to 126.8 crimes per 1000 residents among women in the study, lower than the maximum violent crime rate for Philadelphia as a whole (250 violent crimes per 1000 residents). 30 Neighborhood social environment measures were moderately correlated, with Spearman correlation coefficients of 0.66 between perceived safety and collective efficacy, −0.33 between perceived safety and violent crime rate, and −0.25 between collective efficacy and violent crime rate (all p < 0.001).
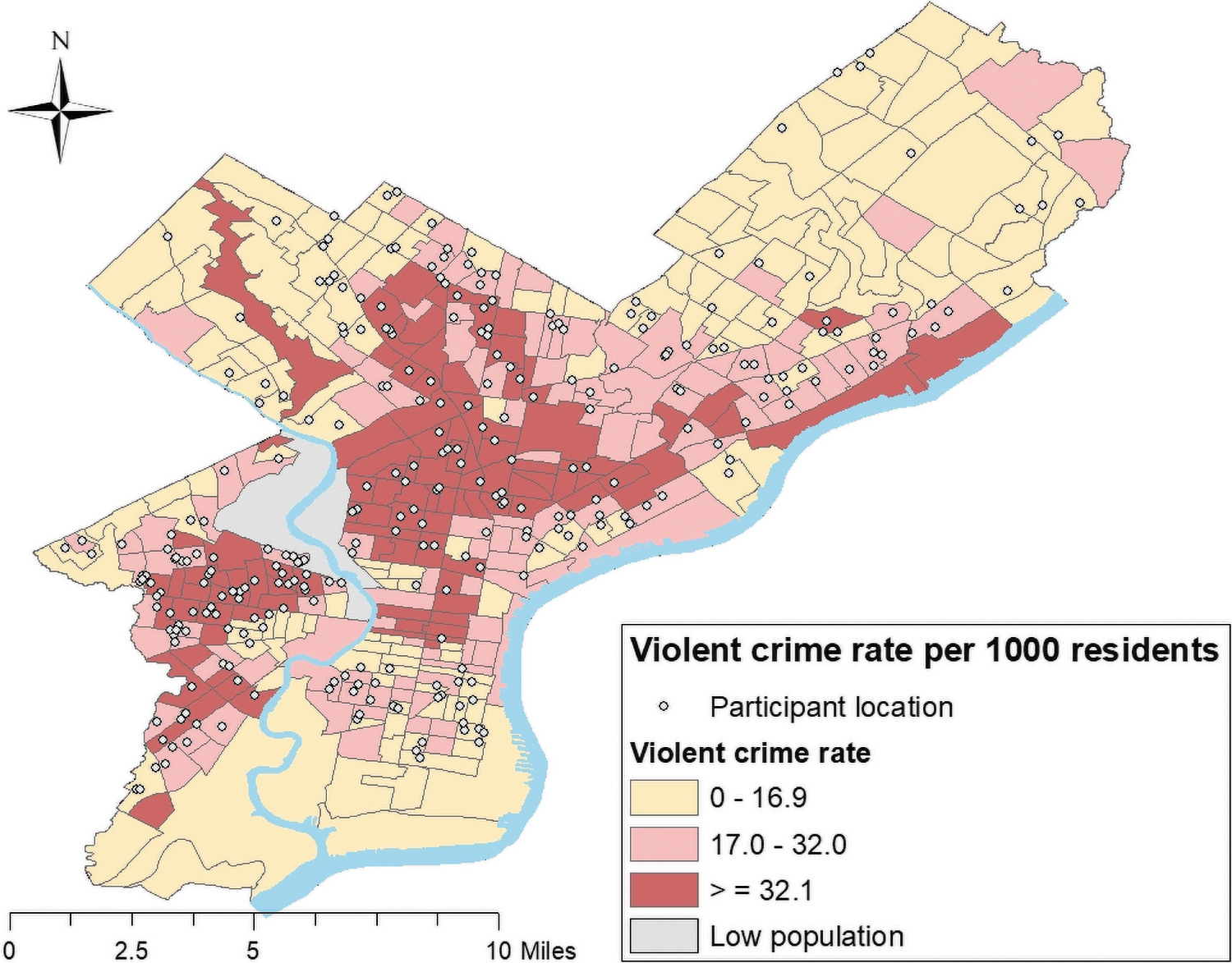
Participant spread and neighborhood violent crime rates across Philadelphia. Tertiles were based on our study cohort rather than the full set of census tracts in Philadelphia. Data reflect crime incidents from January to December of 2019 retrieved from the city of Philadelphia's open data portal. Violent crimes included homicides, assaults, robberies, and sex offenses. Participant point locations were enlarged and randomly jittered to ensure confidentiality. Color image is available online.
Dietary Intake
Parents reported consuming an average of 2.6 cups of fruits/vegetables, 0.8 ounces of whole grains, and 17.2 teaspoons of total added sugars, including 8.5 teaspoons of sugars from SSB per day (Table 2). Parents reported their child consuming an average of 2.0 cups of fruits/vegetables, 0.5 ounces of whole grains, and 14.4 teaspoons of total added sugars, including 4.7 teaspoons of sugars from SSB per day.
Parent and Child Dietary Intake
Dietary intake was calculated using scoring algorithms from the National Cancer Institute that convert Dietary Screener Questionnaire responses to estimated daily intake in cup, ounce, or teaspoon equivalents. Recommended daily intake values for adult females aged 19–59 years are as follows: fruits/vegetables: 3.5 to 5 cups, whole grains: 3 to 4 ounces. Recommended daily intake values for children aged 2–4 years are as follows: fruits/vegetables: 2 to 3.5 cups, whole grains: 1.5 to 3 ounces. Added sugars are recommended not to exceed 10% of total energy intake.
Spearman correlation coefficients.
National recommended daily intakes among adult females and children aged 2–4 years are as follows: fruits/vegetables: 3.5–5 cups for adults, 2–3.5 cups for children; whole grains: 3–4 ounces for adults, 1.5–3 ounces for children; added sugar: limited to less than 10% of daily energy intake; SSB: not recommended. 34 Parent and child dietary quality was moderately correlated, with Spearman correlation coefficients of 0.49 for fruit/vegetable intake, 0.47 for whole-grain intake, 0.50 for total added sugar intake, and 0.37 for sugar from SSB intake.
Associations of Neighborhood Social Environment with Parent Dietary Intake
Associations between neighborhood social environment measures and mothers' dietary intake are presented in Figure 3 (model 3; adjusted for demographics, family SES, and neighborhood poverty) and Supplementary Table S3 (all models). In model 3, run separately for each neighborhood social environment exposure, higher perceived neighborhood collective efficacy was associated with higher daily intake of fruits/vegetables for mothers (Fig. 3; β = 0.30 cups, 95% CI: 0.08–0.52 comparing the highest with lowest tertile).

Association of neighborhood social environment with parent dietary intake. Dietary intake was calculated using scoring algorithms from the National Cancer Institute that convert screener responses to estimated daily intake in cup, ounce, or teaspoon equivalents. Coefficients in the figure reflect the estimated mean difference in daily intake between tertiles of neighborhood social environment from mixed-effects linear regression models. Models were adjusted for maternal age, race/ethnicity, nativity, education, employment, marital status; household income, household size, receipt of SNAP or WIC; neighborhood poverty. Separate models were run for each neighborhood social environment exposure. Neighborhood social environment exposures were categorized into tertiles: perceived safety: tertile 1: 1–2; tertile 2: 2.5–3.5; tertile 3: 4–5; collective efficacy: tertile 1: 1–2.7; tertile 2: 2.8–3.4; tertile 3: 3.5–5; violent crime: tertile 1: 0–16.9; tertile 2: 17.0–32.0; tertile 3: 32.1–126.8. SNAP, Supplemental Nutrition Assistance Program; WIC, Women, Infants, and Children. Color image is available online.
Higher perceived neighborhood safety was also associated with higher daily intake of fruits/vegetables (β = 0.35 cups, 95% CI: 0.12–0.58 comparing the highest with lowest tertile). Higher perceived neighborhood safety was associated with higher intake of whole grains (β = 0.14 ounces, 95% CI: 0.02–0.27 comparing the highest with lowest tertile), while lower police-recorded violent crime rate was not associated with intake of fruits/vegetables or whole grains. None of the neighborhood social exposures examined in this study was associated with intake of total added sugars or SSB for mothers in adjusted models. Results were similar in a sensitivity analysis that used census block groups to define neighborhoods (Supplementary Table S5). In analyses that additionally adjusted for the NEMS-P, associations of perceived safety and collective efficacy with maternal fruit/vegetable intake were substantively similar but slightly attenuated (Supplementary Table S3).
Associations of Neighborhood Social Environment with Child Dietary Intake
Associations between neighborhood social environment measures and child dietary intake are presented in Figure 4 (model 3; adjusted for demographics, family SES, and neighborhood poverty) and Supplementary Table S4 (all models). Among children, higher maternal-perceived neighborhood safety was associated with higher intake of whole grains in model 3 (β = 0.07 ounces, 95% CI: 0.01–0.13 comparing the highest with lowest tertile). Neighborhood social exposures were not associated with intake of fruits/vegetables in any models for children, or with added sugars or SSB in adjusted models. Results were similar in a sensitivity analysis using block group as the neighborhood unit (Supplementary Table S6) and after adjustment for the perceived neighborhood food environment measures (Supplementary Table S4).

Association of neighborhood social environment with child dietary intake. Dietary intake was calculated using scoring algorithms from the National Cancer Institute that convert screener responses to estimated daily intake in cup, ounce, or teaspoon equivalents. Coefficients in the figure reflect the estimated mean difference in daily intake between tertiles of neighborhood social environment from mixed-effects linear regression models. Models were adjusted for child age, sex, day care attendance; maternal age, race/ethnicity, nativity, education, employment, marital status; household income, household size, receipt of SNAP or WIC; neighborhood poverty. Separate models were run for each neighborhood social environment exposure. Neighborhood social environment exposures were categorized into tertiles: perceived safety: tertile 1: 1–2; tertile 2: 2.5–3.5; tertile 3: 4–5; collective efficacy: tertile 1: 1–2.7; tertile 2: 2.8–3.4; tertile 3: 3.5–5; violent crime: tertile 1: 0–16.9; tertile 2: 17.0–32.0; tertile 3: 32.1–126.8. The model examining safety and sugars from SSBs did not converge. Color image is available online.
Discussion
Overall, greater perceived neighborhood safety and collective efficacy were associated with higher fruit/vegetable consumption among mothers, but not children, while greater perceived neighborhood safety was associated with higher whole wheat consumption among both mothers and children. Neither perceived safety nor collective efficacy was associated with differences in consumption of added sugars for mothers or children. Police-recorded violent crime rates were not associated with any dietary outcome. The mean intakes of fruits/vegetables and whole grains reported in our study were lower than the national guidelines recommendation, 34 or at the bottom of the recommended range for child fruit/vegetable consumption.
Few studies have investigated the role of neighborhood safety, crime, and collective efficacy in diet compared with a larger literature on the neighborhood food environment, 9 although more studies have examined these neighborhood social exposures in relation to physical activity. 35 Our findings among mothers align with two prior cross-sectional studies among Philadelphia adults.27,36 Higher neighborhood collective efficacy was associated with higher odds of meeting guidelines for fruit consumption, and to a lesser extent, vegetable consumption, among a community-based sample of African American adults, 27 while higher neighborhood social capital (but not objectively measured crime) was associated with higher odds of meeting fruit/vegetable guidelines in the 2010 Southeastern Pennsylvania Household Health Survey. 36 Similarly, among adult residents of subsidized housing in Rhode Island, greater neighborhood social support for fruit/vegetable consumption was associated with higher fruit/vegetable intake. 37 A potential mechanism through which neighborhood collective efficacy might influence fruit/vegetable consumption is through increasing social support among neighbors,13,14 which could support healthier dietary patterns. It is also possible that residents of neighborhoods with high collective efficacy might have a greater ability to advocate for healthier neighborhood resources, such as farmers' markets, and help each other access food resources.
We hypothesized that lower neighborhood crime and higher perceived safety would be associated with lower consumption of added sugars and SSBs through stress-related consumption patterns. Our findings do not support this hypothesis, but we did not examine intake of other unhealthy foods/nutrients (e.g., snacks, saturated fat) due to limitations in our dietary measure. It may be that neighborhood safety is more relevant for other unhealthy foods. Consistent with this idea, a past cross-sectional study among women aged 18–44 years in Chicago reported that higher police-recorded crime rates were associated with greater consumption of unhealthy snacks, but not with higher SSB consumption. 38 Our finding that higher perceived safety was associated with higher fruit/vegetable and whole wheat consumption provides some support for the idea that neighborhood safety may increase healthy food consumption. It is possible that mothers who perceive their neighborhood as safer may feel more comfortable traveling throughout the neighborhood to seek out healthier food options.
Our findings for young children were less suggestive of an association between the neighborhood social environment and diet, and add to a very small literature on this topic. In prior studies of school-aged children, stronger neighborhood social ties (but not perceived safety or crime) were associated with both greater healthy and unhealthy eating patterns, 39 while higher neighborhood disorder was associated with small increases in energy, sodium, and iron intake and decreases in potassium intake. 40 However, we found no studies examining associations of neighborhood safety, crime, or collective efficacy with diet among preschool-aged children. Two studies that examined neighborhood crime or safety in relation to obesity in this age group found no association.41,42 Our finding that greater maternal-perceived safety was associated with small increases in whole wheat consumption, but not with other dietary patterns, is consistent with the relatively weak evidence available from prior studies.
We hypothesized that a more favorable neighborhood social environment would be associated with healthier dietary patterns intergenerationally, among both parents and children. This hypothesis was based on prior findings that parent and child diets are correlated43,44 and that parental stress may negatively impact child dietary patterns and healthy food-related parenting practices.3–5 While the moderate correlations between parent and child diet seen in our study are comparable with other studies,43,44 our results do not provide strong support for intergenerational associations of the social environment with diet for preschool-aged children. It may be that for this age group, the external environment beyond the home does not play a large role in food choice. Also, mothers may have greater ability to insulate their young children from the effects of neighborhood stressors in early childhood compared with later childhood and adolescence. The associations seen among mothers in our study (and among older children in prior studies39,40) suggest that the neighborhood environment may become more important with age, although longitudinal work is needed to confirm these patterns.
Strengths of our study include the diverse study population and the examination of both objective and subjective measures of the neighborhood social environment. However, our study was also subject to several limitations. First, the cross-sectional design limits causal inference. Future longitudinal and experimental work is needed to examine the generalizability of these findings, identify potential mediating pathways, and determine the potential effect of improvements to the neighborhood social environment on diet. Second, while we enrolled a diverse population of families dispersed throughout a wide range of neighborhoods, the use of a convenience sample in one city may limit generalizability. Third, the relatively modest sample size may have limited power to detect smaller associations. Fourth, we relied on mothers' report of parent and child dietary intake based on a screener rather than 24-hour dietary recall, which may have led to recall bias, or to same-source bias when examining associations with self-reported neighborhood perceptions. Fifth, although we adjusted for a variety of individual, family, and neighborhood confounders, we cannot rule out that findings might be explained by residual confounding due to unmeasured variables. Sixth, our data collection period overlapped with the COVID-19 pandemic, which may have impacted our findings due to changes in the food environment and dietary patterns (e.g., increased food insecurity, increased use of food delivery services, provision of food via community organizations and food pantries). Since fewer than 10% (n = 21) of participants were enrolled before the start of the pandemic, we were unable to examine whether associations differed between the prepandemic and pandemic periods. Seventh, although we examined sensitivity to alternative neighborhood definitions (census tracts, block groups), using administrative boundaries to define neighborhoods has limitations—for example, these boundaries may not align with participants' own definition of their neighborhood. Finally, our study focused on mothers only. Future work should incorporate the perspectives of fathers as well.
Conclusion
Greater perceptions of neighborhood safety and collective efficacy were associated with higher fruit and vegetable consumption among mothers of preschool-aged children in Philadelphia after adjustment for individual-, family-, and neighborhood-level covariates, while greater perceptions of neighborhood safety were associated with higher whole wheat consumption among both mothers and children. We found little evidence of association between the neighborhood social environment and consumption of added sugars or SSBs. Future work is needed to determine whether modifying the neighborhood social environment can improve dietary outcomes among mothers and young children.
Footnotes
Authors' Contributions
S.L.M. conceptualized and designed the study, designed the data collection instruments, coordinated and supervised data collection, drafted the data analysis plan, drafted the initial article, and reviewed and revised the article. C.H. recruited participants and collected data, carried out data analyses, drafted the initial article, and reviewed and revised the article. G.D. recruited participants and collected data, carried out data analyses, and reviewed and revised the article. S.V., K.G., and A.G.F. conceptualized and designed the study and critically reviewed the article for important intellectual content. All authors approved the final article as submitted and agreed to be accountable for all aspects of the work.
Acknowledgments
We want to thank the network of primary care clinicians, their patients, and families for their contribution to this project and clinical research facilitated through the Pediatric Research Consortium (PeRC) at the Children's Hospital of Philadelphia (CHOP). In addition, we thank Rupreet Anand and Ella LaBrusciano-Carris for their contributions to participant recruitment, and Rachel Gross for her advice on recruitment and data collection.
Data Availability
Due to privacy concerns and regulatory restrictions, the full data set will not be made openly available. An HIPAA-limited data set may be shared upon reasonable request to the corresponding author after execution of a data use agreement.
Funding Information
This work was supported by the Academic Pediatrics Association Nutrition Young Investigator Award (no award number) and the Children's Hospital of Philadelphia Possibilities Project (no award number). The study sponsors had no role in study design, collection, analysis, and interpretation of data, writing the article, or the decision to submit the article for publication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.