
Abstract
Different frameworks and models exist for translating and disseminating public health policies, programs, and services. This article describes an approach, grounded in the Integrate, DEsign, Assess, and Share (IDEAS) framework for digital health innovation and the Stanford Byers Center biodesign innovation process, to design a way to make effective behavioral weight control more scalable and cost-effective for low-income children with overweight and obesity, to reduce obesity and associated morbidities. The process considered the relevant stakeholders, the current market landscape, and the potential market. Solutions were designed to address provider training and resources, to have a strong foundation in behavior change methods, be sufficiently intense to produce change, involve both children and caregivers and be delivered in groups, to be less costly to deliver than current family-based behavioral programs, and to have a viable revenue model. An iterative process resulted in a potential solution that combines both technology and human affordances and addresses high fidelity delivery, needs of providers and patients, training and support, likely customers, potential revenue models, intellectual property, and regulatory issues.
Different frameworks and models exist for translating and disseminating public health policies, programs, and services. In the past, we have tried delivering our pediatric weight control program in multiple sites, training and supporting other providers, train-the-trainers for other organizations, and a multi-day, hands-on training institute. Although each showed promise, and led to some long-term successes, none produced the reach and sustainable growth we had hoped to achieve.
Thus, for several years the author set out to learn about scaling innovations from the Silicon Valley tech community. This included many meetings with tech founders, designers, managers, and marketers—from early-stage start-ups, to growing market leaders, to established corporate juggernauts, attending open houses and “meet-ups” for innovators and start-up founders, reading industry newsletters and blog posts and listening to podcasts about innovation and scaling, and collaborating on projects to develop tech-enabled interventions.
This process led to a one academic-year Stanford Byers Center for Biodesign faculty fellowship, created to provide faculty members from the Stanford schools of Medicine and Engineering with advanced training and mentoring in health technology innovation. a The cumulative impact of these fact-finding investigations and experiences, further informed by nearly three decades of designing, implementing and evaluating behavior change research interventions and clinical programs, and providing clinical care to prevent and reduce obesity in children, resulted in the following biodesign approach to packaging and scaling a pediatric weight management program. Thus, an approach, grounded in the IDEAS framework for digital health innovation 1 and the Stanford Byers Center biodesign innovation process, 2 was used to design a way to make effective behavioral weight control more scalable and cost-effective for low-income children with overweight and obesity, to reduce obesity and associated morbidities.
IDEAS: An Overall Framework for Digital Health Innovation
Figure 1 illustrates the IDEAS framework (Integrate, DEsign, Assess, and Share), created to help design more effective digital health behavior change innovations. 1 This framework goes beyond many other frameworks by integrating theory-based behavior change principles and practices into the process. It was an attempt to merge design thinking, b behavioral science, software development, rigorous evaluation, and dissemination strategies.

IDEAS is an iterative process with constant feedback loops, in a rapid cycle of iteration and innovation and testing. The IDEAS framework proposes four main tasks. Integrate insights from users and behavioral theory, empathize with target users, specify target behaviors, ground ideas in behavioral theory; Design iteratively and rapidly with user feedback, ideate implementation strategies, prototype potential products, gather user feedback, build minimum viable product; Assess rigorously, pilot potential efficacy and usability, evaluate efficacy in a randomized controlled trial; and Share the intervention and evaluation findings.
The Biodesign Innovation Process
The Stanford Byers Biodesign innovation process 2 is used most often in medical device innovation and complements the IDEAS framework. It puts more emphasis on preparing for the dissemination and commercialization stage of bringing an innovation to market, including anticipatory strategy development and business planning to address common challenges and commercialization routes available when introducing novel medical technologies (Fig. 2).
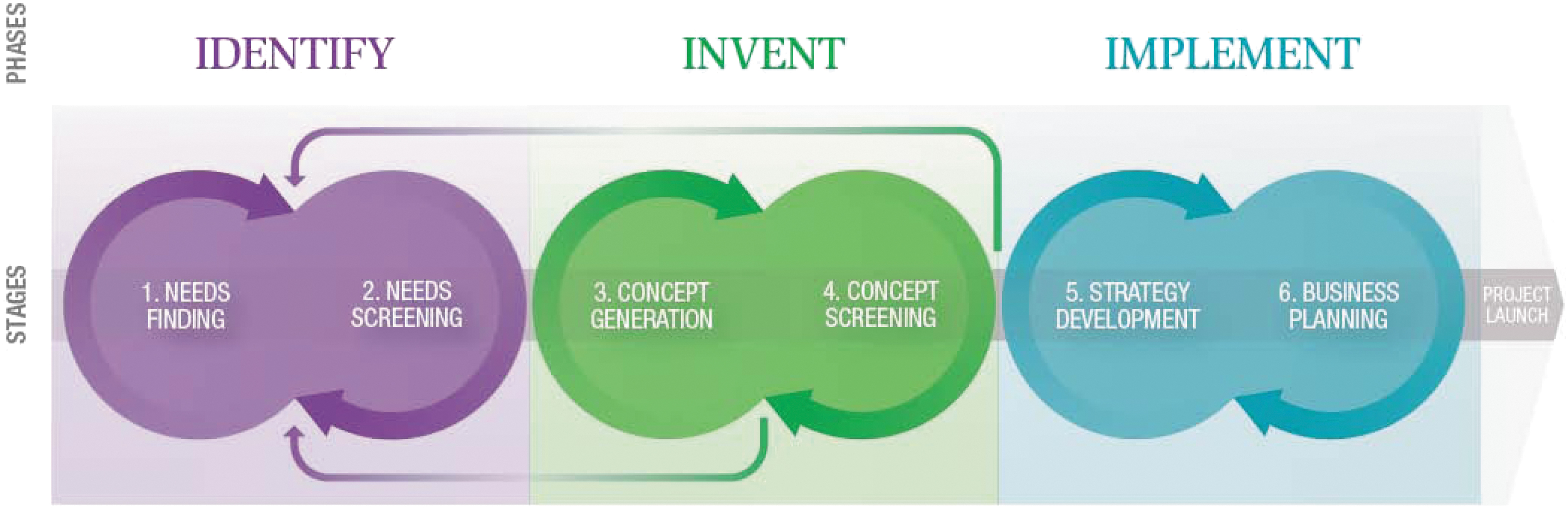
Biodesign also emphasizes a design thinking needs-driven approach that first identifies the needs of end users and other stakeholders and then designs to meet those needs. Through multiple iterative rounds of expanding and then trimming, empathizing, specifying, grounding ideas in theory, ideating (e.g., brainstorming), and rudimentary prototyping and gathering feedback, challenges and potential solutions are scoped according to a standardized biodesign innovation process.
The Need
One of the most important steps in the biodesign approach is the identification, revision, screening, and eventual selection of a needs statement. The rest of the innovation process builds off the needs statement. Need statements follow the general format of: a way to [observed problem] in [a defined population] to [outcome]. Tens to hundreds of candidate needs may be identified and examined through a need screening process before narrowing on a single need statement.
After months of investigation and iteration, the final needs statement for this project became, “A way to make effective behavioral weight control more scalable and cost-effective for low-income children with overweight and obesity, in order to reduce obesity and associated morbidities.” Key defining components of this need statement included specifying behavioral weight control, excluding devices, surgical procedures and medications, scalable and cost-effective, emphasizing potential for wide reach and effectiveness at a reasonable cost, low-income children who already are suffering from overweight or obesity, excluding primary prevention approaches and solutions that would only meet the needs of children from middle- and high-income families, and the outcome as reducing obesity and associated morbidities, emphasizing the importance of evidence of effectiveness on weight changes and obesity-associated metabolic, psychological and social morbidities. 3
The needs screening and scoping process involved gathering data to identify all the relevant stakeholders and their perspectives on the problem, examining the current market landscape to identify potential unfilled gaps and the competitive landscape (e.g., existing products, their efficacy, costs, and availability) and market segmentation to identify the size of the potential market for the problem.
The potential market includes the proportion of the population that could potentially benefit from the innovation. The CDC reported 4 that in 2017–2018 about 19.3% or 14.4 million 2- to 19-year old US children had obesity (BMI ≥95th percentile for age and gender on the 2000 CDC growth charts), including about 6.1% or 4.6 million children with severe obesity (defined as BMI ≥120% of the 95th percentile). By age, about 13.4% of 2- to 5-year olds, 20.3% of 6- to 11-year olds, and 21.2% of 12- to 19-year olds had obesity. In addition, about 16.1% or 12 million 2- to 19-year olds had overweight (BMI ≥85th and <95th percentiles).
An example of a market landscape analysis is illustrated in Figure 3. The goal is to identify gaps where existing approaches are not meeting needs. As shown, there is an available gap for a highly available approach with efficacy that compares with family-based group behavioral programs but at a significantly lower cost to implement.

Must-Haves
Must-haves are the criteria that a solution must meet to address the identified need. Based on the research literature, research into existing approaches, and nearly three decades of experience, four priority must-haves were identified. Not in order of importance, these include first, a solution must address the barrier of provider training and resources to allow a variety of providers to effectively implement the solution; second, it must have a strong foundation in behavior change principles, be sufficiently intense to produce behavior change, involve both children and caregivers, and be delivered in groups; third, it must be less costly to deliver than current family-based behavioral programs; and fourth, it must have a viable revenue model.
Potentially the most controversial of these must-haves is the second listed, the decision to specify intensive behavioral family-based groups as a necessary characteristic. Other models were considered as part of the scoping process, such as individual family treatments or direct use of technology with individual children or parents, or for creating distributed remote groups of families, parents, or children. All of these possible strategies, and others, may turn out to be effective solutions. However, the currently existing efficacy data,5–8 overwhelmingly favor the intensive family-based group behavioral treatment model. This combined with our own experience implementing individual family interventions, individual and group child-only interventions, and technology-mediated individual and group interventions, support the perceived importance of maintaining face-to-face groups of families including both children and their caregivers. Although others may have different experiences, we have found the structure of a group program, with multiple families meeting in a group in the same room, has many advantages for effectiveness. We believe it also promotes high levels of motivation, group rapport, role modeling, social support, participation, and attendance, as families notice when another family is missing and start to feel accountable to one another. We believe this is one of the most important design features of the Stanford Pediatric Weight Control Program (SPWCP) and many other family-based group behavioral treatments, accounting for some of their success.5–8
Insights
Initial brainstorming, including a wide variety of potential stakeholders, is uncensored and leads to a large number of possible ideas. Brainstormed ideas are then measured against the must-haves, and additional insights are collected to help focus initial ideation. Through our own experience of delivering care in many different clinical and community settings, observations and interviews of other providers and clinics treating children with overweight and obesity, and knowledge, past experience, research and exploration of the current reimbursement and technology landscape, several additional insights were identified that could be used to inform the design and initial prototyping.
For purposes of scaling an innovation, the providers are the primary “customers,” not the patients. We usually design for our patients and families. However, when the goal is reframed as scaling and spreading an efficacious intervention, other factors beyond the end-target patients and families will determine success or failure. After considering potential audiences to design for, it was posited that the major determinants of uptake and scaling will be provider organizations, institutions, and leadership, who will decide to adopt and implement the treatment and will need to find a way to pay for it. In this context, we focus on those gatekeepers who will make the decisions to adopt and implement the solution: health systems, hospitals, health plans, public health agencies, employers, youth, and family service providers (e.g., boys & girls clubs, parks and recreation departments, and schools). There may be reason to be somewhat optimistic about this audience because of recent trends for health systems and provider organizations to take greater responsibility for a population's health (e.g., Accountable Care Organizations [ACOs], staff model Health Maintenance Organizations [HMOs], and large employers).
n the specific design of the product it will also be important to address the needs of many other stakeholder groups, of course, including patients and families, possible frontline providers of the program and possible payers, as addressed hereunder, and other possible influencers (e.g., professional societies, government agencies and Non-Governmental Organizations [NGOs], the U.S. Preventive Services Task Force [USPSTF], academic researchers, patient advocacy groups, the food and sedentary behavior industries, and politicians).
Just copying successful adult program models is unlikely to meet our needs. Children are not just small adults. Existing program models (e.g., commercial weight loss programs for adults, meal replacement programs, gyms and trainers, and other members of the dieting industry) are not specifically designed to meet the complex lives and needs of growing and developing children and families, leaving an important opportunity without much direct competition.
Technology is a potential solution to help overcome some of the most daunting provider barriers to adoption and implementation, training, supportive resources, and costs. However, technology and software alone are not sufficient. Human touch is critical. This insight arose from qualitative experiences and observations of delivering clinical services, including the SPWCP. We observed that the frontline providers who will deliver the actual intervention content (e.g., health and mental health professionals, nutritionists/dietitians, exercise physiologists, physical trainers, paraprofessionals, layperson group leaders, and youth leaders) as well as participating families find the human touch components to be highly rewarding and critical in promoting intrinsic motivation to either implement or participate in a treatment program.
Traditional training focused on knowledge gain can be more of a barrier than a facilitator to adoption and implementation. Although this insight runs counter to practice for most dissemination strategies, it is based on many years of working with providers to implement clinic-, school-, and community-based interventions. Although many providers tell us they need and want more knowledge and training, many also report that setting aside the time required for training (and taking that time away from direct service delivery or other priorities) is a burden. Furthermore, it is unclear whether training can be as useful when not delivered in the context of implementation.A focus on limited training emphasizing modeling, enactive learning, rehearsal, and guided practice, such as guided role playing activities, teamed with just-in-time content, are likely to prove more effective at building positive outcome expectancies and efficacy expectancies among frontline providers. 9 Therefore, important content may be better delivered in a just-in-time manner during program delivery, when most relevant to providers, rather than front-loaded.
The Solution
Based on the results of the iterative scoping of needs, must-haves, and insights, a proposed solution was formulated for packaging and scaling an intensive family-based group behavioral weight control program for children with overweight and obesity. In stereotypical Silicon Valley “pitch” manner, we draw analogies to other industries and contexts to illustrate the solution: a combination of “a little bit of Airbnb, a lot of Salesforce, with a pinch of instant cake mix.”
“A little bit of Airbnb” because the solution will use technology to mobilize an existing but currently underutilized resource of interested providers and organizations to equip and empower them to provide the program as a new offering. Among other things, Airbnb used technology to help individuals turn their underutilized rooms and instincts for hospitality into new businesses. In our case, the many types of providers, both organizational and frontline described earlier, who would like to play a role in helping children with overweight and obesity but currently do not have the knowledge or resources to do so, can be helped to develop their own new “businesses.”
“A lot like Salesforce” because, similar to Salesforce's comprehensive customer relationship management software, technology may be used to develop an integrated comprehensive family-based group behavioral pediatric weight management package that includes (1) a turnkey software as a service (SaaS) platform to reduce barriers to entry, training, and implementation for providers; (2) logistics support to help providers obtain everything they need to implement the program, including process and outcomes data on all participants; (3) standardization to increase the fidelity of program delivery and promote program consistency and effectiveness; and (4) cloud-based delivery to greatly increase the ease and efficiency of updating content. In addition, a software industry-like subscription revenue model will be explored.
Finally, “a pinch of instant cake mix” to provide sufficient autonomy to providers. An oft-repeated consumer marketing story tells of the boost in instant cake mix sales only after dehydrated eggs were removed from the box, so cooks would have to add both eggs and water, making them feel like they were still baking and less guilty.
Experience suggests that providers also want to play a role in personalizing treatment to children and families. Providing a total technology-/software-driven program would eliminate provider autonomy, turning highly trained and effective communicators into technicians, and likely squashing their intrinsic motivations to deliver the program. Whereas reducing barriers by including all the key program content through technology can still preserve the role of providers to personalize treatment, although in ways that do not reduce the fidelity of intervention content, and creates the human touch that is more likely to enhance bidirectional interpersonal accountability between providers and participating children and caregivers. Furthermore, human providers are necessary to use their skills to organize and lead groups and keep participants engaged and interacting with one another.
Operationalizing the aforementioned analogy, the following components are proposed for design and prototyping of a comprehensive solution:
User-friendly human subjects and Health Insurance Portability and Accountability Act (HIPAA)-compliant web-based and mobile software that guides providers through every step of program implementation: patient recruiting, screening, enrollment, administrative and logistical group management, step-by-step protocols and content for each session; monitoring patient/family progress on attendance, weight, self-monitoring food intake, physical activity, screen time, smart goal-setting, goal achievement, rewards, skills mastery; providing feedback to children and caregivers regarding performance and progress; as well as documentation for billing and demonstrating outcomes for payers. Delivery of key content components through brief videos and/or animations to promote accessibility and high fidelity delivery of key components. Web and mobile software for patient participation: Maintaining updated and correct paper-based materials for each session is an obstacle for delivery for both providers and participants. This allows just-in-time access, interactivity, and unobtrusive collection of use and performance data. Onsite and online provider training: Based on experience, different providers favor different mixes. Ongoing online assistance and support resources including some live support: Based on experience, access to just-in-time assistance and support is highly valued. Certification of providers based on direct assessment of key process parameters and outcomes: Experience to date suggests providers will value the ability to become certified, potentially a competitive advantage, or used by payers to determine reimbursable services. The proposed use of technology enables monitoring provider actions (e.g., delivery of key program components) and patient flow and performance through treatment, from screening to outcomes. The data also allow for interim feedback to providers to help them continuously improve their implementation practices and outcomes. Potential customers (providers): Likely customers who can support such programs are hospitals (>6000 hospitals in the United States
c
), health systems, health plans, employers, federal, state and local public health agencies, community foundations, youth/family services organizations (e.g., boys & girls clubs, parks and recreation departments, and Ys), health clubs, and individual medical and nutritional professionals and groups. Multiple revenue models must be investigated: The focus on providers as customers represents a business-to-business (B2B) model. One possibility is a recurring revenue subscription model linked to certification. Additional possible revenue sources may be bundled or unbundled with subscriptions. Once a program is established, additional revenue sources may include direct-to-consumer (D2C) products and partnerships and/or licensing possibilities. We also acknowledge that providers will have to identify their own additional sources of support for implementation. Depending on the qualifications and licensing of providers, some existing billing codes already exist in the United States. Not all payers reimburse such codes, but we anticipate that more of these codes may become available over time. However, it is likely that providers will continue to need to find additional sources of reimbursement or funding, and these may vary in every different community. Additional innovation is needed to address this barrier. Intellectual property (IP): IP for the SPWCP is owned by Stanford University, and not likely to pose a barrier to broadly scaling and disseminating the program in this specific case. Regulatory issues: US regulation of medical software by the FDA is rapidly evolving. Research to date suggests the proposed technology package may be excluded from FDA classification as Software as a Medical Device (SaMD).
Conclusions
An approach, grounded in the IDEAS framework for digital health innovation and the Stanford Byers Center biodesign innovation process, was used to design a way to make effective behavioral weight control more scalable and cost-effective for low-income children with overweight and obesity, to reduce obesity and associated morbidities. The process considered the relevant stakeholders, the current market landscape, and potential market. Solutions were designed to address provider training and resources to have a strong foundation in behavior change methods, be sufficiently intense to produce change, involve both children and caregivers, and be delivered in groups, to be less costly to deliver than current family-based behavioral programs, and to have a viable revenue model. An iterative process resulted in a solution that combines both technology and human affordances and addresses high fidelity delivery, needs of providers and patients, training and support, likely customers, potential revenue models, intellectual property, and regulatory issues.
Footnotes
Acknowledgments
The author thanks the faculty fellows, instructors, and mentors from the 2018 Stanford Byers Center for Biodesign Faculty Fellows program, and the many children and families and staff members who have participated in the Stanford Pediatric Weight Control Program.
Funding Information
The preparation of this manuscript was supported by the Centers for Disease Control and Prevention (CDC) of the US Department of Health and Human Services (HHS) as part of a financial assistance award U18DP006423. The contents are those of the author and do not necessarily represent the official views of, nor an endorsement by, CDC/HHS, or the US Government, or any other funders. The development of the content presented was supported by the Stanford Maternal and Child Health Research Institute and the Department of Pediatrics, Stanford University, the Lucile Packard Children's Hospital Stanford, the Lucile Packard Foundation for Children's Health, and the Stanford Byers Center for Biodesign at Stanford University.
Author Disclosure Statement
T.N.R. serves on scientific advisory boards for WW International, Inc.