
Abstract
Background:
We examined the moderating influence of home location and school type across time on cardiometabolic risk and active school commuting over 5 years in a sample of children from southern Brazil.
Methods:
We recruited a sample of children (n = 154; baseline age = 9.6 ± 1.5 years old; 56.8% female) who were followed for 5 years from 2011/2012 to 2016/2017. We collected home location, school type, and school commute data using self-report methods and collected cardiometabolic risk measures to calculate a cardiometabolic composite risk score (cMetSyn). General and generalized linear mixed effects models were employed to examine the moderating influence of home location and school type across time on cardiometabolic risk and active school commuting.
Results:
We found a significant three-way home location × school type × time interaction on cMetSyn scores (b = 0.62, 95% confidence interval [CI]: 0.13–1.12, p = 0.014), indicating that children who were living within rural areas and enrolled in state schools during 2016/2017 had higher cardiometabolic risk compared with children enrolled in municipal schools and living in urban areas at the end of the study. Additionally, we found that children living in rural areas had an 86% lower rate of active school commuting compared with students living in urban areas (rate ratio = 0.14, 95% CI: 0.07–0.32, p < 0.001).
Conclusions:
The results suggest that Brazilian children enrolled in state schools and living in rural areas had higher cardiometabolic risk scores at the end of the study and that southern Brazilian children residing in rural areas had a much lower rate of actively commuting to school.
Introduction
There are health inequalities in Brazil that are prevalent within the country's rural areas. 1 The per capita income of residents within Brazil's rural areas is approximately two times lower than the average income in urbanized areas with the majority of rural households dependent on public health services. 2 However, overweight and obesity prevalence tends to be highest in the developed south and southeastern Brazil. 3 Within the Brazilian pediatric population, for every 100 Brazilian children, an estimated 12 children have obesity. 4 Of concern is a relative lack of health-related studies conducted on children and adolescents within Brazil's rural areas (85% of Brazil is urbanized) and a lack of longitudinal comparison studies using cohorts of children from southern Brazil. 4
The public school system in Brazil is separated into either state- or municipal-funded schools. Trained physical education teachers are available from first grade through high school within municipal-funded schools; whereas state-funded schools typically have physical education classes taught by generalist teachers from the first through fifth grades. Therefore, trained physical education teachers are only available in state-funded school students from the sixth grade onward. 5 Previously, we found that students from state-funded schools had higher levels of body fat and lower cardiorespiratory endurance compared with students from municipal-funded schools. 5 Using other cross-sectional data, we also found that children from Brazilian state and municipal schools tended to have different levels of cardiometabolic risk. 6 These state–municipal school differences may have been because of the discordance in resources for quality physical activity (PA) promotion. 6
PA has numerous health-related benefits for children and adolescents.7–9 Socioecological models suggest that PA is influenced by environmental factors, including the home and school.10,11 However,12,13 children who reside in homes within rural areas have been shown to be at a disadvantage for PA opportunities.14,15 Barriers particular to residing in rural areas include long travel distances to venues that promote PA.12–15 Indeed, long travel distances to rural schools may preclude active school commuting.16–19 Rural areas may also not have a sufficient density of safe and accessible walking paths, biking paths, or sidewalks needed to facilitate active school transportation.16–19 Although previous research utilized repeated cross-sectional designs to determine PA behavior patterns in Brazilian youth, 20 environmental moderators of the differences in behaviors across time points were not examined; therefore, it is unclear if living in rural areas or attending state schools have an impact on a specific PA behavior, active commuting, as indicated by the socioecological model.
A longitudinal study may also improve internal validity of the findings and also show how both cardiometabolic health and active commuting change across time according to home location and school type as the same cohort of children progresses from childhood into adolescence. Furthermore, in other pediatric populations, cardiometabolic risk tends to be stable as children progress into adolescence;9,21 however, it is unclear if these patterns are also observed within a cohort of children from southern Brazil. Therefore, we examined the moderating influence of both home location and school type across time on cardiometabolic risk and active school commuting over 5 years in a sample of children from southern Brazil.
Materials and Methods
Participant Recruitment
We conducted this observational longitudinal study, a part of the Schoolchildren's Health Study, which began during 2011/2012 academic school year. The Schoolchildren's Health study was a lifestyle education program developed by a multidisciplinary team of nutritionists, nurses, pharmacists, physiotherapists, and physical educators that targeted a large cohort of children enrolled in schools within southern Brazil. We recruited a sample of children from 25 schools from Santa Cruz do Sul (RS, Brazil) using multistage cluster sampling and invited these children to complete three assessments during the 2011/2012, 2014/2015, and 2016/2017 academic school years. We received Institutional Review Board approval for this study from the Committee of Ethics in Research with Human Subjects of the University of Santa Cruz do Sul (UNISC), under protocol number 3044/11; 714.216 (CAAE: 31576714.6.0000.5343); and 1.498.305 (CAAE: 54982616.7.0000.5343), respectively, for 2011/2012, 2014/2015, and 2016/2017. We also obtained written informed consent signed by the parents/guardians.
A power analysis was conducted using a two-tailed alpha level of 0.05, a mixed factorial research design with repeated measures, and an expected small effect size (Cohen's f = 0.15). To detect a small effect size for between–within-subjects interactions at 80% power, we determined that the sample size needed to be n = 108. The final analyzed sample consisted of 154 children with a mean baseline age of 9.6 ± 1.5 years (56.8% female). We provided a table communicating the sample's descriptive statistics (Table 1).
Descriptive Statistics for the Total Sample and Within Sex-Specific Groups at Baseline (Presented as Means and Standard Deviations and Counts and %s)
Bold denotes statistical differences between the sexes, *p < 0.05.
cMetSyn, cardiometabolic risk score.
Procedures
Self-report assessments
We administered all assessments at the University of Santa Cruz do Sul, Brazil using trained research assistants. Home location, school type, and commute data were obtained from a self-report questionnaire. The open-ended response items asked the following questions: “In which school do you study?” and “What neighborhood do you live in?” We then classified state and municipal schools, and rural and urban home locations according to responses of the participants. Within Brazil, there are 26 states (in addition to 1 Federal District) that are further divided into smaller municipalities, each with its own level of government that shares education responsibilities. A respective school is funded either by its state or municipality. This information was obtained from school administrators. Our operational definition of the binary urban–rural home location variable was based on the Brazilian 2000 Demographic Census. The census tracts that were characterized as urban areas were cities, villages, or isolated urban areas. The census tracks that were characterized as rural areas were areas outside large metropolitan areas, dispersed settlements, and villages located outside the urban center in municipalities of varying sizes (i.e., both accessible and remote rural areas).
To evaluate the school commuting status, a self-reported item asked, “How do you predominantly travel to school?” The responses consisted of (1) bus, (2) on foot, (3) car or motorcycle, and (4) bicycle. We then recategorized these items into a binary response variable indicating active (i.e., on foot, bicycle) and passive (i.e., bus, car, or motorcycle) school commute status. Skin color was self-reported by the participants, and we obtained socioeconomic status scores based on items found in participants' parents' household and education status. 22
Fitness assessment
We estimated cardiorespiratory fitness (VO2peak) using the 9-minute running and walking test established by the Projeto Esporte Brasil in 2011/2012 and the 6-minute running and walking test established by the Projeto Esporte Brasil in 2014/2015 and 2016/2017.23,24 The tests were performed on an outdoor track. We instructed the participants to run as long as possible with subsequent quantification of the total distance covered in meters and then converted the measured distance into estimated peak oxygen uptake (VO2peak) using equations where running distance covered, BMI, and sex were used as predictor variables.25,26 The prediction models showed evidence for criterion-related validity against laboratory-measured VO2peak and showed no systematic bias or heteroscedasticity when applied to a crossvalidation sample.23,24 Participants' height and weight were measured, with shoes off, using a medical scale with a coupled stadiometer (Filizola, Sao Paulo, Brazil). BMI was calculated by dividing body mass (in kilograms) by height (in square meters). We calculated BMI z-scores using Stata's “zanthro” package for further analysis.
Cardiometabolic risk score assessment
We measured waist circumference (WC) using an inextensible tape measure, using the narrowest part between the ribs and the iliac crest as the reference. Systolic blood pressure was measured early in the morning with the participants sitting at rest using a sphygmomanometer (B-D®, aneroid, Germany). Serum levels of 12-hour fasting glucose and blood lipoprotein-lipids were evaluated through direct venous blood collection. We analyzed the serum samples using commercial the Kovalent/DiaSys Kits (DiaSys Diagnostic Systems, Germany) in an automatic analyzer (Miura 200; I.S.E., Rome, Italy). We calculated sex- and age-specific standardized z-scores using international references for each cardiometabolic risk factor as established by Stavnsbo et al. 27 The cardiometabolic composite risk score (cMetSyn) was calculated by summarizing z-scores of estimated VO2peak, WC, glucose, systolic blood pressure, ratio of triglycerides over high density lipoprotein cholesterol. TC/HDL-C ratio, and triglycerides and dividing it by six.
Statistical Analyses
We presented data descriptively as means and standard deviations for continuous variables and as counts and %s for categorical variables. There were <5% missing data for all variables at each time point; therefore, we did not impute missing data. We employed two separate multilevel mixed effects models; one model for the cMetSyn-dependent variable and one model for the active school commuting-dependent variable. A general linear mixed effects model (LMM) examined the association between home location, school type, and time on the continuous cMetSyn scores. For the LMM model, the primary predictor variable of interest was the categorical time variable (referent = 2011/2012), and both the home location and school type variables were analyzed as moderator variables. The LMM-dependent variable was the cMetSyn variable. The LMM model was adjusted for student skin color and socioeconomic status. We did not use age and sex as LMM covariates because they were used within the cMetSyn calculation, and we did not use BMI z-score as a LMM covariate because of the strong association between BMI z-scores and WC.
A generalized linear mixed effects model (GLMM) examined the association between home location, school type, and time on whether a student actively commuted to school (0 = Passive Commute, 1 = Active Commute). For the GLMM model, the primary predictor variable of interest was the categorical time variable (referent = 2011/2012), and both the home location and school type variables were analyzed as moderator variables. The GLMM-dependent variable was the binary active school commute variable. We used a log link with robust variance estimation within the GLMM to obtain rate ratios (RRs) for interpretation.28,29 Although the log link function is typically employed for count data, it has been recommended that log link functions (Poisson regression) can be employed when the binary outcome within prospective cohort studies have a common indicator, in this case active school commuting.28,29 The GLMM model was adjusted for age, sex, skin color, socioeconomic status, and BMI z-scores. For both models, main effects and two-way and three-way interactions among home location, school type, and time variables were tested to determine the presence of effect modification.
Pair-wise comparison post hoc tests were performed if significant interactions were observed to specifically determine where the mean differences were across home locations, school types, and time points. We used random intercepts at the student and school levels to account for the multiple time point measurements nested within students and multiple students nested within schools. Results reporting consisted of unstandardized regression coefficients from the LMM and RRs from the GLMM. We set the alpha level at p < 0.05 and all analyses were carried out using Stata v17.0 statistical software package (StataCorp., College Station, TX).
Results
We presented the results of the LMM on the cMetSyn continuous dependent variable (Table 2). We found a significant home location × school type × time interaction on cMetSyn scores (b = 0.62, 95% confidence interval [CI]: 0.13–1.12, p = 0.014). Therefore, both home location and school type moderated the changes in cardiometabolic risk across time points. Pairwise comparison post hoc tests revealed that in urban home locations, children enrolled in state schools had higher cMetSyn scores compared with children enrolled in municipal schools in 2011/2012 (mean difference = 0.16, p = 0.022, d = 0.32) and in 2014/2015 (mean difference = 0.11, p = 0.034, d = 0.18). In rural home locations, we found that children enrolled in state schools had higher cMetSyn scores in 2011/2012 (mean difference = 0.23, p = 0.007, d = 0.46) and in 2016/2017 (mean difference = 0.20, p = 0.039, d = 0.34).
Regression Coefficients from the General Linear Mixed Effects Model on the Composite Cardiometabolic Risk Score Outcome Variable
Bold denotes statistical significance, *p < 0.05, **p < 0.01.
95% CI, 95% confidence interval.
We also observed that children enrolled in state schools and living in rural areas had higher cMetSyn scores compared with children enrolled in state schools but living in urban areas in 2016/2017 (mean difference = 0.24, p = 0.011, d = 0.27). No other significant pairwise differences in cMetSyn scores were observed. We displayed the unadjusted three-way interaction within Figure 1.
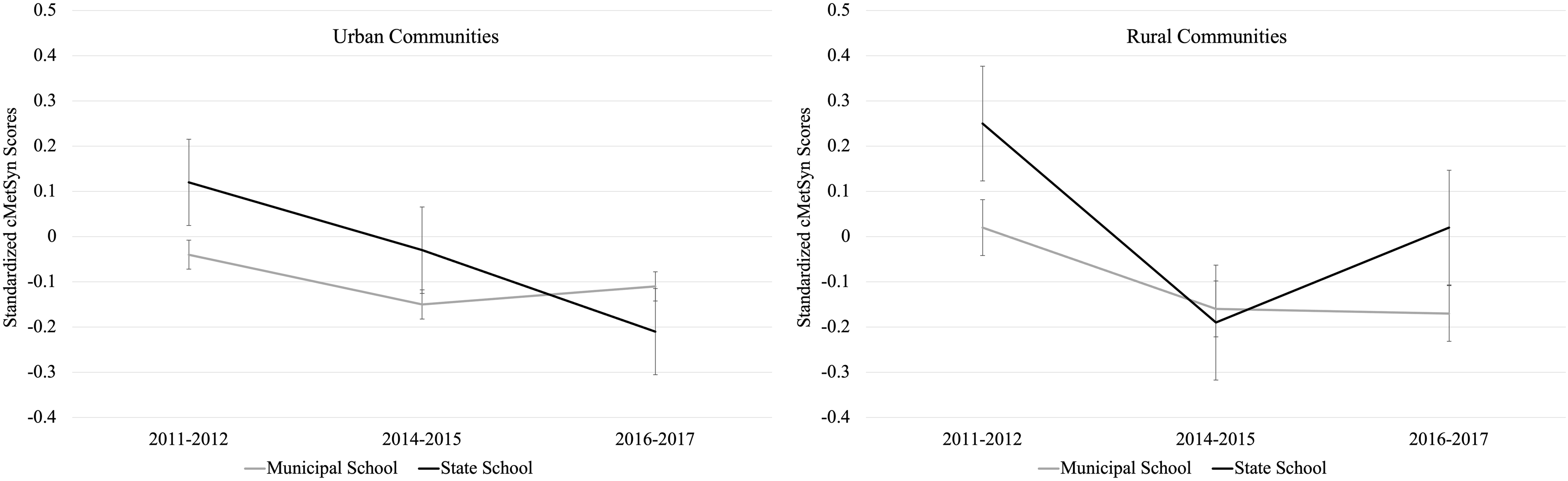
Clustered line graph showing the time trends in cardiometabolic risk (cMetSyn) scores and the moderating influence of home location and school type. cMetSyn, cardiometabolic risk score.
We presented the results of the GLMM on the active school commuting-dependent variable (Table 3). After covariate adjustment, there were no significant two-way and three-way interactions. However, we did observe a home location main effect as children residing in rural areas had an 86% lower rate of actively commuting to school compared with children living in urban areas (RR = 0.14, 95% CI: 0.07–0.32, p < 0.001). The unadjusted prevalence of active school commute status between urban and rural home locations are presented within Figure 2.
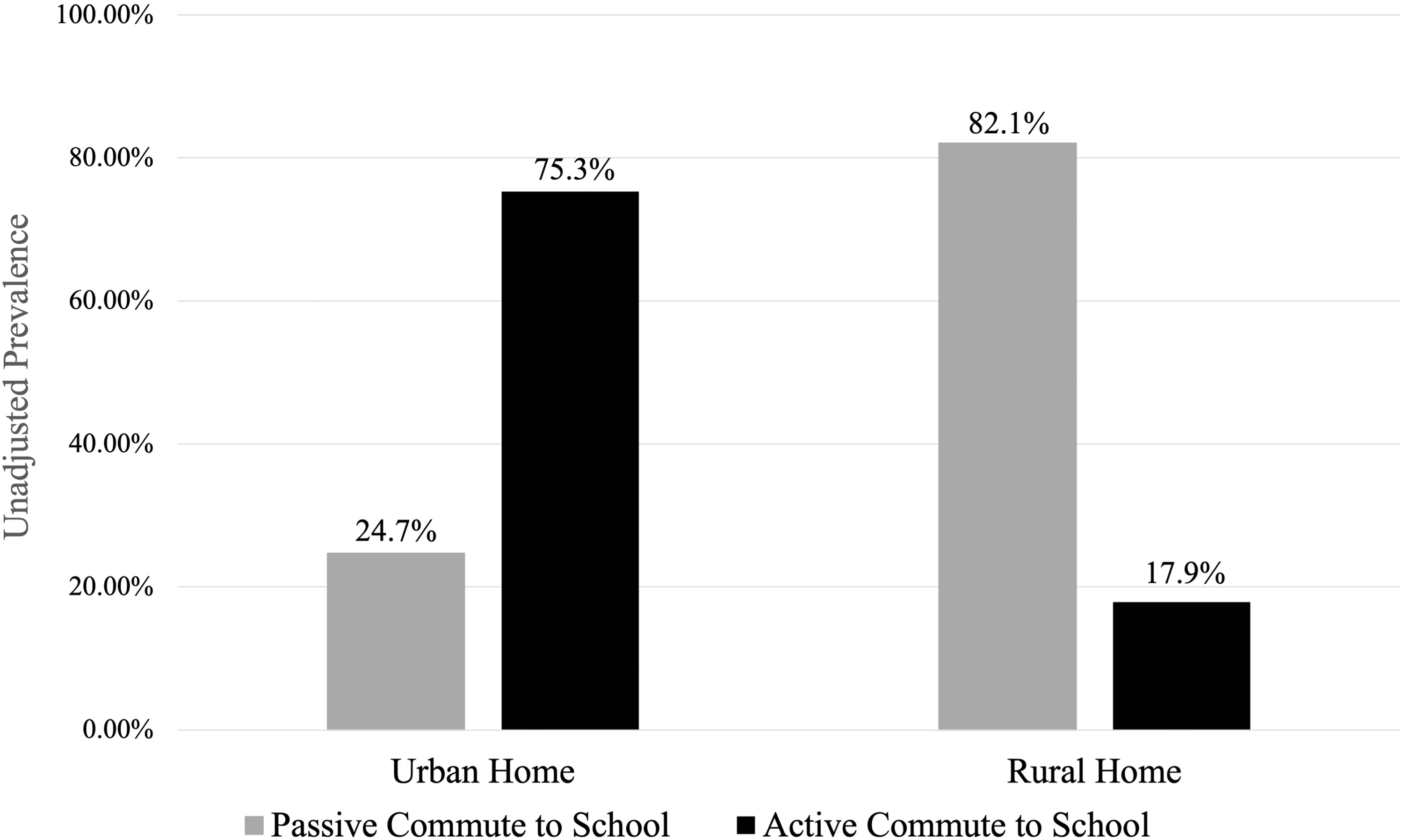
Active school commuting prevalence pooled across time points for children living in urban and rural communities.
Incidence Rate Ratios from the Generalized Linear Mixed Effects Model on Active Commuting to School
State × rural × 2016/2017 was omitted because of collinearity; bold denotes statistical significance, *p < 0.05, **p < 0.01, ***p < 0.001.
IRR, incidence rate ratio.
Discussion
In this study, we examined the moderating influence of both home location and school type across time on cardiometabolic risk and active school commuting over 5 years in a sample of children from southern Brazil. We found higher cardiometabolic risk scores at the end of the study in southern Brazilian youth enrolled in state schools and living in rural areas. We believe that this could be partially be explained by the fact that students enrolled in Brazilian state-funded schools do not have physical education classes developed by trained and certified physical education teachers at early ages. 30 Conversely, within Brazilian municipal schools, there are trained and certified physical education teachers responsible for early physical education classes. 30
Considering that childhood is a crucial period for the development of motor skills and health-related fitness, we believe that it is essential that these components of physical education are properly developed by trained physical education professionals within all Brazilian school types.5,31 Indeed, a study carried out on Brazilian children indicated that students from municipal schools presented higher levels of physical fitness compared with the students from state schools. 5 Given trajectories in the current study, the genesis of higher cardiometabolic risk may commence in childhood but not be observable until adolescence.
Urban–rural differences in cardiometabolic health and has also been found in other work, with rural youth tending to have unfavorable health outcomes and all-cause mortality compared with urban youth. 32 A potential mechanism of poorer health in rural children is the higher prevalence of overweight and obesity. 33 Determinants of overweight and obesity include energy balance-related factors, such as diet quality and quantity, in addition to PA.33,34 These factors tend to be related to socioeconomic status.33,34 There also may be urban–rural differences in cardiorespiratory fitness and sedentary behavior, which also contribute to cardiometabolic risk. 35 Specific to Brazil, individuals residing in rural areas comprise <15% of the population as the country is highly urbanized. Because of this and the relative paucity of comparative studies examining the differences in health outcomes between rural and urban Brazilian youth, it was unclear if the rural environment contributed to higher cardiometabolic risk.3,4
To our knowledge, this is the first study to show an unfavorable trend in cardiometabolic risk within children residing in rural areas in southern Brazil, an effect that was further moderated by school type. Reasons for the differences in findings compared with other studies include the use of more direct assessment of health in the continuous cMetSyn score rather than BMI, 27 controlling for cardiorespiratory fitness in the calculation of cMetSyn, and the consideration of school type as an additional moderator variable of the time trends.
A secondary finding was that children who resided in rural areas had a much lower rate of actively commuting to school compared with children residing in urban areas. A lack of sufficient non-school PA during unstructured days in addition to low active commuting during structured days may both contribute to lower overall PA and fitness in children from rural areas. 19 However, differences in specific PA behaviors, like active school commuting, between children residing in urban and rural areas may be moderated by geographical area and seasonality.36,37 Nevertheless, active commuting has been shown to be a significant overall contributor to both daily PA and weight status in a variety of pediatric populations.38–40 Active school commuting has been found to be lower in children residing in rural areas compared with children from urban areas, with distance to school being a significant inverse predictor of the PA behavior.40–42 In the current study, we found that active commuting incidence was much lower in children residing from rural areas of southern Brazil. These findings support other research, but it is unclear if PA is indeed a mechanism contributing to cardiometabolic health.
It is also unclear what specific perceived barriers may contribute to active school commuting in this population as previous work has shown that child and parent barrier perceptions do not agree 43 ; however, improving traffic safety, providing equipment for active travel, making walking/biking trails easily accessible, and improving neighborhood and school esthetics have been proposed intervention methods to improve the incidence of child active school commuting. 44
Limitations to this study include the use of self-report to assess home and school location and active commuting to school; therefore, there is potential for both recall and social desirability bias in the responses that affects the internal validity of the results. Additionally, only active school commuting status data were collected and there was no valid total day PA assessment. Therefore, it is unclear the magnitude of the contribution of active commuting to total day PA. It is also unclear if PA behavior, influenced by active school commuting status, is indeed a mechanism linking home location and school type to cardiometabolic risk. Valid and objective assessments of PA behavior are needed to address this critical gap in the literature. Finally, the sample consisted of children and adolescents from southern Brazil, therefore, we recommend that researchers and practitioners use caution if the results are generalized to other pediatric populations.
Conclusions
We found that Brazilian children enrolled in state schools and living in rural areas had higher cardiometabolic risk at the end of the study when the children tracked into adolescence. Mechanisms for these associations may be due to a lack of resources and insufficient physical education teacher training within Brazilian state-funded schools and barriers to engage in PA for students residing in rural areas. The rate of active commuting to school was very low in children from rural home locations compared with students from urban home locations. Lower active school commuting may be a mechanism to higher cardiometabolic risk in Brazilian youth, but this association should be examined using more valid assessments of PA behavior. This longitudinal study can help justify and derive interventions targeting rural Brazilian children to improve health outcomes and active commuting behaviors as they progress into adolescence.
Footnotes
Authors' Contributions
We believe that all authors have met the definition of authorship, as defined by the International Committee of Medical Journal Editors. R.D.B. conceived the secondary data analysis methodology, conducted the formal statistical analysis, interpreted the results, and wrote the initial draft of the article. A.P.S., C.B., and J.F.d.C.S. collected data, interpreted the results, and critically revised the initial draft of the article. C.P.R. provided administrative support, interpreted the results, and critically revised the initial draft of the article. All authors approved this initial version of the article to be submitted for publication consideration and all authors agreed to be accountable for all aspects of the study.
Acknowledgments
The authors would like to thank the children and adolescents who participated in this study and the graduate assistants who aided in the data collection process.
Funding Information
We received funding for this study from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—finance code 001.
Author Disclosure Statement
No competing financial interests exist.