
Abstract
Background:
Over the past two decades, childhood obesity has been recognized as an increasing health problem with stark disparities by race, ethnicity, and zip code. A single-level intervention that focuses on individual choices has limited success especially in under-resourced communities.
Methods:
The “Getting to Equity” model provides a framework for building interventions that incorporate multilevel strategies. We applied this model to an elementary school-based obesity prevention program.
Results:
By applying the “Getting to Equity” framework, we demonstrate how a school-based program aligns with the quadrants within the framework to holistically address childhood obesity.
Conclusion:
By applying this model to an elementary school-based obesity prevention program, we demonstrate how program leaders can address childhood obesity while advancing health equity.
Introduction
The rate of childhood obesity in Washington, District of Columbia (DC), is 35%. 1 According to the Robert Wood Johnson Foundation State of Childhood Obesity report From Crisis to Opportunity, the national obesity rate in 2019–2020 for youth of ages 10–17 was 16.2%. 2 However, obesity rates differ significantly across racial lines, with the rate of obesity for non-Hispanic Black youth at 23.8% compared with 12.1% for non-Hispanic White youth, and by household income, ranging from 8.6% to 23.1% between youth for the highest and lowest income groups, respectively. The COVID-19 pandemic has further accelerated childhood obesity with school closures, decreased physical activity, and increased screen time. 3
Previous research has focused solutions to childhood obesity through single risk factor interventions at the individual level. 4 Programs that teach children gardening or cooking skills are important, however, they have limited long-term impact in schools. 5 To effectively address health disparities, multilevel intervention strategies demonstrate greater potential by addressing broader societal, community, and environmental contexts while building on individual strengths.5,6 A systematic review of multilevel interventions indicates that targeting one individual-level strategy with at least one environmental approach shows promising results. 7 The Healthy Schoolhouse 2.0 (HS2) program addresses the interconnectedness of the student, school, and community that is necessary to advance equity and ensure sustainability.
Methods
Project Overview
HS2 is an ongoing 5-year childhood obesity prevention prospective intervention study with data collected from teachers, elementary students, and schools in DC 8 beginning School Year 2017–2018. HS2 addresses multiple tiers within the social–ecological model to support health, nutrition education, and obesity prevention. At the individual level, teachers attend five tailored professional development (PD) sessions that are responsive to their personal health needs and nutrition knowledge, while providing nutrition education content from the United States Department of Agriculture (USDA's) Serving Up My Plate: A Yummy Curriculum (SUMP). 9 In the PD series, teachers are invited to teach a minimum of three nutrition lessons each school year.
Expanding to the organizational level, through the integration of nutrition education lessons into core classes across grades 1–5, a school-wide emphasis on health and well-being is embedded into the culture and environment. At the broader community level, a partnership with a local nonprofit organization supports strong families and strong communities to reinforce the long-term commitment to health. In addition, HS2 established a board of advisors comprising stakeholders representing community-based organizations invested in strengthening the assets of these schools and neighborhoods. The board of advisors meets semiannually to receive program updates, offer guidance, and feedback, and share and adapt successes and lessons learned to other projects their organizations are implementing.
Participants
In the planning and design of HS2, the research team partnered with schools from Wards 7 and 8, the historically underserved southeast region of DC. Wards 7 and 8 residents are 94.7% and 93.7% Black/African American with median household incomes of $42,201 and $39,473, respectively, 10 compared with a median household income of $91,414 DC wide. All schools in this area participate in the community eligibility provision (CEP) that allows students to receive free school meals without households individually applying.
Framework
In seeking to reduce the risk and impact of childhood obesity in DC, a multilevel equity-focused approach in the school setting was critical. Kumanyika's Getting to Equity (GTE) in obesity prevention framework 11 describes the synergistic relationships essential for interventions to be sustained. The GTE framework (Fig. 1) builds on previous research on the systems that enable inequitable policies and practices in health as well as the education sector.12,13 The framework has four quadrants with the top two identifying process strategies for potential policy, systems, and environmental changes: Increase Healthy Options and Reduce Deterrents. The two lower quadrants emphasize pathways for enhancing individual and community resources and capacity: Build on Community Capacity and Improve Social and Economic Resources.
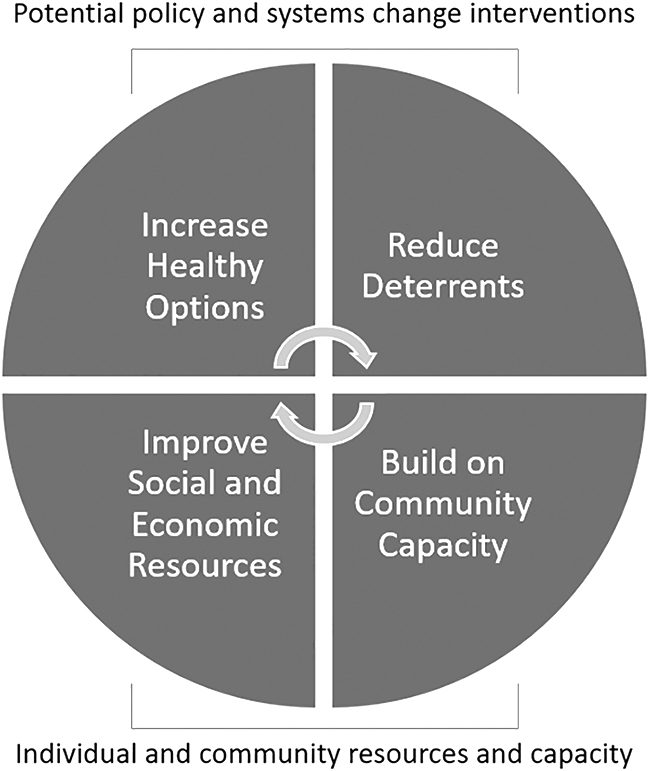
Getting to Equity in obesity prevention framework.
HS2 is a multilevel intervention addressing childhood obesity that activates each quadrant of the GTE framework through the following mechanisms: (1) a cross-disciplinary research team, (2) an advisory board representing various DC nutrition and education stakeholders focused on local needs, (3) codesign of PD sessions with input from teachers and administration throughout the process, (4) community engagement through a partnership with Martha's Table monthly Joyful Food Markets (JFMs), (5) development of culturally responsive instruments and data collection tools with feedback from partners, and (6) results are shared with the community, schools, and district first.
Using the GTE framework to guide program development and refinement, as well an asset-focused stance and the provision of a variety of supports that are tailored to the distinct environment and culture of each school,14,15 HS2 applies a whole school, whole community, whole child (WSCC) approach 16 to support safe, healthy, and engaged students while advancing equity in DC elementary schools. Herein, alignment of each GTE quadrant with HS2 program components is detailed.
GTE quadrant 1: increase healthy options
As a starting point, it was imperative to establish trust and a collaborative relationship with administrators and teachers in the intervention schools that value the contributions of school staff and research team. We recognize educators as the permanent residents of a school and thus their well-being may be a strong indicator of the overall school environment and climate. Engaging educators as partners in nutrition education started with a deliberate focus on what partners identified as needs in terms of staff wellness and was incorporated into the format and content of the PD programming requested by the staff, including yoga, mindfulness, a pedometer challenge, and healthy snacks during sessions with a variety of cooking items/equipment and fitness gear as giveaways throughout the program.
In supporting teachers and other staff, the emphasis orients toward a holistic coconstructed approach that impacts both the individual and school community. We sought to start with the heart of the school and increase access to the healthy options that would make the principles and nutrition education content of HS2 relevant and applicable to teachers first.
The design of HS2 was intentional in that the research team recruited partner schools that host JFMs, a program offered by local nonprofit Martha's Table. JFMs are pop-up monthly markets held in elementary schools in Wards 7 and 8. Families are invited to shop at no cost (due to the school's CEP status) for a variety of local high-quality produce, including apples, greens, and sweet potatoes, as well as basic shelf staples such as pasta and beans. School cafeterias and gymnasiums are transformed into joyful environments with staff wearing fruit and vegetable costumes, music, and dancing. Recipe cards along with food samples allow students and families to taste what they can make with the items available.
JFMs were an important time to strengthen relationships with school leaders, teachers, and students outside of the classroom. The research team led activities each month that connected nutrition concepts from the classroom lessons to physical activity in fun hands-on ways. For example, showing a plate with food items representing four of the five food groups and asking students to identify what food group was missing and hop to that space on the MyPlate outline taped on the floor. Creating real-world relevance to the nutrition education content and students' own experiences made students excited to understand this information that supports lifelong healthy eating.
GTE quadrant 2: reduce deterrents
HS2 utilizes USDA's SUMP that details nutrition education lessons for grades 1–6 that align with the Common Core State Standards in English Language Arts, Math, Science and Health. 11 The research team selected an USDA and WSCC aligned curriculum for multiple reasons that supported the school context and reduced the burden on teachers: (1) the USDA curriculum is free and laid out in a user-friendly format with accompanying handouts requiring very little prework, (2) the curriculum includes three levels covering grades 1–6 allowing for progressive and adaptive use across multiple grades, (3) each lesson consists of three mini-lessons with crossover applicability between subjects and easy integration of nutrition concepts into any class, and (4) kits were created and delivered to teachers at each grade level with all curriculum materials and supplies needed to conduct lessons.
To promote the highest level of inclusivity and participation by all teachers at intervention schools, prekindergarten and kindergarten teachers were also provided Discover MyPlate curricula and lesson materials (though these grades were not included in HS2 assessment). With the design of HS2 as a 5-year project, delivery of nutrition education lessons was intended to be progressive, cumulative, and efficient. With the engagement of most teachers, and content linkages to core subjects and related arts, students received lessons in multiple classes each year layering the content for stronger impact.
GTE quadrant 3: build on community capacity
Teachers at our partner schools, along with school leaders including principals, assistant principals, and community engagement coordinators, participated in the PD series designed to empower them as agents of change in creating a culture of health in the school environment. HS2 embeds capacity in the school community by addressing the skills, knowledge, attitudes, and materials needed to teach nutrition concepts.
Each PD session in the five-part series was 45 minutes in length and offered onsite at school during a regularly scheduled staff meeting. Sessions covered HS2 program objectives, a socioecological approach to nutrition education, guided walkthrough of each of three lessons in USDA's SUMP curriculum, practice time to model nutrition lessons, and nutrition myths and facts. As previously described, sessions also included time devoted to teacher health and wellness on topics that were selected by the participants.
Participation in the PD series was voluntary (although highly encouraged by school leadership) and teachers were able to choose which nutrition lessons they would implement, allowing for autonomy in deciding what content was most relevant to their students. The approach aligns with an equity mindset wherein teachers know their students best and can tailor lessons to their classrooms.
To further link the value of nutrition education with community strength and capacity, the partnership with an engaged community organization committed to empowering families and children in health was critical (described in GTE Quadrant 1: Increase Healthy Options).
GTE quadrant 4: improve social and economic resources
Initially 13 eligible schools were invited to participate, and a determining factor was school leadership engagement and commitment to collaborate with the research team to support the program. A designated point of contact within each school served as partner in the coordination of PD sessions and championed the value and impact of teaching nutrition education lessons. By identifying schools with leaders who recognize the assets of the school community and build connections between teacher well-being, student health, and academic performance long term, participation in HS2 deepens the capacity and engagement at multiple levels within the school and paves the way for equitable and lasting impact.
As stated, each participating school utilizes CEP and is in underserved neighborhoods of Southeast DC. Whether partnering as an intervention or comparison school, each school was to receive a yearly stipend ($1000 or $500, respectively) to purchase needed equipment or supplies. Within intervention schools, teachers who taught three nutrition lessons (the number defined as program completion) could also receive $75 to purchase classroom supplies that would support future lessons on nutrition and health. The research team endeavored to collaborate with the school staff to build upon the social support and environment regarding health across the school setting with near term incentives for participation that would reshape the context and approach long term for authentic transformation.
Results
HS2 findings thus far highlight the potential of school-based interventions to increase access to healthy options while reducing barriers in efforts to prevent and reduce childhood obesity. The preliminary results of HS2 demonstrate proof of concept that engaging teachers as agents of change can improve nutrition knowledge and behaviors among students, as assessed by the validated Student Nutrition Literacy Survey 17 with >1000 elementary school students.
Students who received three lessons had post-test knowledge scores that were on average 10% higher than those students who received fewer lessons [H(2) = 72.1, p < 0.001, n = 844]. 18 There were no significant improvements in knowledge scores among students who received more than three lessons, suggesting that three lessons is the optimal threshold for lesson implementation. Furthermore, teachers who attended more PD sessions were more likely to implement nutrition lessons in their classrooms [H(4) = 23.79, p < 0.001, n = 55].
These preliminary results suggest that engaging teachers to implement nutrition curricula may support sustainable obesity prevention efforts in the school environment and build upon community assets and resources.
Discussion
Although these findings are encouraging, knowledge is only one facet of behavior change and the GTE framework exemplifies that several components must be in sync for true and lasting impact to be achieved in preventing obesity. In underserved communities, it takes a significant investment in cooperative relationships and resources over multiple years to establish a foundation of genuine shared decision making and dedication to advancing health equity. There must also be an emphasis on using an asset-focused approach that is tailored to the strengths and opportunities of each community, thereby prioritizing and adopting an equity lens when applying research evidence in the real world. 19
For example, trusted community partners are an especially important component as they understand and are a part of the school community. Even with these pillars in place, competing demands on educators and staff turnover result in multiple resets within a school year, and across years of the program. Flexibility in implementation and meeting partner schools where they are is essential; calibrating a program's timeline and benchmarks according to the variables that impact the climate of a school and community must be continuous.
Inequitable policies and systems create health inequities. As equity-focused interventions expand, applying both multilevel strategies and the principles of Kumanyika's GTE framework will dismantle the drivers of health disparities that have been left out of the conversation far too long.
Footnotes
Funding Information
Funded by National Institute of Food and Agriculture from the Food Research Initiative Competitive Grant No. 2017-68001-26356.
Author Disclosure Statement
No competing financial interests exist.