
Abstract
Background:
Childhood obesity is a major health concern. Caregivers' feeding practices are modifiable targets of obesity prevention. The study tested two hypotheses: (1) autonomy-promoting feeding practices are associated with lower BMI; and (2) diet mediates the association. We also explored examined whether feeding practices and BMI z-score (BMIz) associations are moderated by child sex, caregiver race, education, family poverty level, and food insecurity.
Methods:
Cross-sectional study of 437 preschoolers (44.4% girls, 38.2% Black/Other, mean age 48.1 months) and caregivers (90.2% female) from 50 child care centers. Feeding Practices were measured by Comprehensive Feeding Practices Questionnaire, child-size perception by preschooler silhouettes, temperament by the Behavior Rating Inventory of Executive Function, child diet by Young Children Food and Drink Questionnaire, and BMIz by measured weight and height. Latent profile analysis delineated feeding practice patterns. Structure equation modeling assessed the patterns in relationship to BMIz. Mediation and multiple-group analyses were used to assess mechanisms of feeding practice patterns and BMIz association.
Results:
From the three feeding practice patterns, Controlling, Balancing, and Regulating, Regulating was associated with lower child BMIz (b = −0.09) compared to Controlling. Higher difficult temperament (b = 0.09), higher caregiver BMIz (b = 0.26), and caregiver desire for thinner (b = 0.23) were associated with BMIz (p < 0.05). Evaluations of moderators and mediators were not significant.
Conclusions:
Comprehensive feeding practices support family factors related to child BMIz. Longitudinal research is needed to examine temporal associations between feeding practices and BMIz, with attention to autonomy-supporting practices, promotion of young children's self-regulation, and caregivers' perceptions of child temperament and size. Trial Registration: NCT03111264.
Introduction
Pediatric obesity is a persistent health problem in the United States. After decades of prevention interventions, the prevalence of pediatric obesity remains high at 13.4% among preschoolers and increases among older children.1,2 Children with obesity are at increased risk to have obesity in adulthood, along with chronic diseases, resulting in an estimated cost to the United States health care system of $147 million a year. 3
Obesity is a complex multifactorial phenomenon impacted by multiple interactive layers of factors. The Bioecological Theory of Human Development emphasizes the dynamic interrelations between children and their proximal environment (the home), including families, communities, and society influencing children's development, behaviors, and growth. 4 Through bidirectional relationships, children's temperament, dietary patterns, sedentary behaviors, and physical activity elicit differential interactions from families, peers, and community members.
Feeding practices, as interactions between caregivers and children, may influence children's eating habits.5–7 Feeding practices are modifiable and may be targets for obesity prevention programs. Most studies examining the association of feeding practices and childhood obesity have focused on single selected practices, often with inconsistent findings. 8 For example, restriction of food and pressure to eat, respectively, have shown positive and negative relationships with childhood obesity in multiple studies.8,9 Other feeding practices have either not been included or have not shown associations with obesity in a recent systematic review.8,9
Acknowledging that multiple feeding practices are performed simultaneously, in our recent study, 10 we used an innovative empirically driven approach in a sample of caregivers of preschool aged children and identified three feeding practice patterns that correspond with the following three conceptual constructs: Controlling, Regulating, and Balancing. 10 Controlling was the most frequently endorsed (69%) and included high coercive control and low autonomy and structural practices. Regulating (16%) had high coercive control and moderate structural and autonomy practice, and Balancing (15%) had moderate levels of all practices. Autonomy support for children's eating behavior refers to providing both the structure and the emotional climate to engage children in the meal, building healthy habits, 11 and is an important component of responsive feeding and healthy growth. 12
In addition to defining three feeding practice patterns, our previous study identified child and caregiver characteristics associated with the patterns. 10 In the current study, we investigate how the three empirically identified feeding practice patterns relate to children's diet and BMI. Feeding practices are thought to influence children's self-regulatory behaviors related to food, 13 suggesting that diet may mediate the association of feeding practices and child weight gain.
The study tested two hypotheses: (1) the feeding practice patterns that promote autonomy (Balancing and Regulating) are associated with lower BMI z-score (BMIz), compared with Controlling; and (2) children's diet mediates the association between feeding practice patterns and children's BMI, with healthier diet associated with healthier BMIz. We also examined whether the associations between feeding practice patterns and BMIz are moderated by child sex, caregiver race, education, or family poverty level and food insecurity. These hypotheses are novel because they are based on the empirically derived feeding patterns 10 that conceptualize multiple feeding practices simultaneously in one model.
Methods
Study Design
This cross-sectional study used baseline data of the CHAMP (Creating Healthy Habits Among Maryland Preschoolers) study; details are published elsewhere. 14 The subsample of complete data consists of 437 children and their caregivers from 50 child care centers throughout Maryland.
Ethical Statement
The CHAMP study was approved by the University of Maryland Baltimore Institutional Review Board (126HP-00065933). Caregivers provided written consent for themselves and their children.
Recruitment and Data Collection
The study team collected anthropometric data on participating children and sent caregivers a link to complete online questionnaires, including demographics, diet, temperament, feeding practices, and perceptions of child size.
Measurements
Child BMIz
Weight was measured in triplicate using a TANIA BWB-800 digital scale after removing jackets and shoes, rounded to the nearest 0.1 kg. Height was measured in triplicate using a stadiometer without shoes with both heels touching the wall, rounded to the nearest 0.1 cm. BMIz was calculated using CDC age and sex-adjusted datasets. 15
For descriptive purposes, we calculated BMI percentile (BMIp) categories: BMIp <5th underweight, 5th to <85th normal weight, 85th to <95th overweight, and 95th or above obesity. 15 The underweight (3.4%) and normal weight group were collapsed.
Child diet
We used a short form of Food Frequency Questionnaire for young children, short FFQ 16 to describe children's diet. The short FFQ assesses food and drinks, including consumption of fruits, vegetables, processed meat, French fries, potato chips, fast foods, candy, chocolate, and soda. Response choices are no serving, one serving/month, one serving/week, and one serving/day except the fruits and vegetables (no serving at all, one serving/week, one serving/day).
This questionnaire has shown good reliability, and acceptable validity for children aged 2–5 years. Concurrent validity of the short, compared with longer, forms of FFQs has been satisfactory for consumption of fruit and vegetable. 16 Lacking a recommendation on score creation, we used structural equation modeling (SEM) to create a latent variable using all items, except fruits and vegetables, which we called Sugars/Snacks/Saturated Fat (SSS). For descriptive purposes, tertiles of the total SSS scores were calculated. The fruit/vegetable variable was defined as having at least one daily serving (1) vs. no daily serving (0).
Child demographics
Child age was reported in months, and sex as girl vs. boy. Race was categorized as White vs. Black/Other and included Black (24.7%), Mixed (3.6%), Asian (3.4%), Native American (0.7%), Vietnamese (0.2%), Hawaiian (0.2%), and Latinx (3%).
Child temperament
Emotional control and inhibitory subscales of the caregiver-reported Behavior Rating Inventory of Executive Function, Preschool Version (BRIEF) captured children's control of emotions, actions, and responses.17,18 The BRIEF has been validated among US preschoolers, with good reliability14,17 and acceptable validity among Maryland children. 19 The subscales have 10 and 16 items, respectively, and use a three-point Likert scale. Mean subscales t-scores were calculated; higher scores indicate more difficult temperament. 17
Caregivers' feeding practice patterns
The Comprehensive Feeding Practices Questionnaire (CFPQ) was used to measure single-feeding practices. This questionnaire has shown consistency for mothers, fathers, and multiple modes of survey administrations, 20 with satisfactory to robust reliability (coefficient alpha = 0.58–0.81) and good convergent validity to caregivers' attitudes toward children's weight. 14 This questionnaire has been widely used and validated in several studies and populations and deemed appropriate to capture a wide range of practices.21–25 The CFPQ has 48 items capturing feeding practices, including monitoring (4 items), emotional regulation (3 items), food as a reward (3 items), child control (5 items), modeling (3 items), restriction for weight control (8 items), restriction for health (3 items), teaching nutrition (3 items), encouraging balance (4 items), pressure to eat (4 items), healthy environment (4 items), and involvement (3 items).
Responses are in 5-point Likert scale, ranging from 0 (disagree/never) to 4 (always/agree). After three items are reverse codes, higher scores show higher use of each. Following factor analysis of the 48 items of the CFPQ, the best model of the latent profile analysis delineated 3 patterns: Controlling, Regulating, and Balancing. 10 The Controlling pattern included high coercive control behaviors and low autonomy behaviors. The Regulating pattern included high coercive control behavior and moderate other behaviors, and the Balancing pattern was moderate in all behaviors. 10 These three patterns were used in the analyses.
Caregivers' perception of child size
We used seven silhouettes of 4-year-old children with good reliability, high interobserver agreement, and satisfactory concurrent validity with weight-length percentile. 26 Caregivers reported their child's current and ideal weight from the silhouettes ranging from 1 (thinnest) to 7 (heaviest). The difference between the ideal and current size was calculated and categorized as desire thinner, satisfied, and desire heavier.
Other caregiver characteristics
Caregivers' age was captured in years, sex as female and male, race as White vs. Black/Other, BMI using caregivers' self-reported weight and height, education as high school or less, some college, bachelors or beyond, marital status as single vs. nonsingle, and employment as full-time vs. non-full-time.
Family poverty level and food insecurity
Caregivers reported the total household income and responded to the two-item Food Insecurity screener. The screener showed adequate sensitivity, specificity, and validity to measure household risk of food insecurity14,26 with a 3-point Likert scale. Endorsement of “sometimes” or “often” in either of the two items indicates risk for food insecurity. 26 The family poverty level is the total household income divided by the federal poverty threshold for a given family size in 2018. 27 The final variable indicates three levels: <200, 200–300, and >300.
Statistical Analysis
Missing values were <10% in all the variables and completely at random. Children with and without missing were compared based on available variables (sex, race, ethnicity, age, BMIz) and no significant differences were found. We used Full Information Maximum Likelihood with robust estimators to account for missingness, SPSS 26 (Statistical Package for the Social Sciences, IBM Corp. Armonk, NY), and MPLUS 8.4 (Muthen and Muthen, Los Angeles, CA) for all analyses.
Child BMIz was regressed on the feeding practice patterns (Controlling pattern was used as the reference category as it had the highest prevalence among caregivers) and other characteristics using bivariable and multivariable regression in the SEM framework, and with child care center as a clustering variable. To achieve a parsimonious model, only variables with p < 0.15 were included in the final model. 28 The mediation effect of diet (SSS food and fruits/vegetables) was tested in the final parsimonious model using multivariable path analysis SEMs. To have a significant mediation effect, feeding practice patterns had to be associated with either SSS or fruit/vegetables and the pathways from diet, SSS food, and fruit/vegetables to the child BMIz had to be significant.
For models that were not just identified, we assessed model fit with the following criteria: Comparative Fit Index (CFI), Standardized Root Mean Squared Residual (SRMR), and Root Mean Squared Error of Approximation (RMSEA), with cut points of >0.90, <0.08, and <0.06, respectively, indicating acceptable fit. 29 The relationships were reported with the standardized beta coefficient and p-Value.
To test moderation, several multigroup SEMs were built on the parsimonious model. Rather than focusing on parameters in a single group, multigroup SEMs make comparisons of parameters between different populations. In these analyses, we determined if associations between feeding pattern classes and child BMIz vary by child sex, caregiver race, education, poverty level, and food insecurity. Each time, the model was stratified based on one of the moderators with and without equalizing other parameters in each stratum. Parameter differences were tested using the Wald test. Interaction effects were checked using general linear models.
Results
The sample of 437 preschoolers and their caregivers included slightly more boys (55.6%), White race (61.8%), and non-Hispanic or Latino (96.0%), with mean age of 48.0 months [standard deviation (SD) = 7.5]. Most children (79.7) had at least one daily serving of fruits/vegetables, and 32% had high SSS food consumption (Table 1).
Child and Caregiver Characteristics by Child Weight Status (n = 437)
SD, standard deviation.
Most caregivers were female (90.2%), mean age of 35.14 years (SD = 5.6), and BMI of 27.48 (SD = 6.1). The majority of them were married (71.6%), working full-time (85.1%) with education at bachelor's or beyond (70.4%), above the federal poverty level (93.5%), and food secure (88.1%). Most were satisfied with their child's size (72.5%); 69.3% of caregivers endorsed the Controlling feeding practice pattern. Table 1 stratifies characteristics by weight status. More than three fourths (76.1%) of the children had a healthy weight, with 13.6% classified as having overweight and 10.3% as having obesity.
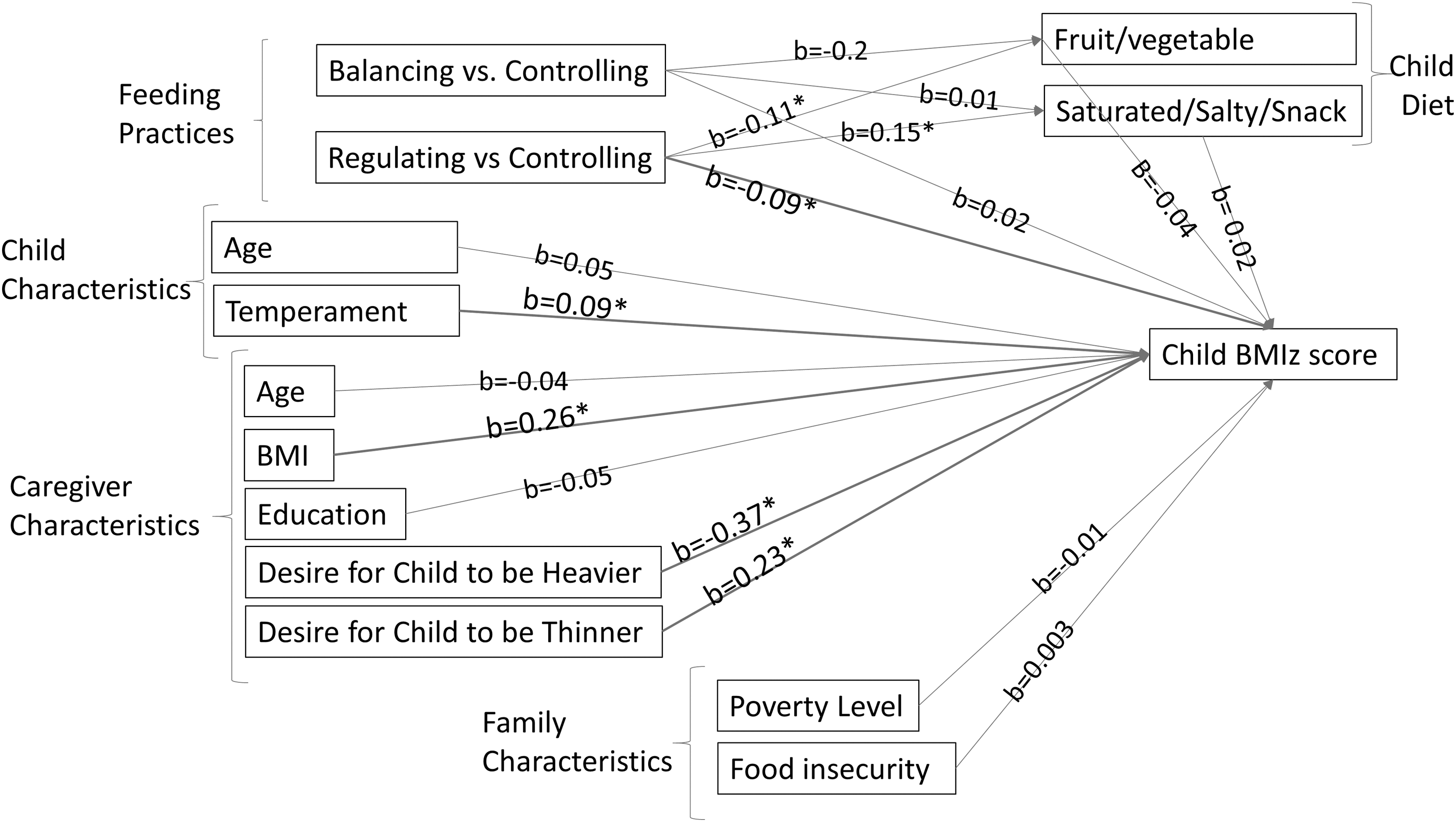
Table 2 summarizes the associations of feeding practice patterns, child, caregiver, and family characteristics with child BMIz. Bivariable, multivariable and parsimonious model estimates are reported for comparison. In the final parsimonious model, the Regulating vs. Controlling pattern was negatively associated with child BMIz (b = −0.09, p = 0.03). Child temperament (b = 0.09, p = 0.008), caregiver BMI (b = 0.26, p < 0.001), desire heavier (b = −0.37, p < 0.001), and desire thinner (b = 0.23, p < 0.001) were associated with child BMIz. Diet was not associated with child BMIz and did not mediate the association of feeding practice patterns and child BMIz (Fig. 1).
Association of Feeding Practice Patterns, Child, Caregiver, and Family Characteristics with Child BMI z-Score (n = 437)
Child care center considered as cluster in all analyses; Child race was excluded in multivariable models due to collinearity; variables significant at p < 0.15 were retained for the parsimonious model; sample size in multivariable models was reduced to 401 cases.
CFI, Comparative Fit Index; RMSEA, Root Mean Squared Error of Approximation; SE, standard error; SRMR, Standardized Root Mean Squared Residual.
Table 3 summarizes the multigroup SEM findings of potential moderators. The association between feeding practice patterns and BMIz was not moderated by child's sex, caregiver race, caregiver education, family poverty level, or food insecurity. However, the interaction term of Regulating feeding practices with caregiver education was significant p = 0.04.
Multigroup Structural Equation Modeling to Examine the Association of Feeding Practice Patterns with Child's BMI z-Score Based on Child's Sex, Caregiver's Race, Family Food Insecurity and Poverty Level, and Education
All the significant variables in the Table 2 parsimonious model are included and held constant to examine subgroup differences in demographic variables of interest.
Discussion
Using an innovative and comprehensive method of conceptualizing feeding practice patterns, this study makes three primary contributions to the understanding of associations between feeding practice patterns and child BMIz. First, Regulating class was associated with lower child BMIz, in comparison to Controlling. Caregivers in both Controlling and Regulating classes endorsed coercive controlling practices. However, Regulating class caregivers endorsed higher autonomy practices, including teaching nutrition, balancing food variety, and encouraging and involving children in food planning and preparation. These practices can empower children by improving their self-regulatory behaviors, which may increase healthy behaviors and decrease obesogenic eating later in life. 13 Autonomy practices can be an important understudied factor in regulating eating behaviors. 30
Second, the results highlight the importance of investigating feeding practices simultaneously. Studies that focus on single feeding practices without considering autonomy support may miss the complete picture. Feeding practices may mediate the association between children's appetite and weight, illustrating the contribution that caregiver feeding practices play. 31
Third, we found a positive association between child temperament, defined by inhibitory behaviors and low self-regulation, and BMIz. This finding is consistent with numerous studies 13 and reviews showing associations between low self-regulation and obesity in toddlers and preschoolers.32,33 For instance, a longitudinal study among children aged 6 months to 11 years showed that school age children with difficult temperaments have an increased risk of having overweight and obesity over time. 34 Self-regulation is modifiable and has become a focus in child obesity prevention programs. 35
Fourth, we found that caregivers' dissatisfaction with child-size was associated with child BMIz. Desire for the child to be thinner was positively associated with child BMIz and desire for the child to be heavier was negatively associated with child BMIz. Although these findings may suggest accuracy in caregivers' perceptions of their child's size, the associations were low and a meta-analysis has shown that most caregivers underestimate their child's size, particularly among children who have overweight or obesity. 36 Caregivers who are dissatisfied with their child's size tend to use controlling feeding behaviors, either encouraging children to consume less or more depending on their perception. 33
In our study, a quarter of caregivers who were satisfied with their child size had children with overweight or obesity. These findings indicate that parent perceptions of healthy child weight need to be further explored for the accuracy of caregivers' perception about child size and their potential influence on both child diet and BMI.
In bivariable models, child age, caregivers' education, and food insecurity were associated with child BMIz. However, they were not significant in the multivariable analysis. Inconsistencies have been found in other studies as well, related to caregiver education,5,37,38 food insecurity,39,40 family and socioeconomic characteristics,5,41,42 and income level. 42 Inconsistencies may be due to differences in study samples, measures, analytical approaches, and inclusion of characteristics.5,42
The absence of moderation and subgroup differences in associations between feeding practice patterns and child BMIz may have been influenced by the relatively small sample size of the Regulating and Balancing patterns. Finally, diet (fruit/vegetable and SSS foods) was not associated with child BMIz and did not mediate the association of feeding practice patterns with child BMIz; Feeding practice patterns were not associated with diet. The lack of associations may be at least partially related to the measurement of diet in this study. The dietary measure focused on fruits and vegetables, and saturated, salty, snacks and junk foods, rather than comprehensive dietary intake. In addition, caregivers may have been unaware of children's intake during preschool. Future investigations of nutrient intake should consider comprehensive methods to measure diet that enable calculation of the Healthy Eating Index. 43
Limitations and Strengths
Other limitations must be acknowledged. As a cross-sectional study, we could not examine temporality. In addition, many caregivers in our sample were in the Controlling group, making the sample size of the Regulating and Balancing group small, limiting the power to detect differences. Although our sample was comparable to the general Maryland population, there were relatively few low-income minority families, limiting the heterogeneity of the sample. We had to collapse many non-White races into one category as the frequency of non-White races other than African Americans was relatively low in our sample. Although this decision was statistically driven, it does not enable us to understand cultural differences.
Future research may benefit from oversampling minorities to have better variance and the ability to explore potential racial differences. Except for child weight and height, all data were caregiver-reported, raising concerns about social desirability and lack of variance. However, using established and validated questionnaires increased the rigor of the investigation.
Strengths of our study include the holistic view of childhood obesity, precisely measured weight and height, and reliable and valid instruments to measure feeding practice patterns, child temperament, and poverty level. Robust statistical methods were used to develop feeding practice patterns and to test the associations in bivariable and multivariable models. In addition, the caregiver sample is diverse and comparable to the population of Maryland. 44 Our study has reinforced the complexity of factors associated with childhood obesity and highlights the role of autonomy in feeding practices.
Conclusion
This study supports the growing evidence of family factors related to childhood obesity. Caregivers' feeding practices, as modifiable behaviors, are likely targets to improve the effectiveness of obesity prevention programs. This study contributes to the understanding of meaningful patterns of feeding practices and their association with childhood obesity. As such, this study exemplifies novel ways of conceptualizing, measuring, and analyzing simultaneous feeding practices. Findings also suggest the importance of autonomy practices, which have the potential to have long-term influence on children's self-regulatory behaviors. 12 Longitudinal research is needed to examine the temporal associations between feeding practice patterns and BMIz, with attention to autonomy-supporting practices, strategies to promote young children's self-regulatory behaviors, and caregivers' perceptions of child temperament and size.
Data Sharing
Protocol of the CHAMP study is published at the Journal of Contemporary Clinical Trials (DOI: 10.1016/j.cct.2019.105849). The deidentified participant data, including all the variables reported in this study and codebooks will be available upon request and signing data use agreement from the principal investigator (PI) of CHAMP study: mblack@som.umaryland.edu for future research studies or upon request for checking the quality of the published study and analysis.
Footnotes
Impact Statement
Feeding practices are modifiable targets of obesity prevention. Using an innovative method of conceptualizing simultaneous feeding practices, the Regulating class was associated with lower child BMI z-score (BMIz) than the Controlling class, suggesting that future obesity prevention research focus on autonomy practices that empower children by improving their self-regulatory behaviors.
Authors' Contributions
Z.R. designed and conducted the study and wrote the drafts as part of her PhD dissertation, in collaboration with her dissertation committee (M.E.J., C.L.S., Y.W., and M.M.B.). M.E.J., C.L.S., and Y.W. provided statistical guidance, and M.E.J. and M.M.B. provided theoretical guidance and supervised the study. All authors reviewed the article, provided critical comments, and approved the final submission.
Acknowledgments
The authors acknowledge all CHAMP families for their participation and members of the CHAMP research team for their contribution to data collection and data management. We also acknowledge Dr. Robyn Gilden for support and feedback on this study. In addition, we acknowledge the University of Maryland School of Nursing's support. This article is part of the first author's PhD dissertation.
Funding Information
CHAMP was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (Grant No. R01 DK107761; PI: M.M.B.). This study was supported by Sigma (Pi at-Large Chapter). The funding bodies were not involved in the design of the study, collection, analysis, and interpretation of data, or in writing of the article.
Author Disclosure Statement
There is no conflict of interest to disclose.