
Abstract
General parenting interventions have improved parent-child relationships and child behavior, with emerging evidence that they may also reduce prevalence of pediatric overweight/obesity. We conducted a systematic review on interventions that were designed to promote positive parenting and examined child weight post-hoc. We searched for studies published through January 2022 that promoted positive parenting among parents of children ages 0–18 years and reported effects on body weight as an ancillary outcome, with no intervention content focused on energy balance (e.g., feeding, physical activity). This search was carried out within ClinicalTrials.gov, ISRCTN Registry, PubMed, PsycINFO, Web of Science, and Connected Papers. Studies were imported into EndNote X9 and assessed independently by two investigators. In total, 753 clinical trials and 723 publications were assessed, and six publications met inclusion criteria. All cohorts were low-income and interventions targeted expectant mothers up through parents of adolescents. Follow-ups occurred when participants were between 2 and 25 years. Significant improvements in weight-related outcomes were observed across all studies for the intervention arm as a whole or for certain subgroups, and reasons underlying these gains tended to differ by participants' age. The magnitude of effect sizes ranged from medium to large. Interventions focused on general positive parenting are efficacious at lowering risk of overweight/obesity without focusing on physical health. Promoting attachments among infants, restructuring a toddler's home environment, praising preschoolers, and communicating with adolescents may optimize weight outcomes in parenting interventions adapted for obesity prevention.
Introduction
According to the data published by the World Health Organization, 39 million children younger than age 5 and more than 340 million children between 5 and 19 years at present have overweight or obesity. 1 For youth, having a BMI ≥85th percentile is particularly problematic since studies show that excess weight elevates risk of medical conditions such as high blood pressure and impaired glucose tolerance, which can intensify over time. Furthermore, these conditions have also been observed to disproportionately affect individuals from minority groups or of lower socioeconomic status.2–4
Given that overweight and obesity are the result of a positive energy balance and are impacted by environmental factors, current clinical practice guidelines have emphasized the importance of improving dietary quality, reducing energy intake, and increasing levels of physical activity for preventing excess weight.5,6 Such approaches, however, have largely failed to yield lasting effects across all demographics,7,8 which suggests that alternative solutions to modify a child's environment are needed. The family is the primary social institution influencing young children, and so, it is plausible that many risk factors for childhood obesity have roots within the family context. Observational data suggest that positive parent–infant relationships, 9 mothers who are highly sensitive and responsive, 10 and parents with a high degree of warmth 11 may be protective against the development of childhood obesity.
Beginning early in life, frequent, high-quality parent–infant interactions are an essential aspect of healthy child development. Robust evidence demonstrates that they enhance infant cognition, aid in verbal comprehension, promote language development, and support school readiness over the shorter term,12–18 and are connected to less depression, a lower likelihood of using substances, and better health in the long run.19–21 Literature on responsive parenting, which involves prompt, contingent, and appropriate responses to a child's cues and awareness of the needs and developmental state, 22 reinforces these findings.23–25 In recent years, obesity researchers have leveraged knowledge from the developmental science literature in this area to evaluate the efficacy of responsive parenting interventions to prevent childhood obesity.26–29
For example, in one of the first randomized controlled trials on responsive parenting for obesity prevention, Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT), 30 parents were taught how to identify and respond sensitively to infant cues (e.g., signs of hunger, fullness, distress) with the goal of supporting healthy weight gain. During infancy, children in the responsive parenting group had less conditional weight gain, lower weight-for-length percentiles, and a reduced chance of being overweight at age 1 year relative to the control group. 31 This intervention also led to a modest decrease in BMI z-scores at 3 years of age, although there were no differences in BMI percentiles between the groups. 32
In the NOURISH randomized controlled trial that used a responsive feeding approach to promote healthy growth in early life, the intervention group had a lower BMI z-score than the control group at 14 months, 33 yet differences between groups diminished by ages 2 and 5.34,35 With respect to research carried out in children of older ages, investigators who led the Parents and Tots Together Intervention found that giving lessons on healthy eating and increasing activity within a parenting program had a positive influence on restrictive feeding but not BMI at the 9-month follow-up. 36
Many efforts to bring together parenting and obesity prevention have focused on messages specifically about feeding, eating, and/or physical activity or integrated these into existing parenting programs for obesity (e.g., PCIT-Health, 37 Lifestyle Triple P's health-related version 38 ). For this review, we were interested to see whether general parenting interventions were capable of lessening obesity risk without relying on weight-related content, given the evidence of their widespread benefits on child development. Studies have shown, for instance, that children and adolescents who receive these interventions experience enhanced socioemotional development and self-control, as well as exhibit fewer problem behaviors (e.g., substance use/abuse, risky sexual activity). When examining the impacts of these general positive parenting interventions on weight as a secondary outcome, there is emerging evidence that these interventions confer lasting protection against unhealthy weight gain—even for children from diverse disadvantaged homes.39–44 As such, implementing these evidence-based interventions could potentially have broad-based effects and reduce the need to modify existing parenting programs from the developmental science literature.
In this systematic review, we evaluated general responsive or positive parenting interventions that did not target child energy balance (e.g., feeding, eating, physical activity) or position child weight as a primary outcome of interest but assessed it as a secondary outcome after the fact. Studies on children ages 0–18 years were considered relevant given a paucity of literature in this area of interest. We aimed to describe the specific content of general parenting interventions that were efficacious in preventing weight gain throughout the childhood years and identify individuals who benefited the most, so as to inform future research and programming on parenting and childhood obesity.
Methods
Search Strategy
We conducted an initial electronic search from February 2021 to June 2021, followed by a full search from December 2021 to June 2022 within the ClinicalTrials.gov, ISRCTN Registry, PubMed, and PsycINFO electronic databases. Search terms for the clinical trials' websites consisted of “childhood obesity,” while search terms for the biomedical literature websites included variations of “parenting,” “infant,” “child,” “intervention,” “RCT,” and “weight gain” (see Appendix A1 for the full search strategy). The R package, “citationchaser,” was used to identify any potentially relevant articles by listing all of the articles that had cited studies we identified as relevant from the abovementioned electronic databases. 45 There was no exclusion criterion related to article publication date; identified studies were published beginning in 1987 and all were imported into EndNote X9 library for review.
In January 2022, a supplementary search was conducted by two additional investigators (H.I.W. and K.H.) to identify any additional articles that met the inclusion criteria using Web of Science and the Connected Papers websites. 46 Connected Papers identifies articles that are similar to a user-provided article based on overlapping references and citations. For this search, each article that met the inclusion criteria during the primary search was entered into Connected Papers to identify similar articles.
Eligibility Criteria
Studies were eligible for inclusion if they: (1) were published in an academic, peer-reviewed journal and written in English, (2) were a randomized controlled trial promoting positive or responsive parenting that did not target child weight as an a priori, primary outcome and used quantitative or mixed methods, (3) targeted parents or primary caregivers of children anywhere between infancy through adolescence (0–18 years of age), and (4) reported on at least one weight-related outcome in children (e.g., BMI, weight gain trajectories, fat mass percentage) as a secondary outcome that was assessed later. 42 Studies were excluded if child weight was a prespecified primary outcome and/or the intervention focused on improving a child's energy balance (e.g., providing instruction on adhering to a healthy diet, increasing physical activity). Meta-analyses, narrative reviews, dissertations, and book chapters were also excluded.
Data Extraction
Two investigators (B.B. and C.S.) independently screened the list of clinical trials and publications in the electronic databases that emerged using the above search strategy. In total, 753 clinical trials and 723 publications were assessed (Fig. 1). Of these, 752 clinical trials and 712 publications had descriptions or abstracts, respectively, containing information pertaining to diet and/or physical activity, positioned child weight as an outcome of interest, or were not a parenting intervention and thus were excluded. For the remaining clinical trial and 11 publications that appeared relevant, further inspection found that the trial is ongoing and three of the publications had content that targeted diet and/or physical activity.
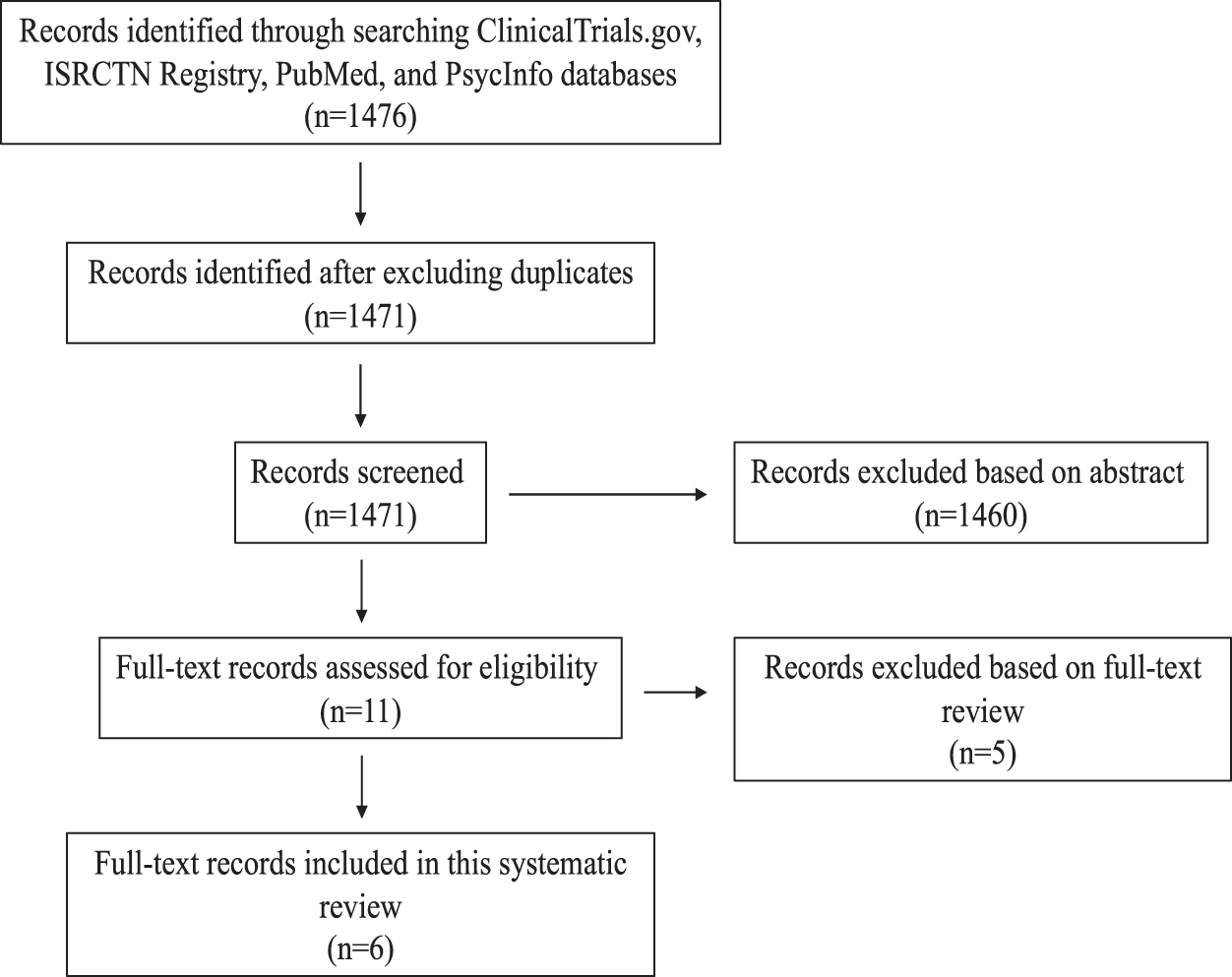
For the remaining eight publications of interest, B.B. and C.S. proceeded to discuss the (1) study design, (2) intervention characteristics, (3) participant characteristics, and (4) outcomes with a third investigator (K.K.) to arrive at a consensus over which ones met the inclusion criteria of the present study. Following this discussion, two studies were deemed irrelevant to our topic because their interventions were integrated into primary care visits (and therefore violated the criterion prohibiting discussion of energy balance during the intervention visits), rendering us a total of six studies for our systematic review. The supplementary search conducted by H.I.W. and K.H. yielded no additional relevant articles.
Results
General Study Characteristics
General study characteristics and participants' sociodemographic variables can be found in Table 1. We report on the six eligible interventions, which were evaluated across seven sets of analyses, resulting in seven unique samples described within six articles (i.e., one of the six interventions was tested in two different samples). All investigations were published within the past decade and took place in the United States. All interventions were randomized controlled trials, consisted of an experimental group and a control group, and were conducted between 1997 and 2016. Various data points were collected at baseline and follow-up visits occurred between 1 month and 14 years postintervention. Approximately 73%–99.4% of individuals enrolled in the intervention were present at follow-up(s) among studies that reported dropout rates,41–44,47,48 yet one consisted of a selected cohort that had been reduced in size because of budget issues. 43 When comparing attrition rates between the experimental and control groups, the five studies that reported details found no significant differences between the two.42–44,47,48
General Study Characteristics and Participants' Sociodemographic Variables *
Interventions are listed according to the age of their participants, starting with infants and ending with adolescents.
ABC, Attachment and Biobehavioral Catch-up; DEF, developmental education for families; FCU, Family Check-Up; MTB, Minding the Baby; NYC, New York City; RCT, Randomized Controlled Trial; SAAF, Strong African American Families.
With regard to participants' sociodemographic variables, the total number of children in each study was between 99 and 998. Child age at baseline ranged from being in the third trimester in utero to 12 years of age. The percentage of males was 44%–54.4%. Given that body weight was not a primary measure of interest, only two investigations assessed it at baseline, and neither of these found any differences between the experimental and control groups.41,42 Five samples consisted predominantly of minority groups,42–44,47,48 whereas two had 42.4%–50.1% of participants self-identifying as European American and the remainder of their cohorts were from various ethnic backgrounds.40,41
Of those that included information on the parents' education levels, four indicated that 48%–72.5% of parents only had a high school education,43,44,47,48 and one reported that most mothers did not complete schooling beyond their junior year of high school. 42 The average income for families in all seven cohorts was low, and many lived at or below the federal poverty line.40–44,47,48 Frequencies of single-parent households ranged from 30% to 86%,41–44,47,48 with this variable not reported in one study. 40 Two studies also had children who were especially high risk—either having a history of involvement in Child Protective Services or an older adjudicated sibling.44,47 Finally, there were no group differences in demographic variables noted at baseline between families in the intervention and control groups,41,42,44,47,48 except for Brody et al. 43 who noted that parents in the experimental arm had lower incomes than controls; Smith et al. 40 did not provide data on this topic.
Intervention Descriptions and Nonweight-Related Outcomes
Description of the interventions can be found in Table 2. Interventions comprised 3–90 sessions that were 3.5–27 months long; sessions for younger children were usually more frequent and occurred over a longer time period than those for older children. Since the primary goal of these investigations was to improve parenting practices, many were exclusively aimed at parents.40–42,44 For studies that also gave educational sessions to children (n = 3), these were separate but always complemented those given to parents and were followed by interactive sessions in which parents and children could practice their new skills with each other.43,47,48 Personnel who delivered the interventions included video narrators, coaches, psychologists, doctoral candidates, social workers, prekindergarten teachers, educational assistants, family workers, pediatric nurses, and therapists.
Intervention Descriptions
WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
For the following paragraphs, we provide a brief description of each intervention, starting with those implemented in early childhood followed by later childhood. To begin, Ordway et al. devised Minding the Baby (MTB) program, which uses interdisciplinary tactics to promote maternal reflective functioning (i.e., a mother's ability to understand her infants' thoughts, feelings, and desires), boost the mental and physical health of first-time mothers, as well as foster secure attachments and development of their newborns. 42 Here, a nurse and social worker would visit an expectant mother's home weekly or biweekly, beginning in their third trimester and going up through the child's second birthday.
Since its inception in 2002, the MTB has been implemented across the United States and parts of Europe with outcomes that include, compared with controls, reductions in externalizing behavior problems (e.g., aggression and poor attention) in children 1–3 years after the intervention, 49 and a decreased likelihood of mental health issues and hostility in mothers 2–8 years poststudy. 50 Since November 2021, MTB has been recognized as 1 of 21 effective home visiting interventions by the US Department of Health and Human Services due to its favorable impact on child and maternal health. 51
Bernard et al. 44 conducted the Attachment and Biobehavioral Catch-up (ABC) program, which focuses on strengthening bonds between infants younger than 24 months and their caregivers and developing infant self-regulation. More specifically, qualified home visitors and supervisors would meet with families once a week for 10 weeks, first giving parents lessons on nurturing their infant in times of stress and being sensitive to their needs, and then observing parent–child interactions to provide feedback. This program was founded initially to address the needs of infants in foster care, although it has since expanded to infants and toddlers from various sociodemographic backgrounds and in multiple continents.
ABC has also been profiled by the US Department of Health and Human Services as an effective home visiting program on account of its ability to significantly enhance child health, development, and school readiness, as well as positive parenting practices,1,52 and a handful of studies have shown that it increases the development of inhibitory control among at-risk children,53,54 improves sensitivity and decreases depression in parents, 55 leads to secure child attachments that are sustained for at least 8 years, 56 as well as promotes speech and executive functioning development in toddlers.57,58
Two parenting interventions that focused on early childhood were the Incredible Years Series and ParentCorps.47,48 Both targeted families with preschoolers and were founded on evidence that early positive parenting might be protective against behavioral issues and poor social skills manifesting in later childhood.59–62 In the Incredible Years Series, 47 parents were educated on engaging with children, using appropriate disciplinary tactics, and acknowledging positive behaviors, while their preschoolers met with therapists to learn about conflict resolution, empathy building, and problem solving. Following their respective sessions, parents and children partook in arts and crafts or free-play activities with each other to exercise the aforementioned techniques. In ParentCorps, 48 parents were advised to create predictable home environments, enact gentle discipline (e.g., time-out), and praise obedience, whereas children became acquainted with such practices from group leaders. Additionally, the children's teachers were educated on how to enhance socioemotional learning in the classroom. Blueprints for Healthy Youth Development, an organization that assesses the effectiveness of pediatric interventions each year, has deemed the Incredible Years Series to be a “Promising” program 63 because preliminary research reveals it improves conduct problems in children over the shorter term.64,65 ParentCorps is regarded as a “Model” program 63 since trials using it have demonstrated gains in parenting practices and child behavior and academic performance that have been maintained at 12-month follow-ups.47,48,66
Brody et al. 43 carried out the Strong African American Families (SAAF) program in a cohort of 11-year-old African American children, nearly half of whom lived below the federal poverty line. This intervention drew on evidence for critical parenting behaviors that protect against the emergence of risky behaviors in youth from impoverished backgrounds. 67 Over the course of 7 weeks, educators played videos showing healthy family dynamics (e.g., parents reacting warmly, enacting consistent discipline, establishing routines at home) and then had families put such skills into practice. Over 29 months, relative to controls, children exposed to SAAF were less prone to steal, drink alcohol, have sex, or be absent or suspended from school, and parents exposed to SAAF were more inclined to communicate openly about risky behaviors and their expectations.68,69 Blueprints for Healthy Youth Development considers it to be a “Promising” program. 63
Two teams of investigators evaluated the Family Check-Up (FCU) intervention, targeting 2- and 12-year olds, respectively.40,41 For both, the FCU consisted of an interview with the family, followed by an assessment of the home environment videotaping family interactions, and ended with a feedback session in which a therapist pointed out positive parenting practices and gave suggestions for boosting communication and involvement in the child's life. Importantly, advice was always customized to each family. Of note, concerning treatment for controls, these individuals continued to receive standard services offered by the child's pediatrician, school, or Special Supplemental Nutrition Program for Women, Infants, and Children,40–42,47,48 were instructed on activities promoting infants' development that did not concern attachment, 44 or were mailed content on development during adolescence and ways to handle stress. 43 FCU for toddlers, in particular, is recognized by Blueprints for Healthy Youth Development as “Promising,” 70 on the basis of literature showing that within the intervention arm 2–5 years later, children exhibited fewer problematic behaviors (e.g., aggression and defiance) and depression, and mothers became happier and more involved in their children's lives when compared against control counterparts.41,71
Weight-Related Outcomes from the Interventions
Results of secondary analyses of intervention impacts on weight outcomes are presented in Table 3. Overall, there were consistent findings that these general positive parenting interventions were linked to a lower subsequent weight status, although not every analysis yielded statistically significant main effects (i.e., impacts were only evident in subgroups for a few studies). In the ABC program, an indirect effect on weight was observed as children who had developed secure attachments to their caregivers had a lower BMI at age 4 than those who had not developed secure attachments. 44 Combined analyses on data from the Incredible Years Series and ParentCorps showed that children in the experimental conditions had lower BMI z-scores and body size ratings than controls at follow-up ages [10.88 years (standard deviation, SD = 1.51) for the Incredible Years Series; 7.77 years (SD = 0.31) for ParentCorps]. 39
Primary Outcomes and Indirect Weight Outcomes of Interventions
95% CI, 95% confidence interval.
As for ParentCorps alone, more than half in the control group had obesity, whereas less than a quarter in the intervention group had obesity. For the FCU intervention implemented in toddlerhood, BMI z-scores were assessed, with a trend toward significance in the program's efficacy to offset unhealthy weight gain [i.e., having an overweight (BMI >1 SD above the WHO growth standard median) or obese (BMI >2 SD above the WHO growth standard median) status] by 9.5 years of age. 40 The FCU intervention implemented in adolescence used BMI scores, and findings showed that treatment improved the quality of parent–youth relationships. This favorable outcome predicted a reduction in maladaptive eating and led to a reduced odds of obesity [odds ratio (OR) = 0.98, 95% confidence interval (95% CI): 0.96 to 0.99, p < 0.05] at 22 years of age. 41 Interestingly, in the SAAF study, just the females who had received the intervention exhibited a leaner BMI at ages 19–25 years. 43 As well, only Hispanic participants in the MTB program experienced significant protection from developing obesity at age 2, as assessed using BMI z-scores. 42
Upon calculating effect sizes, analyses reporting on BMI differences between the intervention and control arms at follow-up assessments occurring 6 and 4 years later, respectively, for the Incredible Years Series and ParentCorps yielded a Cohen's D of 0.62 and 0.5139,44; a Cohen's D of 0.66 was already calculated by investigators of the ABC program when children were 4 years of age. 44 Analyses reporting participants' odds of obesity following the FCU for toddlers, FCU for adolescents, and MTB program, respectively, after 7, 10, and 2 years yielded a Cohen's D of 0.30, 1.17, and 0.93.40–42 On average, the magnitude of the effect sizes in these studies was medium to large.39–42,44 There were insufficient data from the SAAF intervention to determine an effect size. 43
Of note, it is worth highlighting that three interventions explored mediators of children's body weight outcomes. Specifically, Smith et al. 40 and Van Ryzin and colleagues 41 found that the FCU program was indirectly associated with lowered risks of excess weight. Data by Smith et al. 40 showed that boosting caregivers' positive behavior support led to them serving more nutrient-rich meals (i.e., a diversity of food groups that included fruits and vegetables) to their toddlers, and this was connected to a healthier BMI in midchildhood. Relatedly, Van Ryzin and colleagues 41 mentioned that improving the relationship quality between parents and adolescents was predictive of less maladaptive eating (e.g., binging, purging, preoccupation with dieting or body image), which in turn was associated with a decreased likelihood of obesity in early adulthood.
On the contrary, Brody et al. 43 remarked that prevention of obesity among their female participants was not attributed to shifts in the SAAF program's targeted parenting practices. Pathway analyses conducted by that group showed that enhancements to parental emotional support and communication about youth behavior, use of nonharsh parenting tactics, and a routinized home environment were not linked to a healthy BMI in females.
Discussion
Interventions promoting general responsive or positive parenting have consistently been shown to enhance cognitive, socioemotional, and behavioral outcomes in children, which is why several of these interventions are being utilized across cultures and within a variety of contexts worldwide. 72 The current review aimed to summarize the current evidence base when examining general parenting interventions that did not target weight as a primary outcome but have examined potential collateral benefits on child weight as a secondary outcome. Six interventions met the inclusion criteria for this review, and all demonstrated medium-to-large intervention effects on at least one weight-related measure across seven sets of analyses, with two only doing so in a subgroup of participants. In addition, all of these interventions were carried out among diverse (>50% minority) and low-income households.
On the whole, all six interventions were effective at improving their primary targeted variables of interest. Results showed that parents increased in becoming more sensitive toward their children,41,47,48,68 creating stimulating environments, 47 monitoring children's whereabouts, 68 communicating,42,68 implementing rules, 68 and enacting developmentally appropriate discipline and positive behavior support.40,47,48 Children, in response to either their parents' newly acquired skills or parents' skills plus child-centered lessons, displayed more secure attachments or obedience to parents,42,44,47,48,68 heightened social competence, 47 unfavorable views on and less partaking in activities such as unsafe sex and premature/excessive drinking, 68 as well as had less aggression,47,48 depression, and maladaptive eating. 41 In the following paragraphs, we delve deeper into some of the parenting and child behavior variables impacted by these interventions that may explain the collateral and lasting benefits on physical health.
To begin, positive parenting interventions in this review boosted caregiver sensitivity41,47,48,68 and attachment quality between the parent and child,42,44 and prior longitudinal research supports the idea that these impacts might be linked with weight outcomes. For example, the Early Childhood Longitudinal Study (n = 6650) found that 24-month-olds with insecure attachments had a 1.30 (95% CI: 1.05 to 1.62) higher odds of having obesity at 4.5 years of age compared with matched counterparts, 9 and the Study of Early Child Care and Youth Development (n = 977) found that experiencing both insecure attachment and low maternal sensitivity at 2 and 3 years of age was linked with a heightened likelihood of having obesity at age 15 years. 10 In view of these outcomes, one possible explanation is that caregivers, in boosting attentiveness to their children, grew more attuned to their child's needs within the feeding domain (e.g., hunger and fullness). In addition, another potential reason may be that secure children are likely to be less stressed or anxious relative to those who are insecure, thus making them less prone to seek comfort through food. One study evaluating attachment priming in 6- and 7-year-olds noted that showing social support pictures before frightening pictures helped buffer feelings of fear and stress, and that children who displayed the lowest levels of stress also had secure attachments to their parents. 73 These feelings may protect against accelerated weight gain because one investigation found that higher attachment to caregivers correlates negatively to the consumption of energy-dense foods. 74
As well, some interventions encouraged parents to set limits and developmentally appropriate expectations.40,47,48,68 Of the four types of parenting styles, parents who are authoritative are recognized as being warm and nurturing, but also use rules and reasoning to enact structure at home. 75 Providing structure to a child's environment may be especially protective against excess weight, as the Structured Days Hypothesis holds that an environment overseen by adults consisting of appropriate and scheduled or intentional activities (e.g., set meal, sleep, and exercise times) helps prevent children from engaging in obesogenic behaviors.76,77 In a cross-sectional study on 8550 4-year-olds living in the United States, those who consistently ate evening meals with their family, received a sufficient amount of sleep at night, and partook in limited screen time had ∼40% reduced prevalence of obesity compared with children who did not engage in any of these routines. 78
From a longitudinal investigation on the UK Millennium Cohort, analyses showed that 3-year-olds who did not have a regular bedtime were more likely to have obesity at age 11 relative to those who did. 79 In addition, two systematic reviews have reported that offspring of authoritative parents eat healthier 80 and have lower BMIs80,81 than children raised in authoritarian, permissive, or uninvolved households. Altogether, interventions that promote an authoritative parenting style may lead to healthier BMIs in children by exposing them to healthy eating and activity routines.
Lastly, increases in various aspects of executive function were observed across multiple studies. Executive function is defined as cognitive processes involved in the regulation of behaviors, emotions, and thoughts for achieving future goals, 82 and with respect to the field of obesity, this can include limiting energy intakes and engaging in physical activity for weight loss or maintenance. 83 Systematic reviews report that children with overweight or obesity often have lower levels of executive function in comparison with those of a healthy weight,83–85 indicating that boosting it may be advantageous for obesity prevention and treatment.86–89 Here, it seems that success of the responsive or positive parenting interventions was due, at least in part, to strengthening executive functioning and/or its correlates. The MTB and ABC programs promoted infant mental health and self-regulation,42,44 children who participated in the Incredible Years Series and ParentCorps showed a reduction in externalizing behaviors,47,48 which associate with possessing self-regulatory skills, 90 and youth who received the SAAF or FCU intervention exhibited a reduced likelihood of partaking in risky/harmful behaviors,41,43 thereby putting them on the path toward achieving future goals or aspirations.
Of all the studies discussed in this review, three reported on exploring mediators underlying the linkage between effects of the intervention and children's weight outcomes. Smith et al. 40 and Van Ryzin and colleagues 41 demonstrated that effects of the FCU intervention were indirectly associated with lowered risks of excess weight. It is notable that although feeding and physical activity were never targeted, these FCU studies both showed that improvements in dietary intakes and eating behavior were responsible for the positive influence on child weight. This indicates that maintaining energy balance is still critical for achieving a healthy BMI during the formative years, yet efforts to accomplish this may be more successful when an intervention's focus is directed more globally toward parenting. However, for Brody et al., 43 obesity prevention among females was not attributed to shifts in the selected parenting practices. Since this team did not evaluate whether changes in supportive parenting might influence a child's eating or exercise habits, in contrast to Smith et al. 40 and Van Ryzin and colleagues, 41 it is plausible that providing emotional support, using nonharsh parenting, having a routinized household, and communicating about behavioral expectations may have indirectly benefited the female participants' body weights and warrants further investigation into how responsive parenting interventions affect a child's lifestyle behaviors.
Burgeoning research attests to the importance of beginning prevention or treatment of pediatric obesity during the early years91,92; however, findings from this review demonstrate that implementing responsive or positive parenting interventions anytime from 0 to 12 years of age may have a substantial impact on later body weight. Yet, the specific approach toward promoting positive parenting should still be mindful of one's developmental period. In looking to features of the interventions that were most contributory toward our outcomes of interest, we observed that in infancy, being nurturing, sensitive, and attuned to a baby's needs promoted secure attachments, which led to a lower BMI in early childhood.42,44 In toddlerhood, restructuring the home environment for healthy development improved the nutrient quality of meals, and benefits were maintained into midchildhood. 40 During the preschool period, enacting appropriate discipline, giving praise, and establishing structure fostered social competence, resulting in a healthy weight in midchildhood. 39 Finally, in adolescence, parent–child communication about behavioral expectations and setting limits prevented youth from engaging in harmful activities, which was reflected in a reduced likelihood of carrying excess weight in adulthood.41,43
The limitations and strengths of the studies included in the current review should be acknowledged. Regarding limitations, this line of research is still in its infancy as only six studies were relevant for inclusion here, with heterogeneity in the cohorts' sociodemographics. Interventions commenced when participants were in utero to age 12 and impacts on body weight were evaluated between 2 and 25 years of age. Hence, additional investigations are needed to understand the ability of responsive or positive parenting interventions to benefit child weight more broadly and provide insight into reasons underlying the heterogeneous findings. It has been reported that a child's weight and height trajectories, respectively, correlate closely to the maternal BMI and paternal height up through 5 years of age 93 ; therefore, data on parental anthropometrics might help explain why some of our weight-related outcomes differed according to participants' ages. As well, considering that several studies did not obtain children's BMI at baseline because it was not an initial variable of interest,40,43,44,47,48 the magnitude of the programs' influence on child weight should be interpreted with caution. Concerning strengths, five samples consisted predominantly of ethnic minority groups—populations that have historically been underrepresented in the broader parenting literature. Furthermore, all of the studies had control groups, so an effect of the intervention on child weight could still be discerned without pre–post data. Also, follow-ups occurred 2–14 years after treatment; this demonstrates the potency of these interventions to prevent obesity through developmental transitions and into periods in which children have increased autonomy and independence to make their own decisions. Lastly, all of the studies except the one by Van Ryzin and colleagues 41 reported on objective measurements of participants' BMIs in the secondary analyses, thereby affirming the validity of the programs' meaningful influence on weight-related measures.
Please refer to the PRISMA 2020 Abstract Checklist and PRISMA 2020 Checklist for further details on the transparency of this systematic review.
Conclusions
In conclusion, interventions taking a holistic approach to improve parent–child relationships, rather than focusing on physical health, were successful at lowering future risk of overweight/obesity. These interventions were conducted among diverse cohorts and some high-risk families, underscoring the potential of leveraging existing evidence on promoting positive parenting to support healthy growth.
Footnotes
Authors' Contributions
K.K.: conceptualization, methodology, and writing—original draft, and review and editing; S.A.-F.: conceptualization, methodology, and writing—review and editing; B.B.: methodology, writing—original draft, and writing—review and editing; C.S.: methodology and writing—original draft; H.I.W.: methodology and writing—review and editing; K.H.: writing—review and editing.
Registration and Protocol
This systematic review has not been registered, nor has a protocol been prepared.
Data Availability
Data extracted from included studies; data used for all analyses; analytic codes; any other materials used in the review will be made available to researchers who provide methodologically sound proposals. All proposals should be sent to: kkong@cmh.edu
Impact Statement
Interventions taking a holistic approach to improve parent–child relationships, without focusing on physical health, have a lasting impact on pediatric obesity prevention. Importantly, these interventions were proven effective among children from diverse cohorts and high-risk backgrounds.
Funding Information
This work was funded by grant R01 HD087082 from the National Institute of Child Health and Human Development, awarded to Dr. Kai Ling Kong. This sponsor had no participation in the execution of this work or in the decision to submit the article for publication.
Author Disclosure Statement
No competing financial interests exist.
Appendix A: Full Search Strategy
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.