
Abstract
Background:
Childhood obesity has increased globally during the past four decades. Food insecurity could heighten the risk of obesity. However, little is known about the underlying mechanism. This study aims to investigate the mediating role of sleep duration in the association between food insecurity and childhood obesity and whether there are differences by age, sex, and race/ethnicity.
Method:
Data from the National Survey of Children's Health for the years 2016–2020 were used, including children 10–17 years of age. We employed causal mediation analysis within a counterfactual framework to decompose the total effect of food insecurity into natural direct and indirect effects and estimate the proportion mediated.
Result:
The prevalence of obesity was 15.8% in our study sample. Children with food insecurity had 78% higher odds [odds ratio (OR) = 1.78, 95% confidence interval (CI): 1.70–1.86] of having obesity compared with children who were food secure. Overall, only 6.13% of this association was mediated by sleep duration. The association between food insecurity and obesity was stronger in females (OR = 1.96, 95% CI: 1.84–2.10) than males (OR = 1.66, 95% CI: 1.56–1.75), but the proportion mediated by sleep duration was larger in males (7.13%) than females (5.22%). Evidence of mediation was more pronounced in children 10–11 years of age and non-Hispanic Asian children (proportion mediated = 14.85% and 11.21%, respectively).
Conclusion:
Food insecurity is associated with an increased prevalence of obesity among children. Although a small proportion of this association is mediated by sleep duration, these results suggest that sleep should be considered when assessing the link between food insecurity and childhood obesity.
Introduction
The prevalence of childhood obesity has increased globally during the past four decades. 1 From 1975 to 2016, obesity rates in children and adolescents increased from <1% to nearly 8% in boys and 6% in girls. During the same period, obesity in 5–19-year-olds rose more than 10-fold globally. 2 In the United States, 18.5% of children and adolescents are affected. The age group of 12–19 years exhibits the highest prevalence. 3 Childhood obesity can adversely affect children's physical health and mental health, including social interaction, emotional wellbeing, and self-esteem. 4 It has been linked to numerous medical conditions such as cardiovascular disease, diabetes, and cancer.4,5
Food insecurity, defined as a lack of consistent access to enough food for an active and healthy life, is also a prevalent public health concern. 6 The current COVID-19 pandemic has exacerbated the food insecurity burden. 7 Approximately 17 million US children experienced food insecurity in 2020. 8 Food insecurity increased the risk of obesity but the mechanisms and pathways underlying the relationship are not clear.6,9,10 Additionally, food insecurity can be a profound source of stress, which may increase the risk for sleep problems. Individuals experiencing food insecurity are at increased risk of poor sleep outcomes.11–13 Furthermore, sleep duration has been linked to childhood obesity. Studies have shown that children who slept for shorter or insufficient duration had a significantly increased risk of being affected by obesity, compared with those who slept for sufficient durations.14–16
Recent research has found that sleep partially mediates the association between food insecurity and obesity among adults.17,18 Narcisse et al. noted differences by race/ethnicity in their mediation analysis. 18 Another study found that the combination of physical inactivity, insufficient sleep duration, food insecurity, and income inequality explained 53% of obesity rates in US adults. 19 Only one study involved a pediatric sample but reported a null finding of mediation. 20 Whether sleep duration could explain the association between food insecurity and obesity among children has not been fully investigated. The age range of 10–17 is crucial to child development and required more attention. Changes in life, including puberty, increased school workload, and screen time that occurred at this age also interfere with sleep duration and quality.21,22 This study aimed to investigate the potential mediating role of sleep duration in the association between food insecurity and childhood obesity and whether there are differences by age, sex, and race/ethnicity.
Methods
Data Source and Study Population
The study analyzed the publicly available version of the National Survey of Children's Health (NSCH) for the years 2016–2020. The NSCH was designed to generate national and state-level representative prevalence estimates for a variety of children's health indicators.23,24 Parents from randomly selected households with one or more children under the age of 18 received a mailed invitation asking for participation online or through mail. Questions covered a variety of areas relating to children's physical and psychological health and quality of care received, as well as determinants of health in the context of family, community, and school. 23 Each selected child for whom an interview was completed was assigned a weight.
The child's weight was composed of a base sampling weight, adjustments for both screener and topical nonresponse, an adjustment for the selection of a single child within the sample household, and adjustments used to control the population counts for various demographics obtained from the previous year's American Community Survey (ACS) data. 25 The national weighted interview completion rate varied between 69.7% in 2016 and 81.2% in 2020.25,26 A total of 174,551 children 0–17 years of age were surveyed for the years 2016–2020. Children with available information on the outcome (10–17 years of age), exposure, and covariates of interest were included in the present analysis.
Outcome
The outcome of interest was obesity. In the NSCH, BMI was calculated based on parents' reporting of their child's height and weight. CDC sex-specific BMI-for-age categories are provided in the NSCH dataset. In this study, obesity status was dichotomized. Individuals were classified as either without obesity (<95th percentile for BMI) or with obesity (≥95th percentile for BMI) for children of the same age and sex.27,28
Exposure
Food insecurity was the exposure of interest. In the survey, primary caregivers were asked: “Which of these statements best describes the food situation in your household in the past 12 months?” The response options were: “1 = we could always afford to eat good nutritious meals,” “2 = we could always afford enough to eat but not always the kinds of food we should eat,” “3 = sometimes we could not afford enough to eat,” and “4 = often we could not afford enough to eat.” Following the recommendation of previous studies,29,30 respondents having any of the latter three responses were considered as experiencing food insecurity. Respondents who indicated that they could always afford to eat good, nutritious meals were classified as food secure.
Mediator
We investigated whether sleep duration mediated the relationship between food insecurity and obesity. Sleep duration was based on the parent response to the question “during the past week, how many hours of sleep did this child get on most weeknights?”
Covariates
We employed a directed acyclic graph (Fig. 1) to identify a minimally sufficient set of covariates to adjust for the total effect of food insecurity on obesity. These covariates included age, sex, race/ethnicity, education, and poverty ratio. Age was categorized into four groups: 10–11, 12–13, 14–15, and 16–17. The race/ethnicity of the selected child included five groups: non-Hispanic White, non-Hispanic Black, Hispanic (of any race), non-Hispanic Asian, and non-Hispanic other, which included American Indian or Alaska Native, Native Hawaiian and Other Pacific Islander, some other race, two or more races. An adult with the highest education in the family was used for education, which was categorized as less than high school, high school/general education development, some college, and college graduate or higher. The poverty level was categorized as below the federal poverty line (<100%) and at or above the federal poverty line (≥100%). Based on prior studies,17,18 physical activity was assumed to be on the causal pathway between food insecurity and obesity; therefore, we did not adjust for physical activity in the main analysis. All variables were self-reported by the primary caregiver.
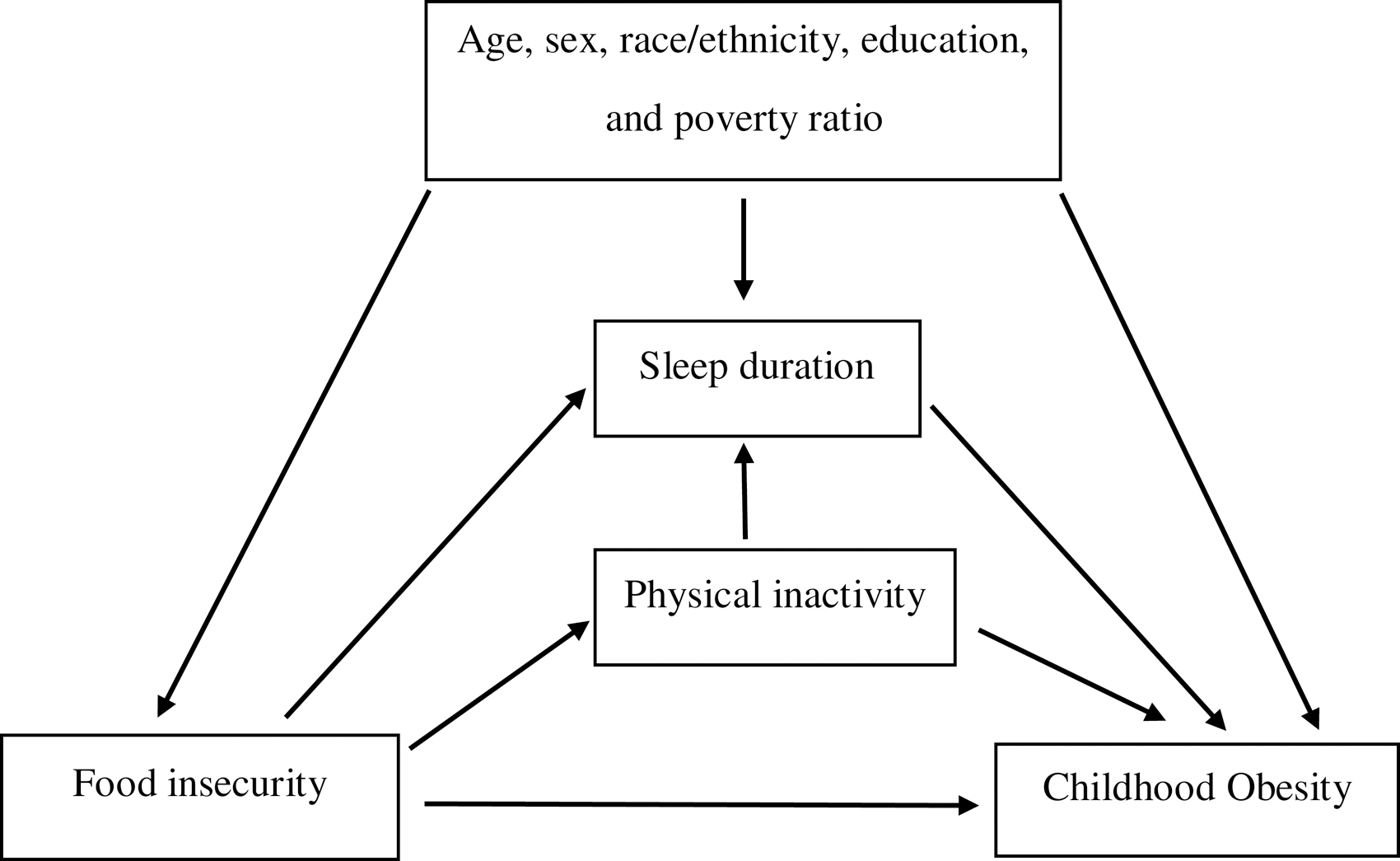
Directed acyclic graph illustrating the association between food insecurity and childhood obesity.
Statistical Analyses
Sample characteristics were compared between children with and without obesity using the chi-square test. The trends in the prevalence of food insecurity, sleep duration, and obesity from 2016 to 2020 were assessed. In mediation analyses, we aimed to assess mediation and quantify the degree to which sleep duration mediated the association between food insecurity and obesity, adjusting for the confounders identified. Utilizing causal mediation analysis within a counterfactual framework, we decomposed the total effect of food insecurity into natural indirect and direct effects. The natural direct effect is the effect of food insecurity on obesity through pathways that do not involve sleep duration while sleep duration is allowed to vary. The natural indirect effect represents the effect of food insecurity on obesity due to the effect that food insecurity has on sleep duration. The logit link was used for the outcome and the identity link for the mediator. The mediated proportion was computed as the natural indirect effect divided by the total effect, and the 95% confidence interval (95% CI) was estimated by repeating 1000 bootstrapped computations. We included cross-product terms for the exposure and mediator but there was no significant interaction.
In a sensitivity analysis, we further adjusted for physical activity, which we did not include in the main analysis. Furthermore, we restricted the analysis to the respondents who answered “1 = we could always afford to eat good nutritious meals” and “4 = often we could not afford enough to eat” to the food security question. We repeated the analysis with a dichotomized sleep duration (inadequate sleep duration and adequate sleep duration) based on the American Academy of Sleep Medicine recommendation. 31 Inadequate sleep duration was defined as sleep duration <9 hours per day in children 10–12 years of age, and <8 hours per day in children 13–17 years of age. In all analyses, the level of statistical significance was set at p < 0.05. The percentages in the descriptive statistics were weighted to account for the multiple-stage sampling design. The analysis was performed in SAS® 9.4 software (SAS Institute, Inc., Cary, NC).
Results
A total of 85,003 children 10–17 years of age were included in this analysis. The weighted prevalence of food insecurity, inadequate sleep duration, and obesity were, 33.1%, 36.0%, and 15.8%, respectively. The trend from 2016 to 2020 remained constant (Fig. 2). The mean sleep duration was 8.2 hours (standard error = 0.009). Table 1 shows weighted obesity prevalence by the participant's characteristics. Obesity was more prevalent among males and decreased with increased age, physical activity, parent's educational attainment, and income. Non-Hispanic Black (23.1%) and Hispanic (20.5%) children were the racial/ethnic groups with the highest prevalence of obesity. Obesity was most common in children with food insecurity (23.0%) and inadequate sleep duration (19.9%).
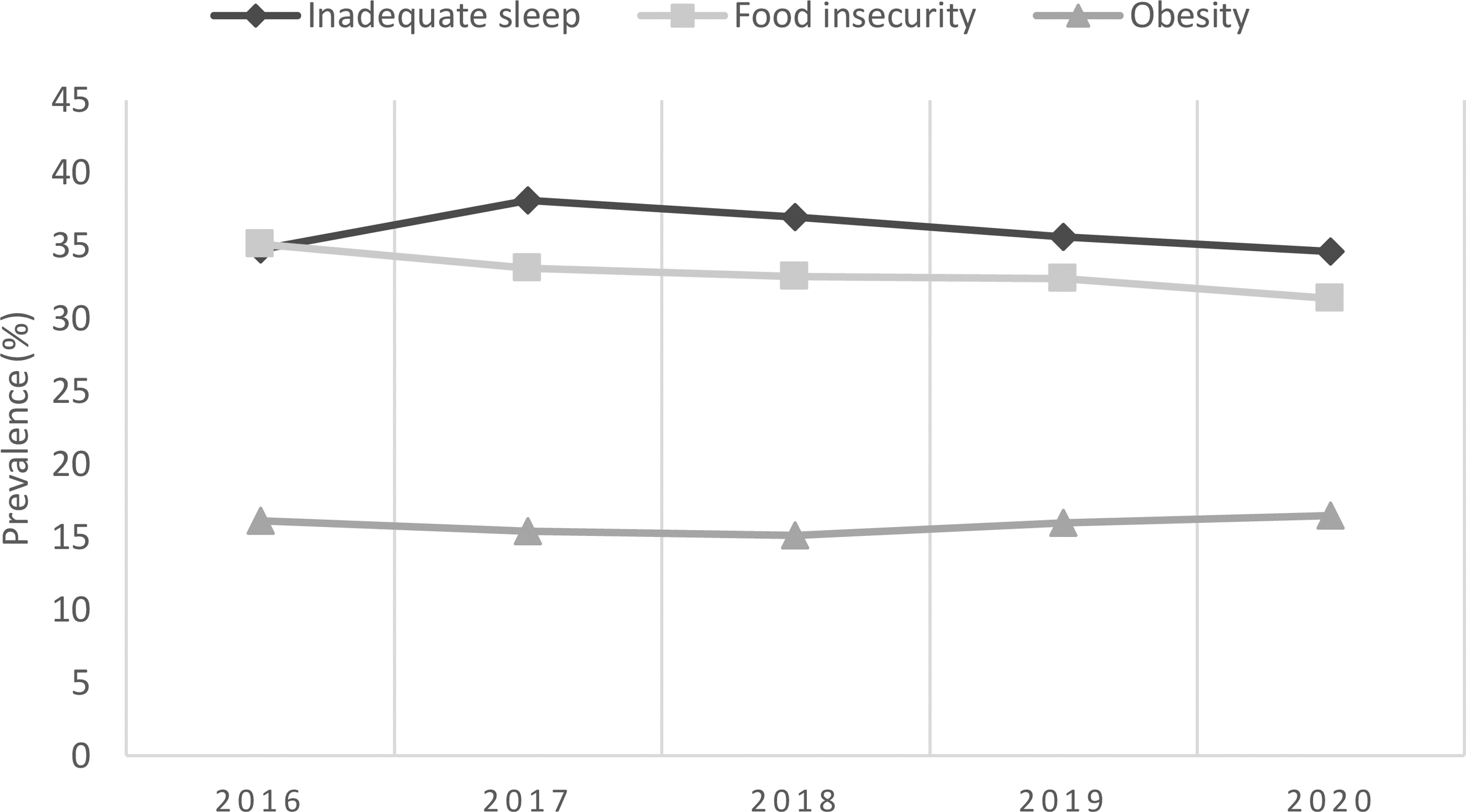
Trends in inadequate sleep duration, food insecurity, and obesity from 2016 to 2020 in US children 10–17 years of age.
Obesity Prevalence by Child Characteristics (n = 85,003)
Unweighted frequency.
p-Value for the X2 tests, used for each variable to examine differences across categories.
Other included American Indian or Alaska Native, Native Hawaiian, and other Pacific Islander, some other race, two or more races.
Highest level of education among reported adult.
Number missing = 199.
Inadequate sleep duration was defined as sleep duration <9 hours per day in children 10–12 years of age, and <8 hours per day in children 13–17 years of age.
FPL, federal poverty level; GED, general education development; NH, non-Hispanic.
Table 2 displays the direct and indirect effect (through sleep duration) of food insecurity on the prevalence of childhood obesity. Food insecurity was significantly associated with obesity after adjusting for age, sex, race/ethnicity, education, and poverty level [odds ratio (OR) = 1.78, 95% CI: 1.70–1.86]. The association was stronger among females (OR = 1.96, 95% CI: 1.84–2.10) and NH-Other race/ethnicity children (OR = 2.08, 95% CI: 1.79–2.46). The proportion mediated by sleep duration was 6.13%. In a stratified analysis, the proportion mediated by sleep duration was larger in males (7.13%) than females (5.22%). Similarly, children in the age group of 10–11 years and non-Hispanic Asian children had the highest proportion mediated by sleep duration (14.85% and 11.21%, respectively). Furthermore, the proportion mediated by sleep duration decreased with increasing age.
Direct and Indirect Effect (through Sleep Duration) of Food Insecurity on Childhood Obesity (n = 85,003)
The percent mediated was calculated as the natural indirect effect divided by the total effect and therefore depended on both the total effect and the indirect effect.
Other included American Indian or Alaska Native, Native Hawaiian, and other Pacific Islander, some other race, two or more races.
CI, confidence interval; OR, odds ratio.
In the sensitivity analysis, when we restricted the analysis to respondents on the extremes of the food security variable, the proportion mediated by sleep duration increased (11.06%, Supplementary Table S1). The analysis further adjusted for physical activity (Supplementary Table S2), and with a dichotomized mediator (Supplementary Table S3) were both consistent with the main analysis.
Discussion
In this study, we sought to determine whether food insecurity was associated with obesity in US children. We also wanted to determine if this relationship was mediated by sleep duration, and if so, to what extent. We found that children experiencing food insecurity had higher odds of having obesity. Furthermore, our results indicate that sleep duration acts as a mediator in the link between food insecurity and childhood obesity. The mediation was statistically significant but weak and more pronounced in the age group of 10–11 years, males, and non-Hispanic Asian children.
The relationship between food insecurity and obesity is complex. In addition to obesity, food insecurity, especially hunger, could also lead to weight loss. 32 Our study revealed a positive link between food insecurity and childhood obesity across age, sex, and race/ethnicity groups. A review of the literature noted that the food insecurity–obesity link among children is mixed but remained consistent among women, with sparse evidence among men and growing evidence among adolescents. 33 Similar to our findings, greater effects of food insecurity on obesity among girls has been reported in the US, Canada, and Korea.34–36 Food insecurity often occurred in low-income communities, more likely to experience restrictions such as inadequate transportation and reduced access to fresh food and vegetables. 37 Individuals who are food insecure tend to consume food high in calories and fat, thus increasing the risk of obesity. 9 Additionally, food insecurity contributes to irregular eating patterns characterized by periods of underconsumption and food deprivation when resources are limited, and compensatory overconsumption when resources are adequate, contributing to adiposity. 6
Lastly, girls exhibit more stress and anxiety in response to food insecurity, which could be the main driver of these apparent sex differences. 38 The stratified analysis by age group indicates that the mediation by sleep duration was higher in the younger age group (10–11 years) and decreased with increasing age. This could partially explain the null finding from the Do et al. study, which included a smaller sample of 12–17-year-old children compared with our study. 20 Sleep appears to have more impact on children's weight status at younger ages, reflecting difficulties coping with changes that affect sleep at the early phase of adolescence (e.g., puberty, increased social demand, school workload).
To our knowledge, this study is the first to explore whether sleep duration mediates the effect of household food insecurity on childhood obesity utilizing the counterfactual framework. Unlike the traditional mediation approach, the counterfactual framework allows for exposure-mediator interactions. 39 To date, most published mediation analyses have been conducted in the adult population. Our findings are consistent with findings in the adult population. The highest proportion mediated reported by Narcisse et al. was 7.82% among non-Hispanic Native Hawaiian and other Pacific Islanders. 18 Another study found that insomnia (including difficulty falling asleep, difficulty staying asleep, and waking up too early) mediated 16% of the food insecurity–obesity link. 17 Our study focuses only on sleep duration, which might explain the low proportion mediated. Different aspects of sleep health (e.g., sleep quality, sleep disturbances, sleep efficiency) might be involved in the causal pathway. 40
Overall, food insecurity may disrupt sleep and through inadequate sleep duration, food insecurity may increase the risk of obesity. The reason for the differences by age, sex, and race/ethnicity is not fully understood and should be explored in future investigations. In this study, the association between food insecurity and sleep duration and the association between sleep duration and obesity, were both stronger among males and non-Hispanic Asian children, which resulted in a stronger proportion mediated.
Mediation analyses imply causation that cannot be inferred from a cross-sectional design. Interpretation of this study's results relies on the validity of the assumption that food insecurity temporally precedes sleep duration, which itself occurs before obesity. This assumption has not been tested in this study; however, food insecurity was assessed during the past year, sleep duration during the past week, and BMI at the time of the survey. This study expands the literature on the relationships among food insecurity, sleep duration, and obesity and should be confirmed in longitudinal research. In addition, unmeasured/residual confounding cannot be completely ruled out in this secondary data analysis. Additional limitations of this study include the self-reported nature of the data and that food security was solely based on one question.
Future studies should consider including objective measures, especially for sleep duration (e.g., actigraphy, polysomnography) and a more comprehensive household food security question (e.g., 18-item household food security survey). Nevertheless, evidence supports the validity of parent or self-reported sleep duration.41,42 Finally, the food insecurity–sleep–obesity link may differ by country or region, therefore the findings from this study might not be generalizable to children outside of the United States. 43
Despite these limitations, this study relies on a large sample from a survey that utilized complex survey sampling to make inferences about U.S. children. This study adds to a small but growing body of literature that investigates the relationships among food insecurity, sleep, and obesity. Numerous food assistance programs have contributed to improved food security in the United States. Subsequent efforts should be implemented to expand and improve these programs. Public health interventions that address food insecurity will likely reduce obesity and improve sleep outcomes.
Footnotes
Impact Statement
This study contributes to the understanding of the mechanism by which food insecurity increases obesity in children through our finding of partial mediation by sleep duration. Additionally, subgroup differences were identified which indicate that the relationships among food insecurity, sleep, and obesity may interact with age, sex, and race/ethnicity.
Authors' Contributions
W.S. and D.A.C. conceived the study. W.S. conducted the literature search, performed the analysis, and drafted the initial report. W.S., D.A.C., D.D.H.T., and T.A. contributed to the data interpretation and critically revised the successive drafts of the article. All authors approved the final version of the report.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.