
Abstract
Background:
Societal changes during the COVID-19 pandemic may affect children's health behaviors and exacerbate disparities. This study aimed to describe children's health behaviors during the COVID-19 pandemic, how they vary by sociodemographic characteristics, and the extent to which parent coping strategies mitigate the impact of pandemic-related financial strain on these behaviors.
Methods:
This study used pooled data from 50 cohorts in the Environmental influences on Child Health Outcomes Program. Children or parent proxies reported sociodemographic characteristics, health behaviors, and parent coping strategies.
Results:
Of 3315 children aged 3–17 years, 49% were female and 57% were non-Hispanic white. Children of parents who reported food access as a source of stress were 35% less likely to engage in a higher level of physical activity. Children of parents who changed their work schedule to care for their children had 82 fewer min/day of screen time and 13 more min/day of sleep compared with children of parents who maintained their schedule. Parents changing their work schedule were also associated with a 31% lower odds of the child consuming sugar-sweetened beverages.
Conclusions:
Parents experiencing pandemic-related financial strain may need additional support to promote healthy behaviors. Understanding how changes in parent work schedules support shorter screen time and longer sleep duration can inform future interventions.
Introduction
During the COVID-19 pandemic, unprecedented societal changes, such as prolonged home stays and remote schooling, may impact children's health behaviors,1–7 particularly their dietary intake, physical activity, screen use, and sleep.8–10 Health behaviors in childhood are linked to adiposity, cardiometabolic outcomes, neurocognitive development, mental health, quality of life, and academic achievement.11–15 Health behaviors during the pandemic may have implications for child health for years to come if new behavior patterns (e.g., new modes of exercise or mealtime routines) persist in the postpandemic era. Among US children, there is growing evidence that the social and economic disruption of the pandemic contributed to higher BMI.16,17
However, less is known about children's adiposity-related behaviors because opportunities to conduct pediatric research was constrained early in the pandemic due to necessary public health precautions. 18 The few studies that assessed children's health behaviors were primarily conducted outside the United States,7,19,20 or among small or homogenous samples of children.6,21
In the decade before the pandemic, children's health behaviors were known to vary by child sex, age, race/ethnicity, and level of formal maternal education.22–24 These prepandemic health disparities may have been exacerbated by the differential effects of the pandemic on households, although this needs to be investigated directly.22,25–29 In addition, the impact of novel exposures or protective factors, such as pandemic-related financial strain or parent coping strategies, on children's health behaviors, is not well understood. Identifying modifiable factors 30 that reduce disparities in child health behaviors has the potential to drive programs, policy, and practice to support improved behaviors during the pandemic period and beyond.
The objectives of this study among children aged 3–17 years during the first 7 months of the COVID-19 pandemic were to (1) characterize dietary intake, physical activity, screen time duration, and sleep duration; (2) describe variation in health behaviors by sociodemographic characteristics, and (3) explore the extent to which the association between pandemic-related financial strain and child health behaviors may be modified by parent coping strategies.
Methods
Study Population
The Environmental influences of Child Health Outcomes (ECHO) Program is a national consortium of 69 established pediatric cohort studies investigating the effects of early life environmental exposures on child health using a common protocol since 2019.31,32 Institutional review boards monitored human subject activities and the centralized Data Analysis Center. Participants provided informed consent. Fifty cohorts representing 77 recruitment sites (Fig. 1) assessed behaviors (diet, physical activity, screen time, or sleep) of children aged 3–17 years during the first 7 months of the pandemic (April 1 to October 31, 2020). While the World Health Organization declared COVID-19 a pandemic on March 11, 2020, April 1 was used as the start date because the assessments queried behaviors in the preceding week to month. Children were excluded if they were missing data regarding their sex. Assessments were completed in-person or remotely.

ECHO COVID-19 Questionnaire
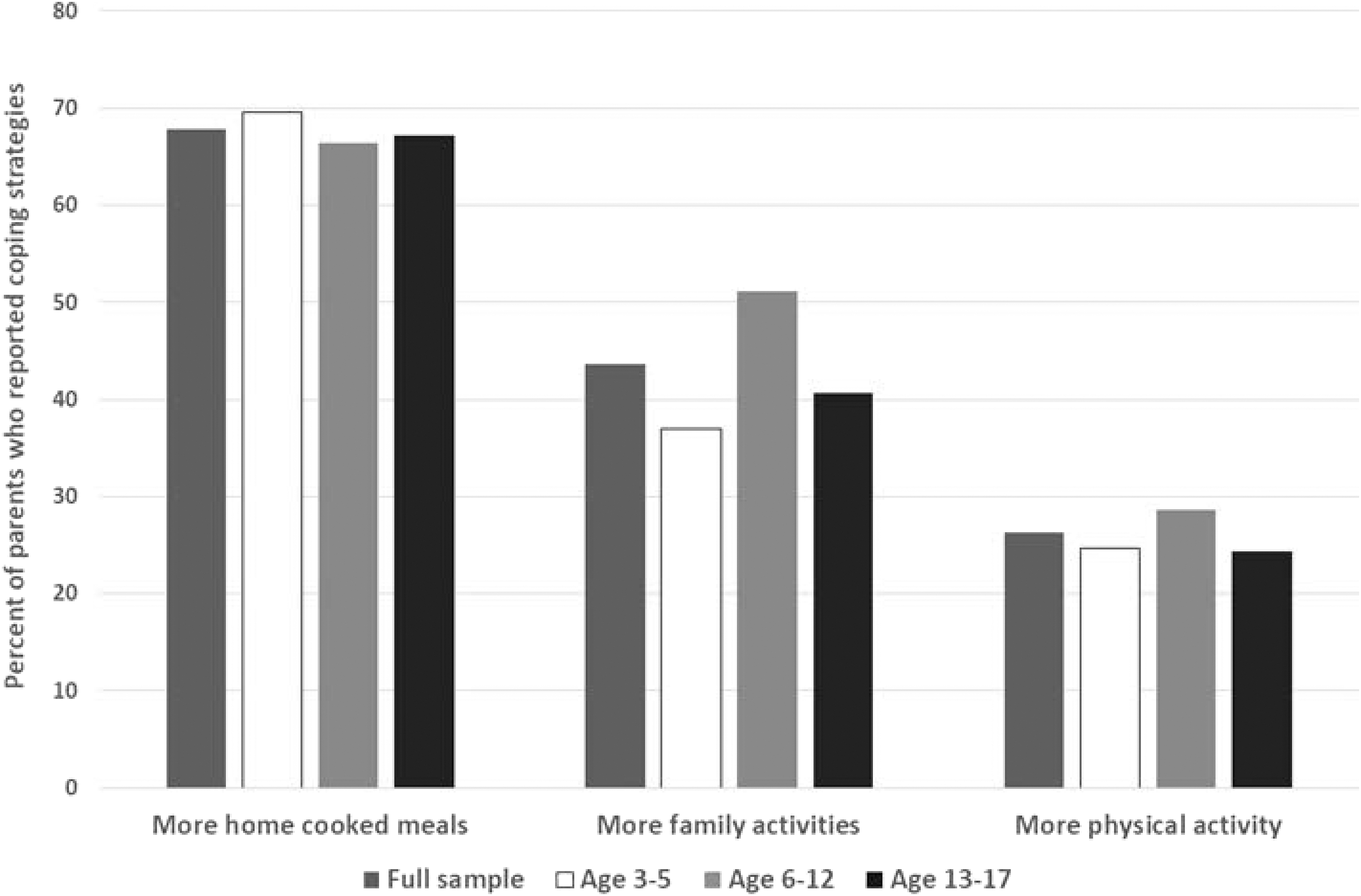
This parent self-report questionnaire was developed in April 2020. Pandemic-related financial strain was assessed with yes/no questions asking if financial concerns were a source of stress; food access was a source of stress; a parent or spouse/partner lost their job or experienced reduced work hours; a parent had to pay more for childcare; or a parent or spouse/partner had to change their work schedule to care for their children. Parent coping strategies were assessed by asking, “what have you done to cope with your stress related to the COVID-19 outbreak?” and “which behaviors have you changed because of the COVID-19 outbreak?” with a multiselect answer option. This analysis considered responses relevant to child behaviors: eating more home-cooked meals, parents getting more exercise, and engaging in more family activities and excluded other types of coping listed in the questionnaire (e.g., tobacco use, alcohol use, meditation).
Sociodemographic Characteristics
The categorical variables included child age group, sex at birth, race and ethnicity, and maternal education (Table 1). The sociodemographic variables were primarily collected via self-report. In some cases, child sex designated at birth and date of birth were extracted from medical records.
Characteristics of the Study Sample Among Children Aged 3–17 Years in the Environmental Influences on Child Health Outcomes Program
GED, General Educational Development; SD, standard deviation.
Health Behaviors
Dietary intake was assessed with the Block Kids Food Frequency Questionnaire (FFQ) 33 or the Dietary Screener Questionnaire (DSQ). 34 These semiquantitative questionnaires were validated for assessing food intake among children and adolescents (child self-report or parent-proxy report). The FFQ queried intake frequency and average portion size of 85 food and beverage items over the preceding week. The DSQ queried intake frequency of 25 food items/categories over the preceding month. Data were harmonized to produce two categorical variables reflecting intake frequency of sugar-sweetened beverages (SSBs) and fruits and vegetables (FV), each with six response categories ranging from “less than once/week” to “once/day or more.”
Physical activity was assessed with one item from the 8-item PROMIS Pediatric v1.0 Physical Activity Short Form 8a, a valid measure of children's lived experiences of physical activity assessed by child self-report or parent-proxy. 35 Respondents (the child when ≥8 years of age; otherwise, the parent) reported “In the past 7 days, how many days were you physically active for 10 minutes or more?” with 5 response options ranging from “no days” to “6–7 days.”
Screen time was assessed with the Child Media Use Questionnaire based on the surveys developed by Common Sense Media, a national leader in media use survey assessment. 36 Screen time included educational (e.g., homework) and recreational (e.g., video games) use. Respondents (the child when ≥12 years of age; otherwise, the parent) reported typical screen time duration separately for weekdays and weekends. Parents reported screen time in minutes, if screens were used for less than 1 hour and in hours and minutes if screens were used for 1 hour or more.
Average nightly sleep duration during the past week was assessed with the ECHO Program's Sleep Health of Children and Adolescents Questionnaire by the child when ≥12 years of age; otherwise, by the parent. This questionnaire is a valid and reliable measure of sleep health for child self-report and parent-proxy report. 37 A reported sleep duration of less than 5 hours was set to missing. Any responses more than 18 hours were capped at 18 hours.
Statistical Analysis
Participant characteristics were tabulated in the full sample and by age group. To examine the association between sociodemographic characteristics and behaviors, we used a generalized estimating equations (GEE) approach to account for correlation between children within cohorts (the independence correlation structure was specified for GEE models). Logistic regression was used for binary outcomes (SSB and FV intake). Intake was dichotomized at ≥3 times/week for SSBs and ≥once/day for FV due to small sample sizes in some categories and to approximate dietary guidelines. 38 For the ordinal physical activity outcome, a cumulative link regression model was used to estimate the odds of reporting one higher category or above of weekly physical activity (response options: no days, 1, 2–3, 4–5, and 6–7 days).
Linear regression was used for continuous outcomes (screen time and sleep). All models adjusted for child age, sex, race, and ethnicity; maternal education; pandemic-related financial strain; and the time between the start of the pandemic (April 1, 2020) and the date the COVID-19 questionnaire was administered.
The eight financial strain and coping variables were included as independent, binary variables in the models. To evaluate whether the association between pandemic-related financial strain and health behaviors was modified by parent coping strategies, interaction terms were added to the models with corresponding outcomes: financial strain × “eat more home-cooked meals” was included in the dietary models; financial strain × “get more physical activity” was included in the activity models; and financial strain × “engage in more family activities” was included in the screen time model. No model included an interaction term for sleep because none of the coping strategies was hypothesized to affect sleep.
Results
The analytic sample included 3315 children (Fig. 1). Data were not available for all 3315 children for all 4 behaviors because some cohorts (1) only administered some of the questionnaires as part of their protocol or (2) administered questionnaires to some participants outside the 7-month period. Child sociodemographic characteristics are shown in Table 1. Over 90% of parents reported at least one type of pandemic-related financial strain: financial concerns were stressful (35.3%); parent lost job/reduced hours (24.7%); parent changed work schedule to care for children (23.1%); spouse/partner lost job/reduced hours (20.6%); access to food was a source of stress (13.5%); and family paid more for child care (5.4%). Descriptive data on health behaviors are presented in Table 2. Median times between the assessment dates for financial strain with the COVID-19 questionnaire and health behaviors were 0 days.
Health Behaviors (Dietary Intake, Physical Activity Frequency, Screen Time Duration, and Sleep Duration) Reported During the First 7 Months of the COVID-19 Pandemic Among Children Aged 3–17 Years in the Environmental influences on Child Health Outcomes Program
In accordance with ECHO's publication and data use policy, cell sizes smaller than five are suppressed for privacy. The sample size in an additional column is also suppressed to prevent calculation of the exact sample size in cell with less than five participants.
We computed a weighted average hours of screen time for each child across weekday and weekend screen time.
Overnight sleep duration only; excludes napping during the day.
Children of parents who changed their work schedule to care for their children had 82 fewer min/day of screen time (−1.37 hours, 95% confidence interval [CI] −2.28 to −0.45) and 13 more min/day of sleep (0.21 hours, 95% CI 0.09–0.33) compared with children of parents who did not change their work schedule (Table 3). Children of parents who changed their work schedule were 31% less likely to consume SSBs 3–4 times/week (compared to 2 times/week or less) (odds ratio [OR] 0.69, 95% CI 0.49–0.98). Children of parents who reported financial concerns as a source of stress had 10 fewer min/day of sleep (−0.16 hours, 95% CI −0.30 to −0.02) compared with children of parents who did not report this type of stress (Table 3). Children of parents who reported access to food as a source of stress were 35% less likely to engage in a higher level of physical activity (OR 0.65, 95% CI 0.44–0.94).
Association of Sociodemographic Characteristics With Dietary Intake, Physical Activity Frequency, Screen Time Duration, and Sleep Duration During the First 7 Months of the COVID-19 Pandemic Among Children Aged 3–17 Years in the Environmental influences on Child Health Outcomes Program
ORs and 95% CIs from GEE logistic regression models (using the “geeglm” function from the R package “geepack”) clustered on cohorts, estimating odds of consuming sugar-sweetened beverages three to four times per week or more compared with two servings per week or less, and odds of consuming one or more servings of FV per day compared with consuming less than one serving of FV per day.
Data are ORs (95% CIs) from GEE cumulative link regression models (using the “ordLORgee” function from the R package “multgee”), reflecting odds of moving up one or more category in the ordinal categories of days of being physically active ≥10 minutes: 0, 1, 2–3, 4–5, and 6–7 days/week.
Data are beta coefficients from GEE linear regression models (using the “geeglm” function from the R package “geepack”), reflecting change in hours of screen time and sleep.
In addition to the sociodemographic factors shown, all models are adjusted for time between the start of the COVID-19 pandemic (April 1, 2020) and the assessment of COVID-19 financial strains.
p < 0.05; **p < 0.01; −p-values were given from the GEE Wald test.
CI, confidence interval; FV, fruits and vegetables; GED, General Educational Development; GEE, Generalized estimating equations; OR, odds ratio.
As shown in Table 3, older children had a higher level of SSB intake and more screen time, and a lower level of physical activity and less sleep compared with younger children. Compared with females, males were 35% less likely to consume FV daily (OR 0.65, 95% CI 0.53–0.79) and 64% more likely to be more physically active (OR 1.64, 95% CI 1.23–2.13). Having a mother with at least some college education was associated with lower SSB intake (OR 0.46, 95% CI 0.24–0.87), higher levels of physical activity (OR 1.47, 95% CI 1.05, 2.04), and longer sleep (0.34 hours, 95% CI 0.08–0.60).
Compared with children who were non-Hispanic white, children who were Hispanic were 64% less likely to consume FV daily (OR 0.36, 95% CI 0.15–0.87), were 30% less likely to engage in a higher level of physical activity (OR 0.70, 95% CI 0.51–0.95), and had 25 fewer minutes of sleep (−0.42 hours, 95% CI −0.67 to −0.17) (Table 3). Compared with children who were non-Hispanic white, children who were non-Hispanic black were 61% less likely to engage in a higher level of physical activity (OR 0.39, 95% CI 0.28–0.54) and had almost 2 more h/day of screen time (1.94 hours, 95% CI 0.66–3.23) and 41 fewer min/day of sleep (−0.69 hours, 95% CI −0.90 to −0.48).
The most commonly reported coping strategy was eating more home-cooked meals (Fig. 2). Among children in families reporting no financial strain, engaging in more family activities was associated with an hour less screen time/day (−1.08 hours, 95% CI −1.60 to −0.56; Table 4). Children in families with at least one parent who changed their work schedule and children engaged in more family activities had 2.6 hours less screen time than those who did neither (not shown in table: −2.58, 95% CI −3.62 to −1.55). Children in families with financial concerns were three times more likely to consume SSBs (OR 3.03, 95% CI 1.66–5.54), and this association was modestly attenuated in families that reported more home-cooked meals compared with those who did not (interaction OR 0.19, 95% CI 0.11–0.33). The association between access to food as a source of stress and SSB intake was amplified among those who reported more home-cooked meals (OR 4.46, 95% CI 1.66–12.01).
Association Between Parent Coping Behaviors and Dietary Intake, Physical Activity, and Screen Time During the First 7 Months of the COVID-19 Pandemic Among Children Aged 3–17 Years in the Environmental influences on Child Health Outcomes Program
ORs and 95% CIs from GEE logistic regression models (“geeglm” function from the R package “geepack”) clustered on cohorts, estimating odds of consuming sugar-sweetened beverages three to four times per week or more compared with two servings per week or less, and odds of consuming one or more servings of FV per day compared with consuming less than one serving of FV per day.
Data are ORs (95% CIs) from GEE cumulative link regression models (“ordLORgee” function from the R package “multgee”), reflecting odds of moving up one or more category in the ordinal categories of days of being physically active ≥10 minutes: 0, 1, 2–3, 4–5, and 6–7 days/week.
Data are beta coefficients from GEE linear regression models (“geeglm” function from the R package “geepack”), reflecting change in hours of screen time and sleep.
All models are additionally adjusted for child age and sex, maternal education, and time between the start of the COVID-19 pandemic (April 1, 2020) and the assessment of COVID-19 financial strains. Interaction terms with the coping strategy “eat more home-cooked meals” were included in the models with diet as the outcome. Interaction terms with “get more physical activity” were included in the models with physical activity as the outcome. Interaction terms with “engage in more family activities” were included in the model with screen time as an outcome.
There was no model for sleep duration because none of the coping strategies was hypothesized to effect sleep.
p < 0.05; **p < 0.01; p values were given from the GEE Wald test.
Discussion
Among a geographically diverse sample of children and adolescents during the first 7 months of the COVID-19 pandemic, financial concerns and access to food as a source of stress were associated with less frequent physical activity and shorter sleep duration. Changes in parent work schedules were associated with a shorter screen time duration, less frequent SSB intake, and a longer sleep duration, suggesting that changes in parent work schedules generally had a protective effect on child health behaviors. In general, these findings did not differ among families who reported using pandemic-specific coping strategies compared with families who did not. Consistent with prepandemic disparities, healthier behaviors were reported among younger children, children who were non-Hispanic white and children of mothers with more formal education.
The 2020–2025 Dietary Guidelines for Americans recommends multiple servings of FV/day, 38 yet, 32% of children in the ECHO sample did not consume FV daily during the study period. Older children consumed FV less frequently and SSBs more frequently, consistent with prepandemic patterns. 22 The less frequent FV intake among Hispanic children during the pandemic contrasts with the absence of this association prepandemic.22,39,40 One unexpected finding was that access to food as a source of stress did not appear to be associated with dietary intake. This is inconsistent with the findings of Hu et al. who found that food insecurity was associated with a greater increase in SSB intake among children during the pandemic. 41 Prepandemic studies also report higher habitual SSB intake among food insecure families 42 and families participating in the Supplemental Nutrition Assistance Program. 43
We expected this association to be weaker among families who reported preparing more home-cooked meals during the pandemic given the positive association between the frequency of home-prepared meals and diet quality 44 but instead found the opposite. One possibility is that home-cooked breakfast and lunch meals during remote schooling may have replaced the intake of meals that were consumed as part of the School Breakfast Program or National School Lunch Program; participation in these programs has been linked to higher milk intake and lower SSB intake. 45 However, this needs to be investigated directly.
The 2018 Physical Activity Guidelines for Americans recommends being active throughout the day for preschoolers and at least 60 minutes of moderate-to-vigorous activity daily for children and adolescents, 46 yet, only 34% of children in the ECHO sample reported at least 10 minutes of activity daily. Lower activity levels among older children, children with mothers who had a lower level of formal education, and Hispanic or non-Hispanic black children in the present analysis are consistent with prepandemic disparities.47–49 Access to food as a source of stress was associated with less frequent physical activity. Additional research is needed to determine if ensuring that families' basic physiological needs are met in one health domain (e.g., food security) can promote positive behaviors in another (e.g., active lifestyle).
Surprisingly, job loss and financial concerns were not associated with physical activity. One possible explanation is that barriers to physical activity related to public health precautions (e.g., shuttered recreational facilities) 21 could not be surmounted, even among families with adequate financial resources. Another possibility is that lower income families may have already been accustomed to utilizing opportunities in their immediate environment for active play because their access to resources (e.g., organized sports) may have similarly been limited prepandemic. 50
For children aged 3–5 years, the American Academy of Pediatrics (AAP) recommends up to 1 h/day of high-quality programming. 51 Median screen duration among ECHO children in this age group during the pandemic was 4 h/day. For children ≥6 years of age, the AAP recommends consistent limits on media use and preventing media use from replacing healthy behaviors. 51 The median educational and recreational screen time duration was 6 h/day among children aged 6–12, and up to 12 h/day among adolescents. Longer screen time duration among older versus younger children was also documented prepandemic. 52
The finding that changes in parent work schedules were associated with a large decrease in daily media use and a small increase in sleep duration is important because changes in parent work schedules may persist into the postpandemic period 53 and continue to shape behaviors. Our finding that engaging in more family activities was associated with an hour and a half less of daily media use mirrors prepandemic findings 54 and suggests that engaging in family activities may be a potential intervention target to reduce screen time.
In our sample, the median nightly sleep duration was within the ranges recommended by the American Academy of Sleep Medicine for all age groups, although at the lower end of the ranges. 55 Similar to the prepandemic period, sleep duration during the pandemic was longer among children who were non-Hispanic white and children whose mothers had a higher level of formal education.29,56,57 Children of parents who reported financial concerns had a slightly shorter sleep duration, as would be expected, based on the link between parental perceived economic well-being and sleep duration. 57 Future studies can elucidate potential mechanisms, which may include sleep timing, quality, and disturbance58,59 and whether a longer nap duration, which was not reported here, may have offset shorter nighttime sleep.
This study has several strengths. The ECHO Program is well positioned to measure pandemic behaviors due to its member cohorts following a common protocol that includes validated instruments. The roll-out of the ECHO protocol in 2019 before the emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) provided existing infrastructure for standardized and remote data collection and data sharing early in the pandemic. The rapid development of an COVID-19 questionnaire allowed for the assessment of novel variables: pandemic-related financial strain and pandemic-specific coping.
This study also has limitations. First, the cross-sectional design prohibits causal inferences about the association between sociodemographic characteristics, coping, and health behaviors. Ongoing data collection, in which a subsample of ECHO participants provided repeated measures of health behaviors prepandemic and at two time points during the pandemic, can address this limitation in future analyses. Second, this is not a population-based study because the ECHO Program was not designed this way. Nevertheless, the present analysis combined data from ethnically and socioeconomically diverse children in all U.S. Census regions, improving the generalizability of findings. Third, the pandemic was a dynamic period but is defined here as a single time-period. To minimize this limitation, the study period was constricted to the first 7 months of the pandemic when a COVID-19 vaccine was not yet available; and the time between April 1, 2020 and data collection was included in all models.
The study did not consider neighborhood-level features (e.g., safety, population density) that are likely to associate with individual-level characteristics. While this is unlikely to affect the relationship between individual-level characteristics and health behaviors, neighborhood-level features may help explain the relationships observed in the present analysis and/or give additional insights into interventions. For example, given the known relationships among race/ethnicity, individual-level socioeconomic status and place in the United States, 60 observed relationships between child race/ethnicity and the health behaviors under study may be related to underlying differences in the neighborhood characteristics of non-Hispanic white children and minority children (Hispanic, non-Hispanic black).
Finally, it is likely that pandemic-related contextual factors (e.g., local public health ordinances) may have influenced health behaviors, and information about these statistics were not systematically collected across the ECHO cohorts and, thus, were not included in the analyses; however, given the broad representation of U.S. geography across the participating cohorts, we do not believe that this omission would systematically affect the findings.
In summary, along with the continued effort to reduce disparities in health behaviors by sociodemographic characteristics observed prepandemic, pandemic-related opportunities for intervention are greatest among families who report financial concerns and access to food as sources of stress. Identifying the mechanisms by which changes in parent work schedules support a shorter screen time duration and a longer sleep duration may help direct future intervention efforts, particularly for families experiencing financial strain. Commonly used coping strategies did not mitigate the effect of financial strain on health behaviors, suggesting that parents may need additional support to overcome pandemic-related challenges.
Footnotes
Authors' Contributions
Dr. Bekelman conceptualized the article, provided input on the analysis plan, drafted the initial article, and reviewed and revised the article. Dr. Sauder conceptualized the article, provided input on the analysis plan, reviewed and revised the article, and served as senior author. Dr. Knapp and Ms. Dong harmonized the data, applied the study design, analyzed the data, drafted the initial article, created the tables, and reviewed and revised the article. Drs. Karagas, Dabelea, Dunlop, O'Shea, Wright, Huddleston, Carroll, Ganiban, Breton, Mihalopoulos, Bastain, Ferrara, Hedderson, Melough, Fry, Gilliland, Hockett, Elliott, Stanford, Lester, Zhao, and Hipwell designed and supervised data collection for their respective cohort studies, and critically reviewed the manuscript for important intellectual content. Drs. Lai, Lucchini, Davis, and Gilbert-Diamond critically reviewed the article for important intellectual content. All authors approved the final article as submitted and agreed to be accountable for all aspects of the work.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funder/sponsor had no role in the study design; the collection, analysis, and interpretation of data; the writing of the report; and the decision to submit the article for publication.
Data Availability Statement
The datasets for this article are not publicly available because, per the NIH-approved ECHO Data Sharing Policy, ECHO-wide data have not yet been made available to the public for review/analysis. Requests to access the datasets should be directed to the ECHO Data Analysis Center (ECHO-DAC@rti.org).
Acknowledgments
The authors wish to thank our ECHO colleagues, the medical, nursing and program staff, as well as the children and families participating in the ECHO cohorts. We also acknowledge the contribution of the following ECHO program collaborators: ECHO Components—Coordinating Center: Duke Clinical Research Institute, Durham, North Carolina: Smith PB, Newby KL, Benjamin DK; Data Analysis Center: Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD: Jacobson LP; Research Triangle Institute, Durham, NC: Parker CB; Person-Reported Outcomes Core: Northwestern University, Chicago, IL: Gershon R, Cella D. ECHO Awardees and Cohorts—Albert Einstein College of Medicine, Bronx, New York: Aschner JL, New York University, New York, New York: Blair CB, Memorial Hospital of Rhode Island, Pawtucket: Deoni S, D'Sa VA, New York State Psychiatric Institute at Columbia University, New York: Duarte CS, Canino GJ, Monk CE, Posner JE, Kaiser Permanente, Oakland, California: Ferrara A, Croen LA, University of Wisconsin-Madison: Gern J, Bacharier, L, Rivera-Spoljaric, K, Henry Ford Health System, Detroit, Michigan: Johnson C; Ownby D.; Zoratti E., Vanderbilt University Medical Center, Nashville, Tennessee: Hartert T, University of California, Davis: Hertz-Picciotto I, Bennett DH, Schweitzer JB, Brigham & Women's Hospital, Boston, Massachusetts: Litonjua AA, Weiss ST, Oregon Health & Science University, Portland, Oregon: McEvoy CT, Spindel ER, Drexel University, Philadelphia, Pennsylvania: Newschaffer CJ, University of Washington, Seattle, Washington: Dager, S, Children's Hospital of Philadelphia, Philadelphia, Pennsylvania: Schultz, R, University of North Carolina, Chapel Hill, North Carolina: Piven, J, Johns Hopkins University, Baltimore, Maryland: Volk, H, University of California MIND Institute, Davis, California: Schmidt, R, Kaiser Permanente, Oakland, California: Croen, L, University of Rochester, New York: O'Connor TG, Buss C, Miller RK, Wadhwa PD o University of Pittsburgh. Magee-Women's Hospital, Pennsylvania: Simhan HN, University of California, Davis: Schmidt RJ, Ozonoff S, Michigan State University, East Lansing, Michigan: Paneth N, Kerver JM, Ruden DM, Columbia University, New York, New York: Perera FP, Herbstman JB, University of Illinois, Urbana: Schantz SL, University of California, San Francisco: Woodruff T, New York University School of Medicine, New York, New York: Trasande L. In addition, we thank Mingyi Li for her assistance with data analysis.
Funding Information
Research reported in this publication was supported by the Environmental influences on Child Health Outcomes (ECHO) program, Office of The Director, National Institutes of Health, under Award Numbers U2COD023375 (Coordinating Center), U24OD023382 (Data Analysis Center), U24OD023319 (PRO Core), and UG3/UH3 OD-023253 (Dr. Camargo), UH3OD023248 (Dr. Dabelea), UG3/UH3 OD023318 (Dr. Dunlop), UG3/UH3 OD023279 (Dr. Elliott), UG3/UH3 OD023289 (Dr. Ferrara), UG3/UH3 OD023244 (Dr. Hipwell), UG3/UH3OD023337 (Dr. Huddleston), UG3/UH3 OD023275 (Dr. Karagas), UG3/UH3 OD023389 (Dr. Leve and Dr. Neiderhiser), UH3OD023290 (Dr. Rundle), UH3OD023347 (Lester) UH3OD023337 (Drs. Wright, Carroll, and Huddleston), UG3/UH3OD023348 (Drs. O'Shea and Fry), UH3OD023328 (Dr. Duarte), T32MH016434-41 (Dr. VanBronkhorst), UG1OD024943 (Drs. Pahud and Davis), UH3OD023287 (Breton/Bastain/Gilliland), UG3/UH3 OD023249 (Drs. Stanford and Mihalopoulos), UG3 OD023271 (Multi-PI: Drs. Karr, Bush, LeWinn, Sathyanarayana, and Tylavsky).
Author Disclosure Statement
Drs. Breton, Camargo, Carroll, Dunlop, Elliott, Ganiban, Gilliland, Knapp, O'Shea, Sauder, Stanford, and Wright report funding from the National Institutes of Health. The other authors have no conflicts of interest to disclose.