
Abstract
Background:
Multicomponent interventions are the first line of treatment for pediatric obesity, but are challenging to access. Mobile health (mHealth) interventions hold promise as they address commonly cited barriers for attending in person programs and have potential for wide scale dissemination.
Methods:
This retrospective cohort study examined data from youth who enrolled in the Kurbo program, which includes personal health coaching and a mobile app. Hierarchical linear regression was used to examine the impact of baseline percentage of the 95th% percentile for body mass index (%BMIp95), number of coaching sessions, and length of time enrolled in the program on change in %BMIp95, controlling for baseline age and sex.
Results:
A total of 3500 youth (mean age of 12.79 years, 71.3% female) were included. Youth experienced a 0.70 U decrease in BMI [standard deviation (SD) = 2.19] and a 4.45% decrease (SD = 8.5) in %BMIp95 over a mean of 31.5 weeks. The overall regression model was significant, R2 = 0.066, F(3,3494) = 77.18, and p < 0.001. Predictors of decrease in weight status included being female (b = −1.11, p < 0.001), higher baseline %BMIp95, (b = −0.58, p < 0.001), and greater number of coaching sessions (b = −0.12, p < 0.001), while greater time enrolled in the program (b = 0.02, p < 0.001) was associated with less change.
Conclusion:
Findings suggest a scalable coaching program with integrated digital tools for monitoring diet and activity can lead to significant reductions in weight status. Findings need to be replicated with more rigorous study designs, including a comparison condition and verified assessment of height and weight.
Introduction
Overweight and obesity in youth is a public health crisis in the United States.1,2 Obesity during childhood and adolescence confers risk for a number of negative health and psychosocial outcomes,3–6 and tracks strongly to adulthood, 7 which in turn is related to increased rates of morbidity, including multiple types of cancer, and all-cause mortality.8,9
In 2017, the U.S. Preventive Services Task Force (USPSTF) reissued a Grade B recommendation, 10 initially made in 2010, 11 for clinicians to screen children aged 6–18 years for obesity and refer identified youth to comprehensive, multicomponent programs with >26 contact hours targeting changes in diet and physical activity, supported by behavioral strategies.10,11 However, the majority of youth in the United States do not receive evidence-based treatment for obesity. 12 There are a number of barriers impacting access to such programs, including their limited number (only 52% of 118 children's hospitals surveyed reported multidisciplinary programs), high cost, geographic location, lack of transportation or time required for travel to in-person programs, and program flexibility.12–16 In addition, some families may be reluctant to participate in programs offered in more clinical settings due to pervasive experiences of weight stigma in health care settings.17,18
Mobile health (mHealth) interventions offer one avenue for addressing such barriers. mHealth is the “use of mobile and wireless technologies to support the achievement of health objectives.” 19 Such interventions are accessed remotely, offering flexibility with regard to family participation and engagement and precluding time and costs associated with travel. A review of mHealth interventions indicates their effectiveness in promoting changes in eating and activity behaviors and reducing weight status in adults with overweight and obesity. 20
While there is a robust literature examining the effectiveness of mHealth interventions targeting adult weight loss, fewer studies have been conducted with pediatric populations.21–23 A scoping review of mHealth interventions targeting pediatric weight control sought to characterize common elements of published studies, and highlighted that the most common elements were use of text messaging and mobile applications. 23 Findings indicate the majority of studies focused on assessing intervention feasibility, acceptability, or usability, with less than half of the studies reporting on treatment effect. A recent narrative review of telehealth interventions, defined as those that involved use of phone or videoconference to deliver pediatric weight control interventions, identified high attendance and retention rates associated with interventions that incorporated telehealth, and statistically significant, although small reductions in standardized BMI score (zBMI). 22
These recent reviews highlight the potential of mHealth interventions to address pediatric weight control as an emerging area and further studies documenting the effectiveness of such programs are warranted. One potentially limiting factor in research evaluating the effectiveness of mHealth interventions is the speed with which updates in technology occur, often outpacing the research timeline, and resulting in evaluation of outdated technology. 24 Commercially available weight control interventions comprise a specific segment of the mHealth intervention sector and may offer an advantage with regard to flexibility and speed with which technological innovations may be incorporated.
There is evidence supporting the effectiveness of commercial programs in promoting weight loss in adults, 25 including showing superior results to a self-help program 26 and comparing favorably to a state-of-the art behavioral weight control program offered in an academic setting. 27 While findings from adult commercial programs cannot be compared directly to pediatric populations, they serve to illustrate the potential promise of such programs for the pediatric space. Research on commercially available pediatric programs is required to examine this question directly.
Kurbo is a commercially available coaching program that includes health coaching with an integrated mobile app for monitoring dietary intake and physical activity. Kurbo was developed as a guidelines-based pediatric program based on work conducted by investigators at Stanford University. A small study documents the utility of the program as a form of early intervention for adolescents waiting to enroll in a multidisciplinary weight control program. 28 In this study, access to the mobile app and individual health coaching was associated with significant improvements in quality of life and decreases in body fat, although not zBMI. 28
A larger retrospective cohort study examined the relationship between involvement with health coaching as part of the Kurbo program and change in weight status in youth (5–18 years) with overweight/obesity who participated in the program between March 2015 and March 2017. 29 This study showed meaningful decreases in weight status as measured by %BMIp95 (∼−5.0%) across the age continuum as well as a significant relationship between the number of coaching sessions completed and decrease in weight status.
The goal of the current study was to build upon this work by examining predictors of weight change outcomes in participants in the Kurbo program incorporating a more extensive and more recent time period, and a larger study sample. The study had two primary aims: (1) examine changes in weight status in youth enrolled in Kurbo over a 6-year period and (2) examine predictors of weight status change in these youth. The primary study hypothesis was that significant reductions would be observed over time and that greater reduction would be associated with more coaching sessions, length of time enrolled in the program, and higher baseline BMI.
Methods
Study Design
This study involved a retrospective cohort design. Data were extracted based on youth who participated in the commercial health coaching program between March 15, 2015 and June 24, 2021. The program was made available to families across the United States through a number of potential avenues, including provider referral, health insurance plans, parent employers, and internet search. Deidentified participant data were provided to the study authors from the Kurbo data registry. The research study was determined to be exempt by the Lifespan Institutional Review Board.
Study Participants
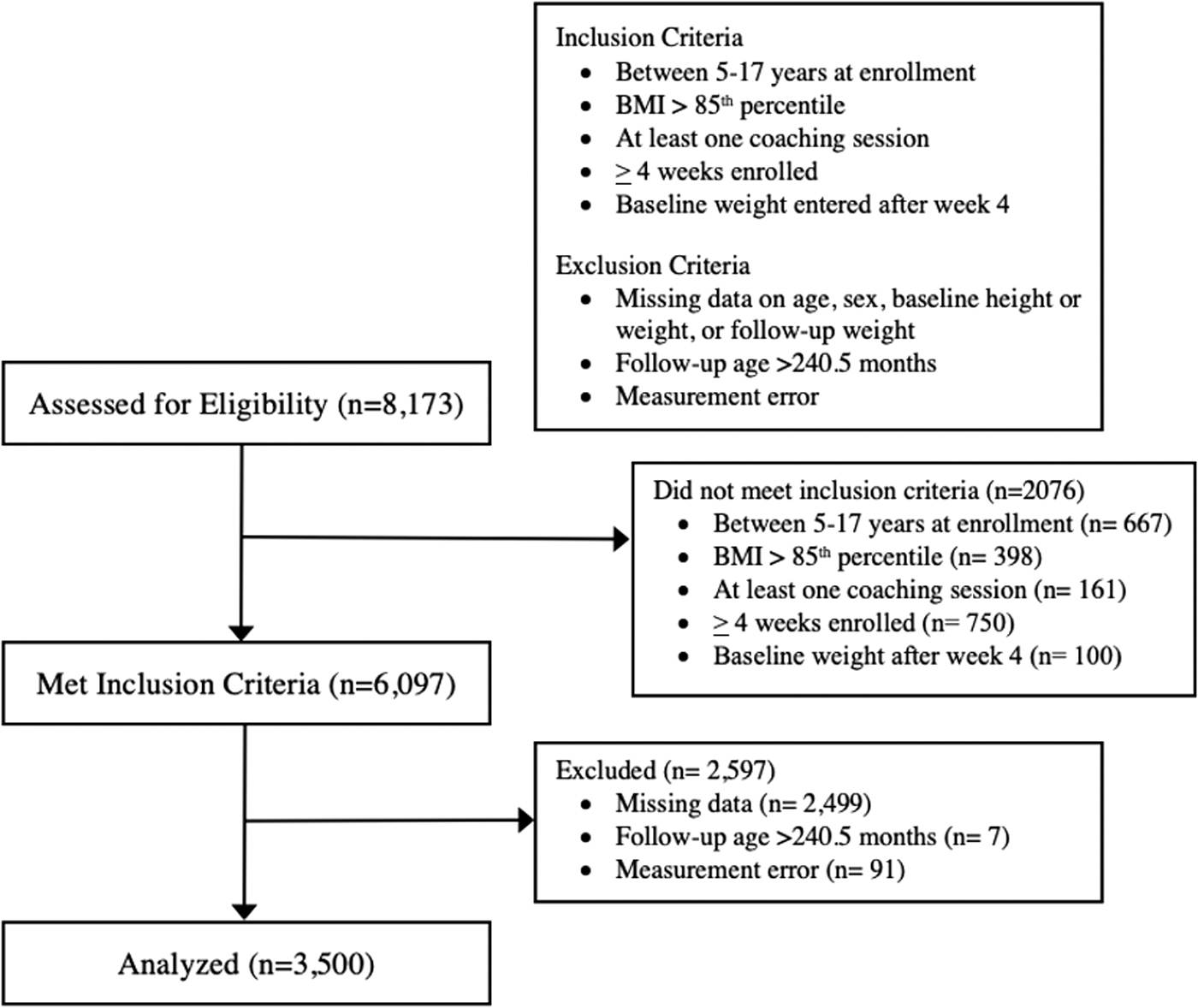
Participants were included in the study analyses if they (1) were 5–17 years at the time of program enrollment; (2) had a BMI >85th percentile; (3) participated in at least one coaching session; and (4) their most recently recorded weight was ≥4 weeks after program enrollment to allow for a minimal window for observing weight change. Youth were excluded from the analyses if information regarding age, sex, baseline height or weight, or follow-up weight was missing. Participants were also excluded if their age at the most recently recorded weight was older than 240.5 months, as CDC BMI percentile calculation ends at 240.5 months.
Kurbo Program
As previously described, the standard Kurbo program includes weekly sessions with a personal health coach via videoconference and use of an integrated mobile app. Participants can choose to subscribe to Kurbo for 1, 3, or 6 months and then are automatically converted to a monthly subscription until they decide to discontinue their involvement with the program. The cost of participation is $85 for 1 month, $210 for 3 months, and $300 for 6 months. Cost of program participation was paid for by families out of pocket, covered by employers, or through insurance. Program content is based on evidence-based pediatric, family-based behavioral weight control interventions with an emphasis on self-monitoring of eating and physical activity, reinforcement for working toward goals, and supportive accountability provided through coaching.30–32
Recommendations for eating and physical activity are based on national recommendations, including decreasing consumption of energy dense, low nutrient-dense foods, increasing consumption of nutrient-dense foods such as fruits, vegetables, whole grains, and lean sources of protein, and gradually increasing to 60 minutes of moderate-vigorous physical activity daily. The eating plan is guided by the traffic light system, whereby foods that are low in caloric density and high in nutrients (i.e., fruits and vegetables) are categorized as green, those that are higher in calories and also contain high nutritional value are deemed yellow, and those that are high in calories with minimal nutrient value are categorized as red.
Nutritional recommendations focus on increasing the number of green foods while decreasing the number of red foods consumed. The traffic light system has served as the foundation for a number of pediatric behavioral weight control interventions, with numerous studies documenting the effectiveness of this approach as part of a comprehensive lifestyle intervention, rather than a standalone approach. 33
Kurbo includes an integrated platform for youth to track each type of food consumed, and physical activities completed, which the coach can view through a web-based dashboard. The app includes food options from a variety of cultural backgrounds and is designed to address a broad age group, with recognition that different features may be more engaging to different age groups. Supporting materials are available in Spanish. The app is intended to be used in tandem with individual coaching sessions, which may be further tailored based on age, cultural background, and motivation. Coaching sessions are conducted via a centralized workforce, trained, and supervised through Kurbo.
Coaches are required to have a bachelor's degree and a health coaching credential or equivalent graduate degree in a related field. Coaches complete criminal background checks and extensive training on the Kurbo curriculum and behavior modification techniques to ensure program fidelity and client safety before intervention delivery. Training includes the importance of recognizing eating disordered behaviors and attitudes during coaching calls, as well as monitoring restriction of recorded dietary intake. In addition, an alert in the app is triggered with reported weight loss of greater than two pounds for more than two consecutive weeks or total weight loss exceeding 8 pounds in a month. Concerns and alerts result in the coach escalating the issue to a supervisor for consultation and follow-up as appropriate.
The initial individual coaching is 30 minutes, with subsequent sessions lasting ∼15 minutes. The goal of coaching sessions is to provide children and families with personalized feedback and customized action plans informed by data entered in the mobile app. Parents are asked to attend the first session and strongly encouraged to attend subsequent sessions. There are a number of strategies in place to increase parental engagement with the program, including a family workbook, a weekly meeting summary from the coach, and family cookbooks, to ensure parents are apprised of progress and goals even if they were not in attendance at a coaching session. Coaches are available to communicate with families in between coaching sessions via email, SMS or in-app chat to answer questions, schedule meetings, and re-establish engagement. All communication between coach and family is monitored through the web-based coach dashboard.
Measures
Demographics were limited to age and sex, entered by the child or parent at the time of enrollment. Participant's self-reported weight and height, assessed at baseline and follow-up, were used to calculate percentage of the 95th% for BMI (%BMIp95). %BMIp95 was selected as a primary outcome because it is sensitive to assessing weight status change in youth with high BMI and reduction of ≥5% has been associated with improvement in cardiometabolic risk factors in a large heterogeneous group of children.34,35 Information regarding number of coaching sessions completed, length of time enrolled in the program, and number of meals tracked was extracted from the Kurbo dashboard.
Statistical Analysis
Analyses were conducted in SPSS (Version 25). Measurement error was assessed through examination and exclusion of outliers (z-score ±3.0) on baseline and follow-up height, weight, and %BMIp95. No data were missing on any of the included variables. Hierarchical linear regression was used to examine the impact of baseline %BMIp95, number of coaching sessions, and length of time enrolled in the program on change in %BMIp95, controlling for baseline age and sex.
Additional analyses were conducted to further elucidate the relationship between length of program enrollment and change in weight status. Analysis of covariance, with sex and baseline %BMIp95 as covariates, was conducted to examine whether there were significant changes in weight status according to predetermined categories of length of enrollment, defined as 0–12 weeks, 13–26 weeks, 6–12 months, 12–18 months, and 18 months and longer. Independent samples t-tests were conducted to compare children (aged 5–12) and adolescents (aged 13–17) on key variables (%BMIp95, time enrolled, number of coaching sessions, and meals tracked). In addition, program engagement was examined through descriptive information, including number of coaching sessions and total number of foods tracked.
Results
Participants
A total of n = 8173 youth enrolled in the program. Of these, 4582 were excluded because they did not meet preestablished inclusion/exclusion criteria. An additional 91 participants were excluded because at least one of their data points was identified as an outlier. Application of these criteria resulted in a total of 3500 youth available for inclusion in study analyses. See Figure 1 for details. The mean age of included youth was 12.79 years [standard deviation (SD) = 2.41] and 71.3% were female. Baseline demographics are presented in Table 1. Females had significantly greater weight loss [%BMIp95; mean (M) = −4.76, SD = 8.05], t(1702.11) = 3.25 (p = 0.001) than males (M = −3.38, SD = 9.54). There was no significant difference between younger (5–12 years) children (M = −4.50, SD = 9.19) and adolescents (13–17 years; M = −4.40, SD = 7.70) on change in %BMIp95.
Baseline Descriptive Variables
BMI, body mass index; M, mean; SD, standard deviation.
On average, youth demonstrated a 0.70 U decrease in BMI (SD = 2.19) and a 4.45 U decrease (SD = 8.5) in %BMIp95 over a mean duration of 31.5 weeks (SD = 38.98). One-fifth (20%) of children decreased from one weight status category to a lower category (i.e., from severe obesity to obesity), while 5% of children increased weight status category. The overall regression predicting change in %BMIp95 was significant, R2 = 0.066, F(3,3494) = 77.18, and p < 0.001. Significant predictors included sex (b = −1.11, p < 0.001), baseline %BMIp95 (b = −0.58, p < 0.001), number of coaching sessions (b = −0.12, p < 0.001), and length of time enrolled in the program (b = 0.02, p < 0.001).
The direction of the relationships was such that being female, having higher baseline weight status, and participating in a greater number of coaching sessions were associated with greater change, while longer time enrolled in the program was associated with less change in weight status.
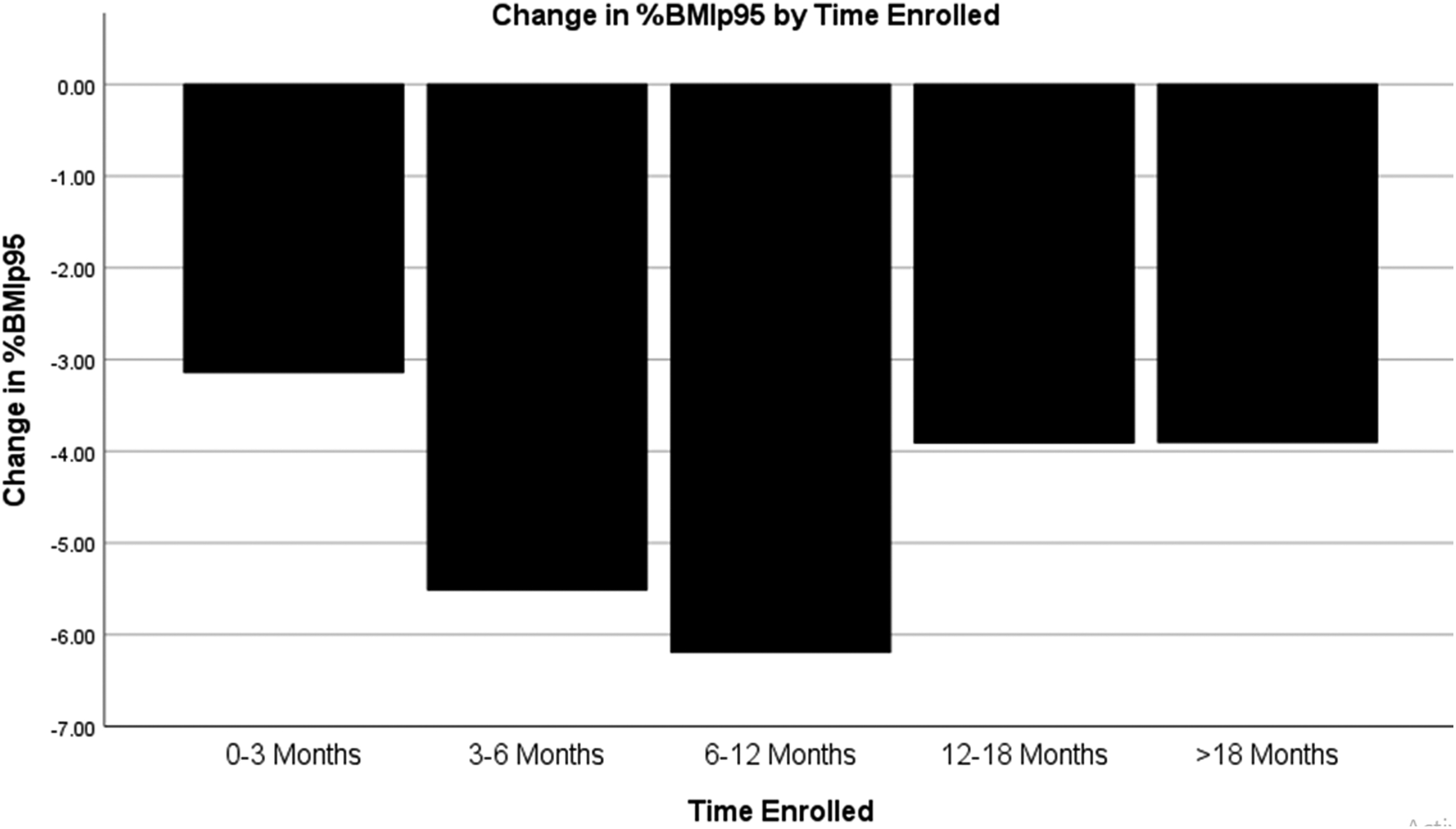
Analysis of covariance, controlling for sex and baseline %BMIp95, examined changes in weight status by time of enrollment and indicated a statistically significant difference in change in %BMIp95 by length of enrollment, F(4,2493) = 22.89, and p < 0.001. Post hoc comparisons between groups indicated statistically significant differences between all groups, excluding differences between 13–26 weeks and 12–18 months and 12–18 months and longer than 18 months. Figure 2 illustrates the association between length of time an individual was enrolled in the program and change in %BMIp95. Specifically, for individuals enrolled through 12 months, there was an apparent positive association between time in program and decrease in weight status. Beyond 12 months, there was a negative relationship, such that participants enrolled in the program for longer demonstrated less of a decrease.
Comparisons between children (aged 5–12 years) and adolescents (ages 13–17 years) revealed no significant differences on %BMIp95, meals tracked, or number of coaching sessions. There was, however, a significant difference between children (M = 34.69 weeks; SD = 42.21) and adolescents (M = 27.05 weeks; SD = 34.15) on length of time enrolled in the intervention t(3496) = 5.85, p < 0.001. On average, children were enrolled for 7.64 weeks longer than adolescents. Descriptive information concerning program engagement, as indicated by number of coaching sessions and total number of foods tracked, was also examined. Table 2 includes a breakdown of number of coaching sessions attended and number of foods tracked by these enrollment periods.
Completed Coaching Sessions and Foods Tracked by Time Enrolled in Program
Discussion
Overall, study findings suggest that use of a scalable program, including health coaching with integrated digital tools for monitoring diet and activity, can lead to significant reductions in weight status among children and adolescents. Across all participants, there was an average 0.70 U decrease in BMI (SD = 2.19) and a 4.45% decrease (SD = 8.5) in %BMIp95 over a mean duration of ∼7.5 months. While primary outcomes were assessed in different metrics, average reductions in weight status appear similar to those reported in family-based in person pediatric weight control interventions offered in community settings.36,37 The pattern of findings observed here also compares favorably to those reported from the Pediatric Obesity Weight Evaluation Registry (POWER), a consortium of multicomponent clinical pediatric weight management programs in the United States.
Findings from the large cohort of youth enrolled in this registry of face-to-face clinical programs indicated decreases in %BMIp95 of 1.88, 2.50, and 2.86 at 4–6 months, 7–9 months, and 10–12 months, respectively. Moreover, decreases of ∼5% points in %BMIp95 in this same registry were associated with some improvements in cardiometabolic function. 35
Significant predictors of decreased weight status included being female, higher baseline weight status, number of coaching sessions, and length of time enrolled in the program. These findings are similar to those reported from POWER, in which greater severity of obesity was associated with greater improvements in %BMIp95. 35 Unlike the findings reported from POWER, in which older age was associated with better outcome, there were no significant differences between children and adolescents enrolled in Kurbo with regard to change in weight status, suggesting program applicability across the age continuum.
Time enrolled appeared to be associated with better outcomes through 12 months, after which the pattern seemed to reverse. These data need to be interpreted with caution, as only 17.8% of the sample was enrolled beyond 12 months and available for this analysis. Given that the only available outcome data are from the time of program exit, it is possible that youth who remained enrolled beyond 12 months had previous successes that are not reflected in the final metric. It may also reflect the fact that individuals who were less successful remained enrolled in the program in hopes of future success, although this runs contrary to the more common observation that less success leads to earlier dropout. 38
Reported outcomes are similar to previous findings based on a smaller sample of youth who participated in the Kurbo program. The current findings also suggest a meaningful level of program engagement as inferred from mean number of coaching sessions completed. While the timing of when such sessions were completed is unknown, it is nonetheless noteworthy that for those who engaged with coaching, the average number of coaching sessions completed was fairly high. For example, the mean number of sessions for those enrolled for 0–12 weeks was 7, increasing to an average of 22 sessions for those who were enrolled from 6 to 12 months. This level of engagement is encouraging in light of the well-documented challenges associated with retention and engagement of participants in face-to-face pediatric weight control interventions and suggests increased feasibility of contact through videoconferencing.38–40
Remotely delivered health coaching sessions differ significantly from the common format for face-to-face visits in that they are typically shorter in duration and allow for considerably more flexibility in scheduling, thereby increasing accessibility, a factor noted by parents as key to supporting engagement. 41
This study is not without limitations. A significant limitation is that height and weight data were self-reported rather than measured, and the study design does not include comparison to a control condition or the ability to examine weight trajectories within participants. While there are limitations associated with parent report of categorization of child weight status, there are some recent data to suggest good sensitivity and specificity with parent estimated and measured height and weight. 42 In addition, information regarding race, ethnicity, socioeconomic status, and other variables, such as social determinants of health, were not collected, and may have impacted outcomes. The reason for this is that requesting such information was viewed as a barrier for enrollment in a commercial program.
Although we do not have individual level data regarding participant insurance status, historically children enrolled in Kurbo reflect a broad payor mix, including direct consumers (∼60%), those for whom participation is covered through employee benefit (∼35%), and Medicaid (∼5%). Examining outcomes based on enrollment is an important area for future research. Participants who elected to enroll in the program also had access to resources such as internet capability and access to a mobile device. These limitations notwithstanding, the data reported here reflect information collected from a large number of youth under real-world conditions and contribute to an emerging body of evidence regarding the effectiveness of mHealth interventions for pediatric weight control.
As noted by prior investigators, future research in this area would benefit from studies using well-controlled, rigorous designs to allow further examination of the effectiveness of mHealth interventions. 22 In particular, it would be informative to compare such programs to a comparison condition and include verified assessments of height and weight. It would also be instructive to examine the impact of programs combining digital platform with health coaching on psychosocial outcomes, including self-concept, mood, and eating disorder symptoms, all of which have shown improvements in face-to-face weight control interventions for youth and to examine cost effectiveness compared to more high intensity interventions.43–45 Finally, it is imperative to continue to conduct and publish research related to scalability of evidence-based pediatric weight management interventions, including commercial programs, to inform dissemination.
Impact Statement
Mobile health interventions hold promise as intervention for pediatric weight control. Findings from this retrospective cohort study suggest that a coaching program with integrated digital tools for monitoring diet and activity leads to reductions in self-reported weight status and warrants further study as a model for scalable intervention.
Footnotes
Acknowledgment
We acknowledge the Kurbo coaches and all the families who participated in the program.
Authors' Contributions
E.J.: conceptualization, methodology, and writing—original draft. K.D.: conceptualization, formal analysis, and writing—original draft. M.C.: conceptualization, resources, data curation, and writing—review and editing. T.R.: investigation, resources, and writing—review and editing. G.F.: conceptualization, writing—review and editing.
Funding Information
No funding was received for conduct of this study.
Author Disclosure Statement
E.J. was a consultant for WW International, Inc. G.D.F., M.I.C., and T.R. are full-time employees and shareholders of WW International, Inc. All other authors declared no conflicts of interest.