
Abstract
Background:
Metabolic and bariatric surgery (MBS) has been shown to be safe and effective for the treatment of adolescent obesity, yet many providers express hesitance to refer adolescents for surgery due to concerns for insufficient insurance coverage.
Methods:
The Healthy Lifestyle Clinic, a pediatric weight management clinic, was established in 2014, and an adolescent MBS program was added in 2017. Patients 15 years or older who meet the selection criteria are eligible for the surgery track. A retrospective chart review was conducted to describe our experience obtaining insurance approval for laparoscopic sleeve gastrectomy (LSG) for our adolescent patients.
Results:
Almost all patients who were interested in and eligible for LSG ultimately received insurance approval. Most patients had public insurance (70%). Sixty-four percent of patients were approved after the initial application, 23% were approved after a peer-to-peer review, and 11% required an appeal for approval. There was no difference in the time from insurance application to insurance approval based on age, race/ethnicity, or type of insurance.
Conclusions:
Age <18 years and having public health insurance have not been demonstrated as barriers to insurance approval for LSG in our cohort. Providers should not delay referral for MBS for eligible adolescents based on concern for insufficient insurance coverage. Adolescent MBS programs would benefit from a patient advocate to help families navigate the insurance approval process and reduce barriers to surgery.
Background
Severe obesity in adolescents continues to be a growing public health concern, and ∼8% of adolescents have severe obesity. 1 In addition to experiencing the immediate health effects of excess weight, obesity in adolescence is associated with an increased risk of premature mortality and morbidity in adulthood. 2 Metabolic and bariatric surgery (MBS) is a safe and effective treatment for adolescents with severe obesity3,4 and has sustained benefits for weight loss and remission of comorbidities. 5 Despite these well-documented benefits, MBS is an underutilized treatment option in adolescents, and there is often delay in referral for MBS in adolescents with severe obesity or the procedure is never offered.4,6
There are also significant disparities in the utilization of this treatment modality. Most adolescents undergoing MBS are female, White, and have private insurance. 7 Even though adolescents who are Black or Hispanic experience higher rates of obesity, Black and Hispanic adolescents are less likely to have MBS than White adolescents even after adjusting for type of insurance. 7
Although multiple factors contribute to providers' hesitance to refer eligible patients for MBS, including concern for complications and unfamiliarity with postoperative management, insufficient insurance coverage and the cost of surgery are perceived limitations that can inhibit referrals.8,9 In one survey of pediatric providers, fewer than 10% of pediatric providers had ever referred a patient for MBS, with cost being cited as one reason for not making a referral. 10
Adolescents pursuing weight loss surgery do have higher rates of denial for insurance approval than adults, with age <18 years being the most common reason for denial. 11 In a survey of private insurance companies, only 59% of private insurers would consider preapproval for adolescent MBS, and most would not approve MBS in this age group unless patients met specific nonevidence-based criteria, such as skeletal maturity. 12
In recent years, medical societies such as the American Academy of Pediatrics have sought to increase access to MBS for adolescents with severe obesity by providing evidence-based recommendations for practitioners and policy makers.8,13 The purpose of this study is to complement such recommendations by describing practical and effective strategies for pursuing insurance coverage. Specifically, this study describes insurance approval patterns for laparoscopic sleeve gastrectomy (LSG) in the first 3 years of an adolescent MBS program in the midsouth United States serving a population of primarily historically under-represented and publicly insured patients.
Methods
The Healthy Lifestyle Clinic (HLC) is an interdisciplinary pediatric weight management clinic in the midsouth established in 2014; 14 an adolescent MBS program was added in 2017. At the time of the study, there were 1800 patients in the HLC program, with an average of 86.9 referrals per month to the clinic during the study. The option of MBS as an adjunct treatment to lifestyle changes is discussed by an HLC medical provider with all active HLC patients who are ≥15 years and meet medical criteria based on guidelines from the American Society for Metabolic and Bariatric Surgery. 15
Indications for adolescent MBS include body mass index ≥35 kg/m2 or 120% of the 95th percentile with significant comorbidities such as obstructive sleep apnea (apnea/hypopnea index >5), type 2 diabetes mellitus, idiopathic intracranial hypertension, nonalcoholic steatohepatitis, Blount's disease, slipped capital femoral epiphysis, and/or hypertension; or body mass index ≥40 kg/m2 or 140% of the 95th percentile. 15
Comorbidities were diagnosed by appropriate medical subspecialists, and the presence or absence of comorbidities was determined by chart review. Demographics, including race, ethnicity, household income, and parental caregiver education, are self-reported as part of the initial HLC visit and documented in the electronic medical record. These data were abstracted during chart review. Similarly, gender and type of insurance were abstracted from the electronic medical record.
The patient's family is responsible for determining whether MBS is a covered benefit before pursuing surgery. Patients expressing interest in MBS are scheduled for an appointment with the adolescent MBS program and then begin the surgery track. The surgery track entails monthly preoperative visits with the pediatric metabolic and bariatric surgeon, medical provider and subspecialists, pediatric psychologist, dietitian, and exercise physiologist. During these visits, education about the LSG, nutrition, exercise, pre- and postoperative diet stages, and postsurgical expectations is delivered.
The multidisciplinary clinical team considers whether the patient and family have the ability and motivation to adhere to the recommended pre- and postoperative treatments. The decision to pursue MBS is a shared decision-making process between the patient, caregivers, and clinic providers. 16 The patients must also provide a letter of support from their primary care provider. After a minimum of 4–6 monthly visits to the MBS program, completing psychological evaluation, 17 ascertaining adequate family/social support, and demonstrating adherence to lifestyle changes, the decision is made to apply for insurance approval. The MBS coordinator, a registered nurse, completes the insurance application and subsequent correspondences with the insurance company.
This study is a retrospective chart review of all patients whose insurance approval for LSG was sought from September 2017 to March 2021. The research was conducted in accordance with the Declaration of Helsinki as revised in 2013. University of Tennessee Health Science Center Institutional Review Board approval was obtained to abstract study data. The analysis excluded one patient who did not have bariatric surgery as a covered benefit.
Study data were managed using Research Electronic Data Capture (REDCap) electronic data capture tools. REDCap is a secure web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry, (2) audit trails for tracking data manipulation and export procedures, (3) automated export procedures for seamless data downloads to common statistical packages, and (4) procedures for importing data from external sources.
All data reduction, processing, and analysis for this project were generated using SAS software, version 9.4 of the SAS system for Windows (SAS Institute, Cary, NC). Analysis of variance was performed to analyze the effect of patient characteristics by group on approval rates and timeline variables. Significance was set at p = 0.05.
Results
Patient Characteristics
Insurance approval was obtained for 43 adolescents and young adults undergoing LSG (Table 1). This cohort was 65% female and 75% non-Hispanic Black. The mean age at time of insurance approval was 17.3 ± 1.3 years, and the mean BMI was 53.9 ± 10.4 kg/m2. Most patients had public insurance (70%). Annual household income was ≤$30,000 for nearly half (42%) of the cohort, and less than a third (30%) of parental caregivers reported earning a college degree. Most patients had at least one comorbidity, the most prominent being obstructive sleep apnea (72%).
Patient Characteristics
Insurance Approval Rates
Almost all patients who were interested in and medically eligible for LSG ultimately received insurance approval (Fig. 1). Bariatric surgery was not a covered benefit under one patient's private insurance plan. The majority of patients were approved after the initial application for surgery (65%). The remainder of patients were approved after a peer-to-peer review (23%) or appeal (12%). The average time from a patient's initial visit with the metabolic and bariatric surgeon to insurance application was 239 days; this time range decreased over time from 2016 to 2020 (F = 5.01; p = 0.002).

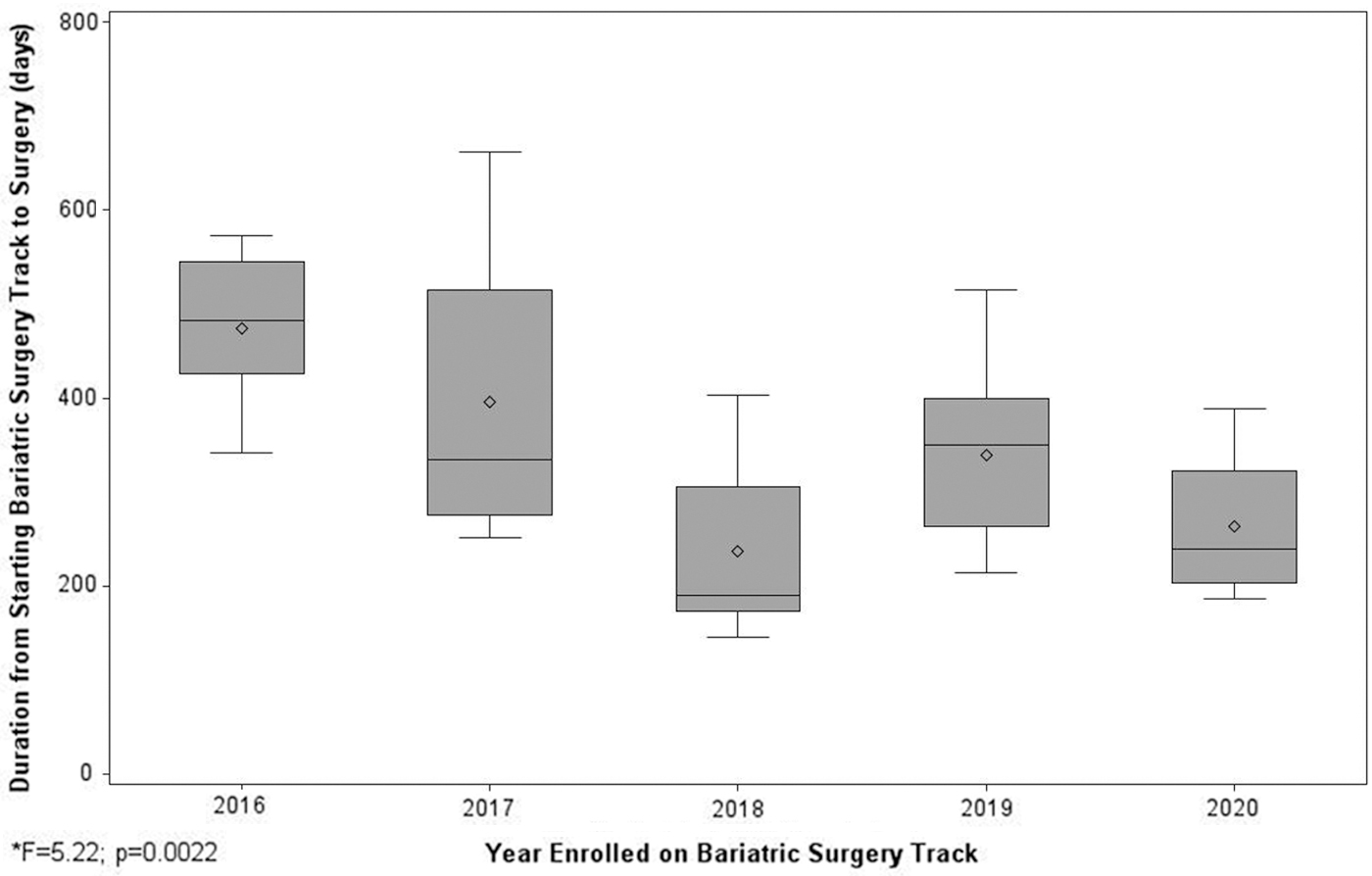
The average time from insurance application to insurance approval was 27 days; this time remained consistent from 2016 to 2020 (F = 0.53; p = 0.71). The average time from a patient's initial visit with the metabolic and bariatric surgeon to day of surgery was 328 days; this time frame decreased over time from 2016 to 2020 (F = 5.22; p = 0.002) (Fig. 2). Everyone in our cohort who obtained insurance approval of LSG went on to have the procedure.
Patient Characteristics and Insurance Approval
There was no difference in the time from insurance application to insurance approval when comparing patients under age 16 years with those >16 years (F = 0.67; p = 0.6). There was also no difference from application to approval by gender (F = 0.02; p = 0.8), racial group (F = 0.56; p = 0.5), or type of insurance (F = 1.89, p = 0.15). However, insurance approval for patients with higher BMIs took longer than for patients with lower BMIs (F = 3.23; p = 0.049).
Discussion
In our cohort of adolescents and young adults with obesity who predominantly have public insurance, nearly all patients who were eligible for MBS were approved for the LSG by their insurance company. Most patients were approved after the first insurance application; however, some required an appeal or a peer-to-peer review. The average time from insurance application to approval was consistently just under 4 weeks. However, the average time from a patient's initial MBS visit to insurance application decreased over time. The average time from a patient's initial MBS visit to the day of surgery also decreased over time, suggesting that our program's maturation, not improvement in insurance approval time, resulted in shorter times to surgery. We believe that once a patient is deemed to benefit from MBS, the education process about perioperative complications and lifestyle changes associated with MBS should be efficient. The insurance application should also be timely, as all of our patients who were approved for LSG went on to have the procedure.
In contrast to most adolescent MBS patients who are White and have private insurance, 7 our cohort is predominantly Black and publicly insured. Perceived lack of insurance coverage is one reason providers are reluctant to refer adolescent patients for bariatric surgery; 9 however, MBS was covered by a wide range of insurers in our cohort, and we did not see a significant difference in the amount of time required for insurance approval based on age. Paradoxically, it took more time to obtain insurance approval for patients with higher BMIs than patients with lower BMIs, creating potential barriers for the patients who may benefit most from surgery. All but one patient requiring an appeal, which considerably lengthens the insurance approval process, had a BMI ≥60 kg/m2. This finding highlights the importance of education regarding the exacerbation of risk associated with delaying treatment for adolescents with severe obesity. 18 Future research should examine the potential roles of weight-related stigma and discrimination. 19
In our multidisciplinary program, the entire clinical team works collaboratively to support patients through the preparation phases that lead up to seeking insurance approval for MBS. The MBS coordinator (a registered nurse) applies for insurance approval and serves as a patient advocate during this process. Before and after insurance application, the MBS coordinator is in frequent contact with the insurance company and with the patient's family. Previous studies have discussed that Black patients are less likely to successfully navigate the appeal after denial for bariatric surgery. 7 We believe that having a patient advocate who is persistent during the insurance approval process has been essential to reducing systemic barriers to insurance coverage. In addition, the MBS coordinator empowers patients and families to be selective and intentional about choosing their insurance providers as some private companies do not provide MBS as a covered benefit.
Limitations
This is a single institution study and the results are not widely generalizable. However, patients in this cohort are from three different states, representing more than one state's public insurance program. In addition, insurance approval for MBS does not always translate to payment for the hospital, which was not investigated in this study.
Conclusions
Public insurance is not a barrier to obtaining insurance approval for LSG. Primary care providers should be prompt to refer adolescents who might benefit from MBS, regardless of their payer status.
Impact Statement
Pediatric providers should not delay referral for metabolic and bariatric surgery (MBS) for eligible adolescents due to concerns for insufficient insurance coverage. Adolescent MBS programs benefit greatly from a designated patient advocate to help patients and families navigate the insurance approval process.
Footnotes
Acknowledgments
We acknowledge the support of the Memphis Research Consortium, Le Bonheur Children's Foundation Research Institute, and Urban Child Institute. In addition, we acknowledge the expertise and assistance of Joan C. Han, MD.
Portions of this study were presented in a poster session at The Obesity Society Annual Scientific Meeting, 2019, Las Vegas, NV.
Authors' Contributions
E.W.G. contributed to conceptualization, formal analysis, investigation, methodology, and writing—original draft. W.A.S. was involved in conceptualization, data curation, formal analysis, methodology, and writing—reviewing and editing. E.T.B. carried out conceptualization and writing—reviewing and editing. D.H. took care of investigation and writing—reviewing and editing. A.O. carried out writing—reviewing and editing. Y.Z.W. was in charge of conceptualization, formal analysis, methodology, and writing—reviewing and editing.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.