
Abstract
Background:
Challenges to treat excess weight in primary care settings include time constraints during encounters and barriers to multiple visits for patient families, especially those from vulnerable backgrounds. Dynamo Kids! (DK), a bilingual (English/Spanish) e-health intervention, was created to address these system-level challenges. This pilot study assessed the effect of DK use on parent-reported healthy habits and child BMI.
Methods:
In this 3-month, quasi-experimental cohort design, DK was offered to parents with children aged 6–12 years with BMI ≥85th percentile in three public primary care sites in Dallas, Texas. DK included three educational modules, one tracking tool, recipes, and links to internet resources. Parents completed an online survey before and after 3 months. Pre-post changes in family nutrition and physical activity (FNPA) scores, clinic-measured child %BMIp95, and self-reported parent BMI were assessed using mixed-effects linear regression modeling.
Results:
A total of 73 families (mean child age = 9.3 years; 87% Hispanic, 12% non-Hispanic Black, and 77% Spanish-speaking families) completed the baseline survey (participants) and 46 (63%) used the DK site (users). Among users, pre-post changes (mean [standard deviation]) showed an increase in FNPA scores (3.0 [6.3], p = 0.01); decrease in child %BMIp95 (−1.03% [5.79], p = 0.22); and decrease in parent BMI (−0.69 [1.76], p = 0.04). Adjusted models showed −0.02% [95% confidence interval: −0.03 to −0.01] change in child %BMIp95 for each minute spent on the DK website.
Conclusions:
DK demonstrated a significant increase in parent FNPA scores and decrease in self-reported parent BMI. e-Health interventions may overcome barriers and require a lower dosage than in-person interventions.
Introduction
Childhood obesity remains a persistent epidemic in the United States (US) with immediate and future concurrent health risks that include cardiovascular disease; diabetes; cancers such as gastric and colorectal cancers; and death.1,2 Important aspects of the childhood obesity epidemic in the US include its deepening and widening disparities and high economic costs.3–9 Specifically, 19.3% of US children aged 2–19 years have a BMI ≥95th percentile adjusted for age and sex (%BMIP95), 10 defined as having obesity, but the prevalence is even higher among non-Hispanic Black (20.4%) and Hispanic youth (23.6%), compared with non-Hispanic White youth (14.7%).9,11–13
Even more troubling, the rate of change in BMI doubled from 0.052 to 0.100 kg/m2/month in US children aged 2–19 years during the COVID-19 pandemic, compared with the prepandemic period, 14 heightening the need to address obesity 7 in postpandemic recovery efforts.
To address childhood obesity, the Obesity Chronic Care Model 15 recommends that (1) children's weight statuses be evaluated at health care practices; (2) providers establish a relationship with the family that focuses on weight in a health context (vs. appearance); and (3) parents or guardians (hereafter “parents”) understand that OW/OB are medical diagnoses. Indeed, studies have shown that children with excess weight benefit from comprehensive, family-based, moderate- to high-intensity weight control interventions.16–18
Yet, the US health care system is not currently able to deliver intensive interventions that adhere to US Preventive Services Task Force (USPTF) best practices, especially for the most at-risk populations due to limited time in clinical visits, insufficient financial resources, and lifestyle barriers such as lack of time, transportation, or child care.16,19 Moreover, addressing pediatric obesity through primary care is difficult for providers who often lack the time, knowledge, and skills to be effective. 15
Similarly, families are challenged by disrupted schedules and medical information about weight management that may be delivered in an inconvenient and/or not culturally congruent manner.20,21 Moreover, vulnerable populations may not have a trusted provider or health insurance coverage to afford the necessary care. 16
While e-health interventions may be a strategy to address the provider and patient barriers to obesity care mentioned above, research on their efficacy is limited. Existing studies focus on mobile alerts or telehealth engagement instead of personalized/independent online programs. 22 Yet, according to the USPTF, effective obesity treatment programs should be multicomponent, address behavior change, include at least 26 hours of exposure, and last for 2–12 months. 16 Moreover, parents play a critical role as the family environment is predominant in development of children's eating and physical activity behaviors.23–25 Yet, it is unknown if these recommendations apply to a self-paced, tailored, e-health delivery model.
This study aimed to assess the efficacy of Dynamo Kids! (DK), an e-health, family-based, self-paced, and personalized pilot intervention, on improvement in child and family obesity-mitigating behaviors, as well as child and parent BMI. It was hypothesized that participation in the DK intervention would (1) improve child and family obesity-mitigating behaviors, as measured by family nutrition and physical activity (FNPA) scores; (2) decrease %BMIP95 in child participants; and (3) decrease self-reported BMI in parent participants.
Methods
Study Design
This quasi-experimental (uncontrolled) cohort study enrolled 100 families from 3 public primary care centers in Dallas, TX. Participant families were asked to utilize DK for 3 months and were evaluated before they were exposed to any content and after they completed the intervention. This study was reviewed and approved by both UTHealth and UT Southwestern institutional review boards (STU 2019–0876) and developed in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines (Supplementary Data). 26
Study Population
The study population comprised vulnerable racial and ethnic minority families with children aged 6–12 years who attended a primary care center that was part of the public hospital system. The pilot study was intentionally launched in three neighborhoods that are predominantly inhabited by minority populations, which are generally hard to reach; however, the clinics see patients from all racial and ethnic backgrounds.
Eligibility and Recruitment
Parents who met the following eligibility criteria were included in the study: (1) had a child 6–12 years of age; (2) the child was a patient of the participating providers at three outpatient practices; (3) the child had a BMI ≥85th percentile at that appointment; and (4) the parent spoke either English or Spanish. Children with a chronic condition that prevents typical physical activity (e.g., used a wheelchair) or requires an atypical diet (e.g., gastrostomy feeds or type 1 diabetes) were excluded. Recruitment occurred from August 2020 to April 2021.
Providers received an electronic health record (EHR) alert and referral link when family met inclusion criteria at a well-child visit. After receiving the referral, a study coordinator called parents to establish eligibility, obtain verbal consent, and enroll the family in the DK intervention. Consent was obtained only from the parent because the intervention was directed toward the parents of the child with OW/OB rather than to the child.
Before beginning the intervention, participants were required to complete a baseline research survey (Supplementary Appendix SA1).
Study Procedures
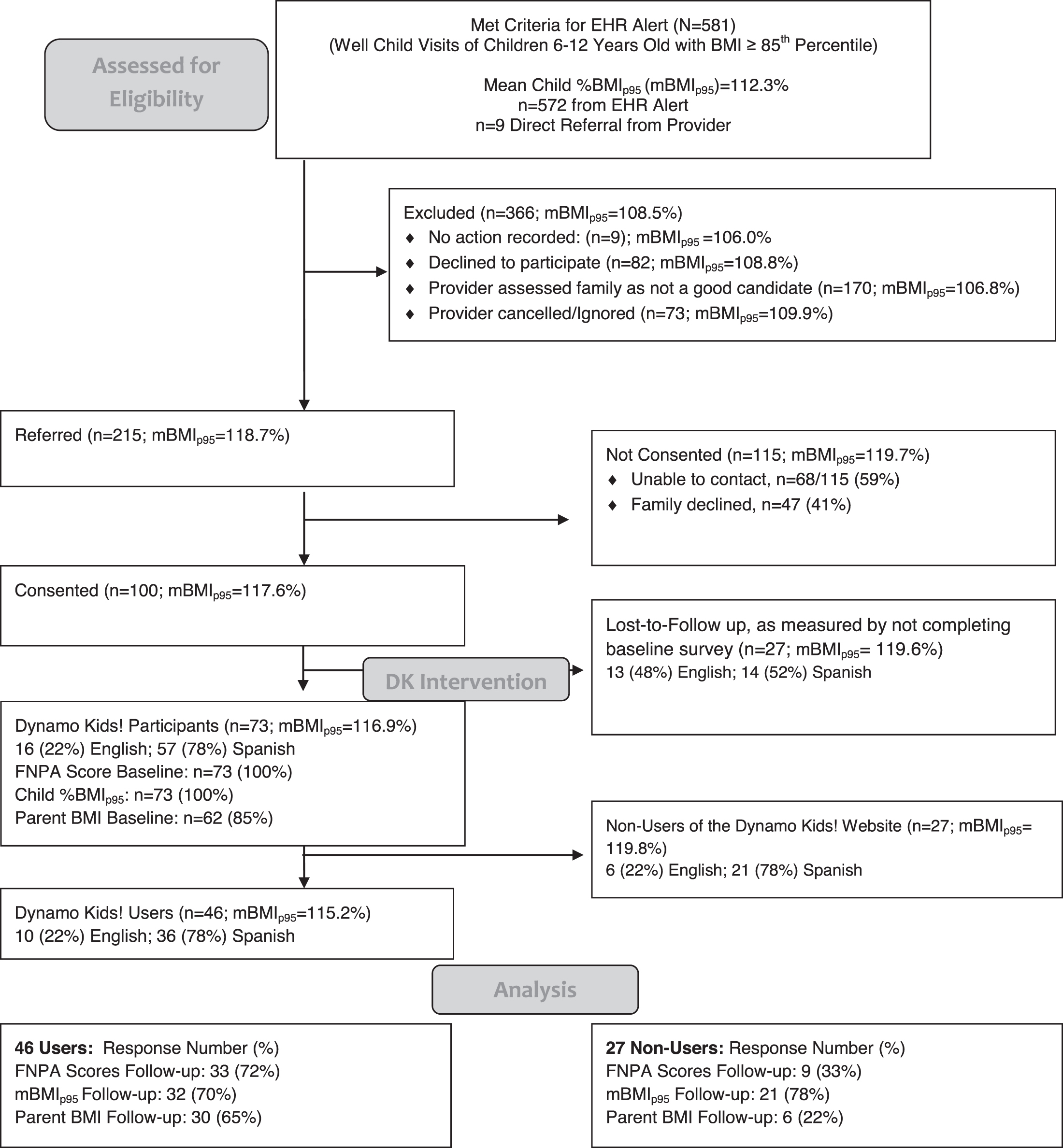
Based on child inclusion criteria, an EHR alert identified 575 eligible patients; and providers identified 6 patients outside the EHR alert. Providers referred 223 patients; 100 consented to participate. Of the 100 consented parents, 73 completed the baseline survey and 46 used the DK website (Fig. 1). Baseline child weight and height were extracted from the EHR at the well-child visit when the EHR alert fired.
Intervention Description
DK is a family-based, e-health pilot intervention that is guided by the Obesity Chronic Care Model.27,28 This technology-based, customized, self-paced, and self-directed intervention includes an online portal in both English and Spanish, which parents access to learn strategies to improve specific health behaviors for their children. Additionally, the website intervention includes two practice-based features: (1) an EHR-embedded alert that appears when DK inclusion criteria are met and (2) a customized report based on patient website use, with talking points for providers at a follow-up clinical visit. 29
DK is intended to extend brief primary care counseling using an e-health format, with the capacity for exposing families to hours rather than minutes of weight management support. Specifically, the DK foci were to reduce consumption of sugar-sweetened beverages, increase physical activity levels, and adhere to MyPlate recommendations. Tables 1 and 2 provide details of DK; a description of development and protocol is published elsewhere.27,29
Dynamo Kids! Intervention Characteristics and Content
DK, Dynamo Kids!; PA, physical activity; SSB, sugar-sweetened beverages.
Sample Dynamo Kids! Education and Engagement Plan, Stratified by Module
Each module (SSB, PA, and MyPlate) has the same 4-week structure. Participants can choose the order in which they engage with each topic, and upon completing one module (e.g., PA), they can select the module they want to continue with in week 5 (e.g., MyPlate) and then begin their final module in week 9.
OW/OB, overweight and obesity.
Outcome Measures
Primary outcome
The pre-post change in FNPA screening composite scores30,31 used to measure parent-reported healthy home environment and parenting practices was the primary outcome. The FNPA survey 32 is a validated 20-question survey, available in both English and Spanish; it has been shown to be effective at predicting children's risk for having OW/OB. 25
Secondary outcomes
Secondary outcomes included (1) age- and sex-specific %BMIp95, calculated based on the 2000 CDC growth charts 33 using child height and weight collected using the Health-o-Meter professional tool during clinical visits, which were extracted from the EHR; and (2) parent self-reported height and weight from baseline and follow-up surveys, which were used to calculate BMI.
Follow-up child measurements were extracted from the EHR at the planned weight-focused visit following the intervention or (if the visit did not occur) at the next visit, up to 14 months after the referral visit, allowing time for an annual well-child visit to occur.
Primary exposure
The primary exposure variable was the total number of minutes that families spent and stored on the DK website.
Covariates
Child sex, time between the well-child visit and follow-up visit, and age were primary covariates collected through the EHR. Child race/ethnicity, parent's educational attainment, parent's age, food insecurity status, parent perception of their child's weight, and the family's language preference (English or Spanish) collected using the baseline participant survey were additional covariates.
Statistical Analyses
Descriptive statistics were performed on all variables, both aggregate and stratified by DK user status (i.e., participants who used the DK website [users] and participants who did not use the DK website [nonusers]). Bivariate analyses included correlation coefficients, t-tests, χ 2 , or Fisher exact tests, as appropriate, to assess the relationship between the three dependent outcomes and all independent variables, including user status.
Bivariate analyses were conducted to determine if missing data were missing completely at random. Given that the multiple imputation estimates and standard errors were very different from those in the complete case analysis, the missing data mechanism was assumed to be informative. 34
Hence, we limited our interpretation to multiple imputation to estimate the missing data: we produced 11 values for parent baseline BMI, 6 values for food insecurity, 14 values for time between baseline and follow-up measurements, 31 values for the change in FNPA survey, 14 values for the change in child %BMIp95, and 37 values for the change in parent BMI. Then, we used mixed-effects modeling to identify significant predictors of the change in the three outcomes of interest.
Linear mixed-effects repeated-measures models assessed the effect of DK on the three outcomes of interest and accounted for clustering within participants over time. Multiple imputation using chained equations imputed missing outcomes for the six variables with missing data. 25 Covariates were selected for inclusion based on literature35,36 reporting an association with weight status or when significantly correlated (at a p ≤ 0.05 level).
All data analyses were conducted using Stata 16 (StataCorp 2019, College Station, TX).
Results
For the children of the 73 participants (46 [63%] users and 27 [37%] nonusers), the baseline mean (standard deviation [SD]) age was 9.3 (1.79) years; 60% were male; 88% were Hispanic and 12% were non-Hispanic Black; 78% preferred Spanish content; 88% had annual household incomes <$40,000; and 56% reported food insecurity in the previous year (Tables 3 and 4). Slightly more than half (55%) of the participants completed the follow-up survey (33 [72%] users and 7 [26%] nonusers).
Descriptive Characteristics of the Children and Family Household Resources in the Study Sample
Bold text denotes statistically significant value.
Difference between users and nonusers.
t-Test; bχ 2 test; cFisher's exact test; dmissing data for one user (2.2%); emissing data for one user (2.2%); and fmissing data for three nonusers (11.1%) and three users (6.5%).
Descriptive Characteristics of Parents in the Study Sample
Difference between users and nonusers.
χ 2 test.
Fisher's exact test.
A total of 28 (38%) participants attended a planned follow-up visit (21 [46%] users and 7 [26%] nonusers). Among users, 21 (46%) had measures from weight-focused follow-up visits vs. 16 (35%) from other visit types. Among nonusers, 7 (26%) had measures from weight-focused follow-up visits vs. 15 (56%) from other visit types. The mean (SD) days between baseline and follow-up anthropometric assessments was 269 (107.84) days. The mean (SD) number of minutes spent on the DK website was 144.39 (132.08) minutes, with a range from 4 to 476 minutes.
Families with girls were more likely to use the DK website (χ 2 = 8.05, p = 0.005). Characteristics associated with increase in FNPA scores included younger child age (ρ = −0.39, p = 0.03) and parents older than 35 years (t = 2.48, p = 0.02). Girls (t = 2.01, p = 0.05) were associated with a higher baseline child %BMIp95, and older parents (ρ = 0.27, p = 0.02) were associated with a decrease in child %BMIp95. A higher baseline child %BMIp95 (ρ = 0.35, p = 0.01) and lower educational level (ρ = 0.34, p = 0.01) were associated with a higher baseline parent BMI (Table 5).
Baseline Family Nutrition and Physical Activity Scores, Child BMIp95 Measures, and Parent BMI
Difference between users and nonusers.
t-Test.
Fisher's exact test.
FNPA, family nutrition and physical activity; SD, standard deviation.
Complete case analysis of the outcomes was performed for all enrolled participants and for the subset of DK users (Table 6). FNPA scores (primary outcome) improved among all enrolled participants (3.5 [SD = 6.95], p = 0.002) and among DK users (3.0 [SD = 6.25], p = 0.13).
Change in Three Dependent Outcomes (Family Nutrition and Physical Activity Scores, Child %BMIp95, and Parent BMI) Among Participants: Complete Case Analysis
Bold text indicates statistical significance.
Paired t-test analysis.
Users were defined as participants who logged into the DK website and opened one of the modules at least twice.
Decrease in mean child %BMIp95 was seen in all enrolled participants and DK users, but was not significant: among all enrolled participants, Δchild %BMIp95 = −0.53 (SD = 5.52), p = 0.39, and among DK users, Δchild %BMIp95 = −1.03 (SD = 5.79), p = 0.22. Self-reported parent BMI change was not significant among all enrolled participants (−0.51 [SD = 1.69], p = 0.08), but reached significance among DK users (−0.69 [SD = 1.76], p = 0.04).
In the multiple imputation models for FNPA and self-reported parent BMI, no covariates were significantly associated with change in score. However, in the Δchild %BMIp95 model, the time between the initial and follow-up visits that were the source of the clinical measurements was significantly associated with an increase in child %BMIp95, and the amount of time spent on the DK website was significantly associated with a decrease in child %BMIp95.
Specifically, while adjusting for all other covariates, a 1-day increase in time was associated with an increase in child %BMIp95 (0.015% confidence interval [95% CI: 0.002–0.03]) and a 1-minute increase in total minutes spent on the DK website was associated with a decrease in child %BMIp95 (−0.02% [CI 95%: −0.03 to −0.01]) (Table 7).
Mixed-Effects Repeated-Measures Linear Regression Modeling of Demographic and Dynamo Kids! Usage Predictors of Primary Outcome [Family Nutrition and Physical Activity Score Change] and Secondary Outcomes [Child %BMIp95 and Parent BMI Changes]
Missing data are shown to be missing completely at random for the following covariates: parent baseline (15%) and follow-up BMI measures (51%), food insecurity status (8%), follow-up FNPA score (42%), follow-up child BMIp95 (19%), and time between baseline measures and follow-up visit (19%). All models were performed using multiple imputation mixed-effects multivariate linear regression.
p < 0.003.
p < 0.02.
%BMIP95, BMI as a percent of the 95th percentile; CI, confidence interval; GED, General Education Development; Ref, reference category; SE, standard error.
Discussion
DK, a pilot, e-health family-based program for addressing pediatric excess weight in primary care, was successfully implemented in multiple primary care centers, with improvement in healthy family routines among hard-to-reach, high-risk vulnerable populations for childhood excess weight (Table 6). Reduction in parent BMI was significant only for parent BMI among DK users, but time on the website predicted improvement in child %BMIp95 in the regression model, suggesting intervention benefit.
Given the increasing prevalence of and disparities within pediatric OW/OB, 9 DK shows potential for addressing a vexing public health and clinical challenge that has both proximal and distal health consequences for patients and health care systems.
Compared with other studies using the FNPA tool as a primary outcome, this study showed a lower score at baseline and a smaller change in score over time.37–39 Whereas previous research focused predominantly on non-Hispanic White populations with healthy weight, this study population included only racial and ethnic minority participants with excess weight.38,40 Importantly, the FNPA tool has not been validated in exclusively racial and ethnic minorities.
Moreover, while research has shown that an increase of 10 points in the FNPA score corresponds to a decrease of 0.17 BMI units, research has not demonstrated what change in points is required for an observable behavioral change.31,41 Additionally, the lower baseline scores may reflect less healthy behaviors, and the smaller change may reflect the intensity of program use. 39
Among DK users, the improvements in FNPA scores and parent BMI are notable because DK use was objectively tracked. The association between child %BMIp95 and time on the website using multivariable regression suggests that parents who used the website implemented healthy behaviors for their children. Importantly, OW/OB BMI trajectories for this age group were magnified during the COVID-19 pandemic when this study was conducted, so any reduction may indicate a benefit, especially compared with the increase in child %BMIp95 for this population during this time period.37,42
Provider adherence to expert guidelines for weight management within primary care encounters may be poor. 15 One study showed that primary care providers can motivate families to use self-guided tools to achieve short-term weight improvement. 43 Technology-assisted delivery of weight management within primary care has been limited to hybrid group programming 44 or low-quality telehealth engagement or mobile alerts that found minimal or no effect. 22 DK is innovative as all components are digital and the educational component is self-paced and self-directed. However, given the intervention's novelty, the expected dosage, usage, and acceptance could only be surmised based on the intervention's needs assessment. 27
The relationship between exposure time and child %BMIp95 demonstrates the importance of intervention dosage, as recommended by USPTF guidelines, 16 and raises the question of whether e-health interventions and in-person interventions require the same intervention dosage. While designed to be a 12-hour intervention based on the information ascertained in the needs assessment, 27 this intervention in this population during this time period was a lower-intensity intervention as participants opted to use the DK website, on average, for ∼2.5 hours compared with the recommended 26 hours.
The significant findings are noteworthy at a low-intensity intervention because new research demonstrates how high-intensity interventions create barriers for patient engagement. 45 e-Health programs such as DK may improve engagement by allowing patients to engage on their own time and device in their own space and personalized manner. Importantly, a follow-up implementation science evaluation, perhaps using a standardized framework such as RE-AIM (reach, effectiveness, adoption, implementation, and maintenance),46,47 would help identify the impact of and need for tailoring DK for diverse populations and settings.
Study Limitations and Strengths
There are several study limitations. A lower than expected proportion of participants used the website and/or did not return for a follow-up visit. Additionally, the follow-up clinical measures were collected at visits with varying follow-up time. COVID-19 may be an explanation for high attrition, given patient concerns about other health issues, and also an explanation for low use, given competing parent demands during a tumultuous time.
Furthermore, given the survey length, survey completion was relatively low, a documented phenomenon,48,49 although completers and noncompleters did not differ in baseline characteristics. However, non-COVID-19 clinical weight management programs commonly face high dropout rates. 50 Moreover, without a control group, the relative impact of the intervention is unknown, an important question especially during COVID-19 when a comparison group could have had higher than typical BMI change.14,37
In addition, because parent weight was self-reported, social desirability bias may be present and help explain why parent BMI may have significantly dropped and child %BMIp95 did not. Finally, the small sample size prevented subgroup analyses, which limits the generalizability of our findings.
Study strengths include the entirely virtual format of the intervention, which proved necessary during the COVID-19 pandemic and provided an immediate solution to treat pediatric OW/OB. Importantly, we successfully reached high-need populations who are disproportionately affected by OW/OB and typically lack access due to program availability and/or barriers to access (63% of participants used the DK website).
Aligned with the Obesity Chronic Care Model, DK was integrated into the health care system so that the diagnosis and physiological measurements took place in a clinical setting, while the intervention was home based and accessible online. This format is scalable and aligns with patient preferences. Thus, DK proved to be a response to common barriers of language, internet, time, and transportation for users.
Conclusions
DK, an e-health pilot intervention, demonstrates that e-health interventions may be feasible for some low-income predominantly Hispanic families and may have impact among users in terms of improving parenting behaviors and reducing BMI and child %BMIp95, even during the COVID-19 pandemic. Larger controlled studies are needed to assess effect size and conduct subgroup analyses, as well as to assess the integration of additional implementation outcomes, to understand low uptake and for effective translation to other settings and populations.
However, a simple solution to childhood weight management is unlikely. Therefore, sustainable scalable interventions that target vulnerable children and that show even modest benefits may contribute to multilevel changes that impact childhood OW/OB.
Impact Statement
We provide a quantitative evaluation of the efficacy of Dynamo Kids!, a pilot, self-paced, customized e-health intervention informed by the Obesity Chronic Care Model, which was implemented in public primary care sites for parents of pediatric patients aged 6–12 years who have overweight and obesity (OW/OB).
Footnotes
Acknowledgment
The authors would like to acknowledge Mr. Lionel Santibáñez for his editorial assistance. The University of North Carolina (UNC) at Chapel Hill Connected Health for Applications and Interventions Core services received support from the National Institutes of Health (grant no. P30DK056350; PI, Mayer-Davis and Shaikh) to UNC Nutrition Obesity Research Center and National Cancer Institute (grant no. P30CA16086; PI, Earp) to the UNC Lineberger Comprehensive Cancer Center. Agency for Healthcare Research and Quality R24 (grant no. HS022418; PI, Halm) provided a pilot award for formative interviews. Institutional support from Children's Health, Children's Medical Center of Dallas for Web site creation.
Authors' Contributions
J.S.Y. drafted the full manuscript, developed the analysis plan, was responsible for manuscript edits, and prepared the manuscript for submission. He also served as a project team member in all phases, from development through evaluation. M.A.A. served as a coprincipal investigator and was responsible for project ideation, implementation, and evaluation. She also provided feedback on the final manuscript. F.D.A. served as a subject matter expert who approved the analysis plan and provided feedback on the final manuscript. C.A.G. and S.E.M. served as subject matter experts who provided feedback on the final manuscript. S.E.B. is the principal investigator and was responsible for project ideation, implementation, and evaluation. She provided significant feedback and insight throughout the manuscript writing process and on the final manuscript.
Ethical Approval
This study was approved by the Institutional Review Board at UTSW and the Committee for the Protection of Human Subjects at UTHealth School of Public Health.
Funding Information
This study was partially supported under a pilot funding mechanism from the AHRQ-sponsored patient-centered outcomes core facility at UT Southwestern (Grant Number: 5R24HS022418-05)
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.