
Abstract
Background:
Pediatric obesity is a growing concern in the United States and has been linked to negative psychological health outcomes such as depression, anxiety, and decreased quality of life. Obesity is a complex disease that is influenced by several environmental and social factors that are often out of an individuals' control. The etiology of pain in youth with obesity is not well understood. There are likely many factors that overlap and influence each other, including those related to functional limitation, sleep quality, and psychological health that exacerbate symptoms as a whole.
Methods:
This study examined the relationship between obesity level (BMI z-score) and youth self reports of: pain, functional limitation, sleep quality, depressive symptoms, and health-related quality of life (HRQoL). Ninety-eight patients completed validated surveys of pain, pain burden, functional disability, sleep, depression, and HRQoL as standard of care during their initial visit in Weight Management Program at Connecticut Children's Medical Center. Indirect effects of pain measures (pain scores and pain burden) on HRQoL through functional limitation, sleep quality, and depressive symptoms, respectively, were tested using bootstrapping according to Hayes.34
Results:
Significant indirect effects and full mediation for both models were found.
Conclusions:
This study uniquely contributes to existing research through the discovery of the serial mediating effects of these variables in the relationship between youth pain and HRQoL. Although these variables have been studied independently as influential in this relationship in past research, this is the first study to examine how they interact through serial mediation models.
Introduction
The obesity epidemic is a long-standing problem in the United States. Among U.S. adults, general obesity prevalence has increased from 35.4% in 2011–2012 to 43.4% in 2017–2018, an 8% difference. 1 Obesity among children and adolescents over the past few decades has significantly increased as well and is a serious public health concern. 2 Obesity rates have been shown to be as high as 20.9% for boys and 18.5% for girls in the United States, with Hispanic youth having obesity prevalence rates of 26.2%. 3 In addition, non-Hispanic Black youth had significantly higher rates of obesity (24.8%) than non-Hispanic White (16.6%) and non-hispanic Asian (9.0%) youth aged 2–19 years old. Obesity is an incredibly complex disease that is influenced by several factors including environment4,5 and psychosocial variables. 6 Mental health is often much poorer in teens who are overweight or obese. 7 Compared with groups of healthy-weight youth, obesity is related to increased risk for reduced quality of life, anxiety, and depression. 6 One study found that compared with children with normal weight, children with obesity had significantly higher scores on scales measuring internalizing (e.g., social withdrawal, anxiety and depressive symptoms) and externalizing (e.g., aggression, delinquency) behaviors. 8
Pain, an understudied aspect of obesity, has a significant impact on the etiology and course of obesity. One review states that obesity is essentially a proinflammatory state, and that inflammation can cause pain. 9 In addition, mechanical stresses on the body owing to excess weight eventually leads to the breakdown of cartilage in the joints as well, causing further musculoskeletal pain, which releases more proinflammatory cytokines.10,11 Neurologically, these cytokines released in individuals with obesity shifts the balance of the neurotransmitter serotonin, which can lead to depression. 12
Although most research has focused on obesity-related pain in adults, it commonly occurs in youth as well. One study found that 47% of youth with obesity reported having pain, with 42% having severe pain. 13 Pain was most commonly reported in the ankles, knee joints, lower back, and during physical activity. BMI was also positively related to the number of pain locations. Other studies have found increased risk for back pain, 14 bone and joint problems, 15 and limitations in physical activity owing to pain 16 in children and adolescents with obesity, especially as BMI increased. In a study of adults with obesity and chronic pain, quality of life related to physical functioning decreased, and depressive symptoms increased as BMI levels rose. 17 A separate study examining adults with primary fibromyalgia syndrome found that patients who had comorbid obesity reported significantly higher levels of pain, depression, and poor sleep quality compared with those who were of normal weight or overweight. 18 When examining chronic pain, it is important to understand that pain is multifaceted, and not only includes numeric ratings of pain perception, but also its impact on everyday life and functioning (e.g., school attendance, being able to take care of oneself). This daily interference caused by pain can be termed pain burden, which has been established as an important measure that provides additional insight on the impact of pain. Validation studies for pain burden measures have identified negative relationships to activity limitations and quality of life among youth.19,20
Poor sleep quality has been found to dysregulate the balance between leptin and ghrelin, two important appetite-related hormones, which can lead to increased caloric intake and weight gain. 21 A study of adolescents with chronic pain and obesity found higher levels of leptin and C-reactive protein, an important inflammatory marker, among those who had obesity and chronic pain compared with those who had only chronic pain or obesity alone. 22 BMI z-score has also been found to be a significant predictor of worsened sleep quality and reduced quality of life among youth with obesity. 23 Of interest, whereas poor sleep quality was related to depressive symptoms and lower quality of life ratings, the relationship between symptoms of depression and sleep quality was not related to obesity level. 23
Although there have been studies that examine the individual relationships between variables related to pediatric obesity and chronic pain,16,22,23 there is little to no research on how these factors interact to influence pain in youth with obesity. This study aims to better understand how these factors predict each other through serial mediation analyses to uncover some of the complexities of pediatric obesity and consequent pain experiences. There are three primary hypotheses for this study. First, it is hypothesized that significant relationships will be identified between obesity (measured by BMI z-score) and self-reported youth pain, functional limitation, sleep quality, depressive symptoms, and health-related quality of life (HRQoL). Second, the relationship between pain perception and HRQoL will be mediated by functional limitation, sleep quality, and depressive symptoms and third, the relationship between pain burden and HRQoL will be mediated by functional limitation, sleep quality, and depressive symptoms.
Methods
Participants
Participants were youth aged 12–18 years evaluated in the weight management clinic at Connecticut Children's Medical Center (CT Children's) for an initial visit between September 2016 and December 2021 who were enrolled in an existing Institutional Review Board (IRB) approved obesity program prospective database at CT Children's. This prospective database houses data from patients' initial and follow-up clinic visits, and is regularly updated and maintained to include variables of interest. Research assistants within the Pediatric Obesity Center are responsible for the entering, cleaning, and updating participant data on a regular basis.
Exclusion criteria for this study were youth younger than 12 or older than 18 years of age, those who could not speak or read English, or self-report their symptoms on various measures. We also excluded individuals who skipped entire measures or had significant data gaps to remove insufficient data. We began with a dataset of 594 patients, which was reduced to 358 after removing those who were too young, old, or were not seen for an initial visit (and therefore had undergone treatment previously), and then to 98 after removing those with incomplete measures that could not be scored with accuracy. Series mean imputation was used for remaining missing item values (for the scales included in the analysis, the 98 respondents left 183 items blank of 10,093 total item responses, representing 1.8%).
The study was approved by CT Children's IRB. Patient data were stored in a secure database and extracted into a separate data collection sheet for the purposes of this study. All patients were assigned participant IDs and identifiers were removed, including name and medical record number. Data for this study were collected as standard of care for initial patient encounters in the Pediatric Obesity Center. Quantitative data on demographics, anthropometrics, and participant survey data for statistical analysis were also extracted.
Measures
Demographics and anthropometrics
The following information was extracted from participants' medical records: demographics including age, sex, race and ethnicity, and level of obesity as measured by BMI and BMI z-score.
The Pain Burden Inventory
The Pain Burden Inventory is a 7-item scale developed from the Sickle Cell Disease Pain Burden Interview 19 to measure the impact of chronic pain in pediatric populations. 20 Each item is answered with a 5-point Likert scale ranging from 0 (none) to 4 (every) to measure how often individuals experienced pain over the past month. Scores are summed for a total score and range from 0 to 28, with higher scores indicating greater pain burden. This scale has strong reliability (α = 0.793) and cross-informant agreement (r = 0.822, p = 0.000). 20
The Pain Frequency–Severity–Duration Scale
The Pain Frequency–Severity–Duration Scale (PFSD) is a 7-question scale that measures frequency, severity, and duration of pain in youth over the last 2 weeks. 24 This scale is intended for children and adolescents between 8 and 18 years of age rated on a 10-point Likert scale ranging from 0 (no pain) to 10 (worst pain). A composite score is calculated by multiplying reported days of pain, typical pain level, and worst pain level, and then dividing the total product by 10. This scale was preliminarily validated compared with other measures of pain. PFSD composite scores were significantly correlated to total scores on the Child Activity Limitations Questionnaire (r = 0.49, p < 0.01) and the Pediatric Quality of Life Inventory (r = −0.38, p < 0.01) This scale gives a well-rounded picture of a child or adolescent's pain, looking at not more than just severity, but also differences between typical and worse pain, how long these experiences last, and how often they occur.
The Child Activity Limitations Interview
The Child Activity Limitations Interview (CALI-21) is a 21-item scale that measures functional impairment of school-age children owing to chronic pain. 25 There are identical child self-report and parent report versions of the CALI-21. Each item lists an activity that participants give difficulty ratings to on a 5-point Likert scale ranging from 0 (not difficult) to 4 (extremely difficult), thinking about the past 4 weeks specifically. Scores are summed, ranging from 0 to 84, with higher scores indicating greater limitation or impairment. Psychometric testing indicates strong reliability for the entire measure (α = 0.95) along with overall construct validity. 25 Correlations between child and parent versions were strong for the total score (r = 0.73, p = 0.000). The child-report version of the CALI-21 was used for the purposes of this study.
The Adolescent Sleep–Wake Scale
The Adolescent Sleep–Wake Scale (ASWS) is a 28-item self-report scale for adolescents aged 12–18 years based on the Children's Sleep–Wake Scale.26,27 The ASWS assesses sleep quality over the past month through a 6-point frequency Likert scale ranging from 1 (never) to 6 (always). There are five subscales measuring sleep including going to bed, falling asleep, maintaining sleep, reinitiating sleep, and returning to wakefulness. Total score is an average of items with higher scores indicating greater sleep quality. Good internal consistency scores were found for the subscales (α = 0.64–0.82) and the full scale (α = 0.86) in a sample of American adolescents. 28 A recent revalidation of the ASWS found strong reliability for total scores (α = 0.88) and subscale scores (α = 0.75–0.82). 29 Only total scores were calculated for the purposes of this study.
The Center for Epidemiological Studies Depression Scale for Children
The Center for Epidemiological Studies Depression Scale for Children (CES-DC) is a 20-item self-report for depressive symptoms in children and adolescents. 30 Its use is designed for those between 6 and 17 years old. The CES-DC is intended as a screen for potential depressive symptoms and not as a diagnostic tool. Each item is rated with a 4-point frequency Likert scale, ranging from 0 (not at all) to 3 (a lot). Some items are reverse-scored, and scores are summed for a total score. Psychometric testing for the CES-DC suggests strong validity with high internal consistency (α = 0.89) 31 and concurrent validity with the Children's Depression Inventory. 30 In addition, 2-week test–retest reliability was found to be stronger in adolescents (ages 12–18 years) than in children (ages 6–11 years). 30 A separate study examining the scale on adolescents ages 12–16 years also found strong validity (α = 0.80). 32
Sizing Me Up
Sizing Me Up is a 22-item child self-report scale that measures HRQoL in children with obesity developed from the Sizing Them Up parent report version. 33 Measured on a 4-point frequency Likert scale, scores range from 1 (none of the time) to 4 (all of the time), with scores ranging from 22 to 88. Higher scores indicate greater HRQoL. Some items are reverse-scored and the scale itself is scored by summing the scores, subtracting them by 22, dividing by 66, and multiplying by 100 for a total score. Initial psychometric testing found strong overall reliabilty for the measure (α = 0.82). Test–retest reliability had a score of 0.78 for the entire measure.
Data Analyses
We first tested for correlations between primary study variables and then conducted serial mediation analyses. Spearman correlations and Mann–Whitney U-tests were used to examine relationships between the primary study variables. A two-sided p-value of <0.05 was considered statistically significant. The serial mediation models were tested using Hayes 34 PROCESS macro model 6. We investigated the indirect effect of youth pain and pain burden on HRQoL through functional limitation, sleep quality, and depressive symptoms among youth with obesity, along with the serial mediation of these three variables. Using the bias-corrected bootstrap method with 5000 resamples we calculated the 95% confidence interval (CI). If the CI does not include 0 then the indirect effect is significant.
Results
Participant Demographics and Anthropometrics
The sample of this study was diverse, with 62.2% being female, 63.3% not Hispanic or Latino, and 51% White (Table 1). Most of the data were not normally distributed, so continuous variables are reported as medians with interquartile ranges (IQRs), and categorical variables as n (%). Eight participants were classified as overweight (8.2%) and 90 as having obesity (91.8%). Of those with obesity, 62 had moderate obesity (95th percentile for BMI), and 28 had severe obesity (99th percentile for BMI). The median age of participants was 14.7 years, had median BMI levels of 36.5 kg/m2 (IQR = 33.8–40.8) and median BMI z-scores of 2.4 (IQR = 2.2–2.6).
Participant Demographics and Anthropometrics
n = 98. Participants were mostly female (n = 61, 62.2%) with a median age of 14.7 years old (IQR = 13.5–16.2), median BMI levels of 36.5 kg/m2 (IQR = 33.8–40.8), and median BMI z-scores of 2.4 (IQR = 2.2–2.6).
IQR, interquartile range.
Descriptive Statistics and Correlation Testing
In testing the first hypothesis, descriptive statistics and correlations were conducted between the primary study variables (Table 2). Spearman correlations were used for relationships between continuous variables, and Mann–Whitney U-tests were used for the relationship between dichotomous (i.e., sex) and continuous variables. Sex was positively related to depressive symptoms and negatively associated with HRQoL (i.e., female sex was associated with higher levels of depressive symptoms, but lower levels of HRQoL). Youth pain was positively correlated to pain burden and functional limitation, and negatively correlated to sleep quality and HRQoL. Pain burden was positively correlated to functional limitation and depressive symptoms, and negatively correlated to sleep quality and HRQoL. Functional limitation was negatively correlated with sleep quality and HRQoL, and positively correlated with depressive symptoms. Sleep quality was negatively correlated with depressive symptoms and positively correlated with HRQoL. Finally, depressive symptoms were negatively correlated with HRQoL.
Descriptive Statistics and Correlations for Study Variables
Sex was coded as 0 for males, 1 for females.
Obesity level as determined by BMI z-score.
p < 0.05, **p < 0.01.
HRQoL, health-related quality of life.
Serial Mediation Analyses
As some of the data in this study were not normally distributed, we cannot assume normality of error terms within our mediation models. However, the bias-corrected bootstrapping method used in these analyses adjusts for asymptotic data and uses CI estimates to test for statistical significance of indirect effects. 35 In both serial mediation analyses, depressive symptoms negatively predicted HRQoL (β = −0.43, p < 0.001; β = −0.43, p < 0.001), respectively. The results indicate that only the total effect (β = −0.33, p < 0.05) of youth pain on HRQoL was significant. The direct effect (β = −0.18, p > 0.05) was no longer significant indicating full mediation. One significant indirect relationship of seven paths was significant (Fig. 1). If the bootstrapping CI includes 0 the indirect effect is not significant. 35 The indirect effect of pain on HRQoL through functional limitation, sleep quality, and depressive symptoms, respectively [β = −0.01, standard error (SE) = 0.01, 95% CI = (−0.04 to −0.001)] was significant, indicating serial mediation supporting hypothesis 2 (Table 3). Youth pain positively predicted functional limitation, which negatively predicted sleep quality, and in turn negatively predicted depressive symptoms, which ultimately negatively predicted HRQoL.
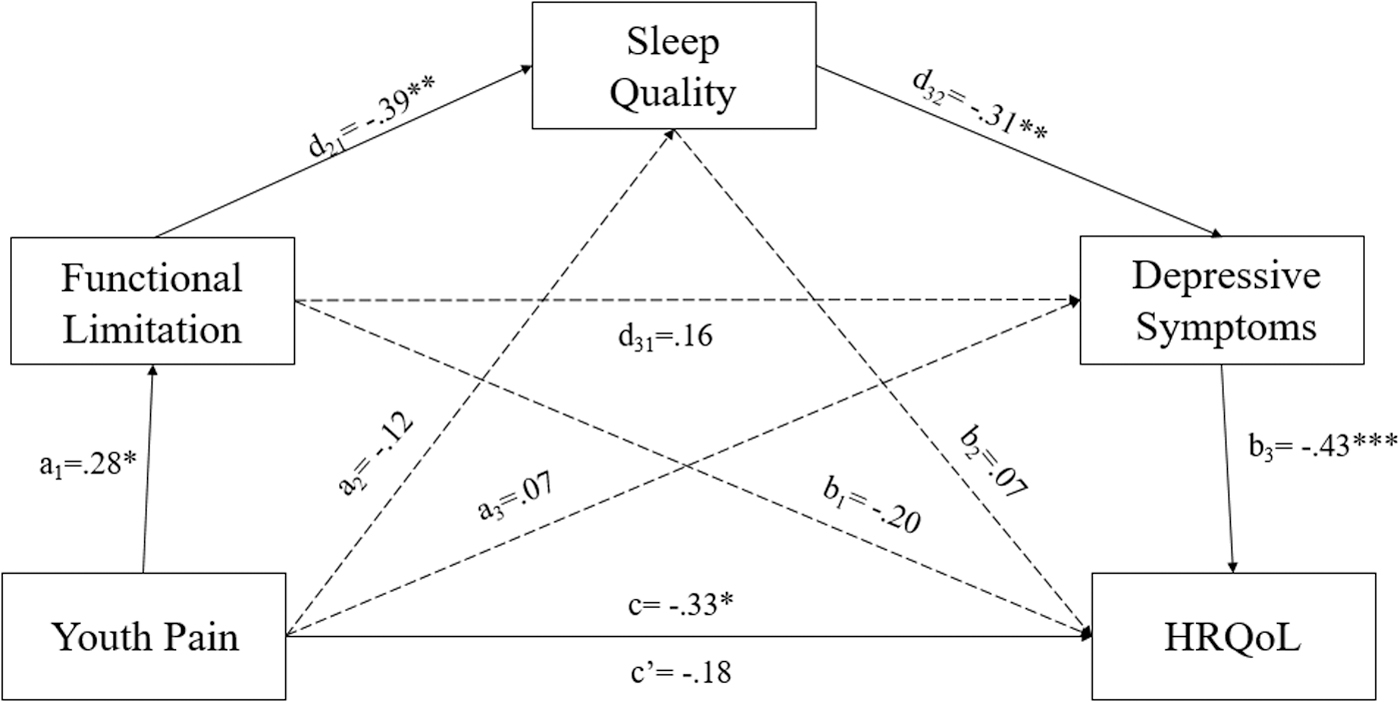
Indirect Effect of Youth Pain on Health-Related Quality of Life via Functional Limitation, Sleep Quality, and Depressive Symptoms (n = 82)
Standardized coefficients are presented.
CI does not include zero.
CI, bootstrapping confidence interval; DepSym, depressive symptoms; FuncLim, functional limitation; LL, lower limit CI; SE, standard error; SleepQual, sleep quality; UL, upper limit CI.
For the second mediation analysis, results indicate that the total effect (β = −0.31, p < 0.01) of pain burden on HRQoL was significant, and the direct effect (β = −0.12, p > 0.05) was not significant, thus indicating full mediation. Two significant indirect relationships of seven paths were significant (Fig. 2). The indirect effect of pain burden on HRQoL through sleep quality and depressive symptoms, respectively [β = −0.05, SE = 0.03, 95% CI = (−0.11 to −0.01)] was significant, indicating serial mediation. The indirect effect of pain burden on HRQoL through functional limitation, sleep quality, and depressive symptoms, [β = −0.01, SE = 0.01, 95% CI = (−0.04 to −0.002)] was significant, indicating serial mediation supporting hypothesis 3 (Table 4). Pain burden positively predicted functional limitation, which negatively predicted sleep quality, and in turn negatively predicted depressive symptoms, which ultimately negatively predicted HRQoL.
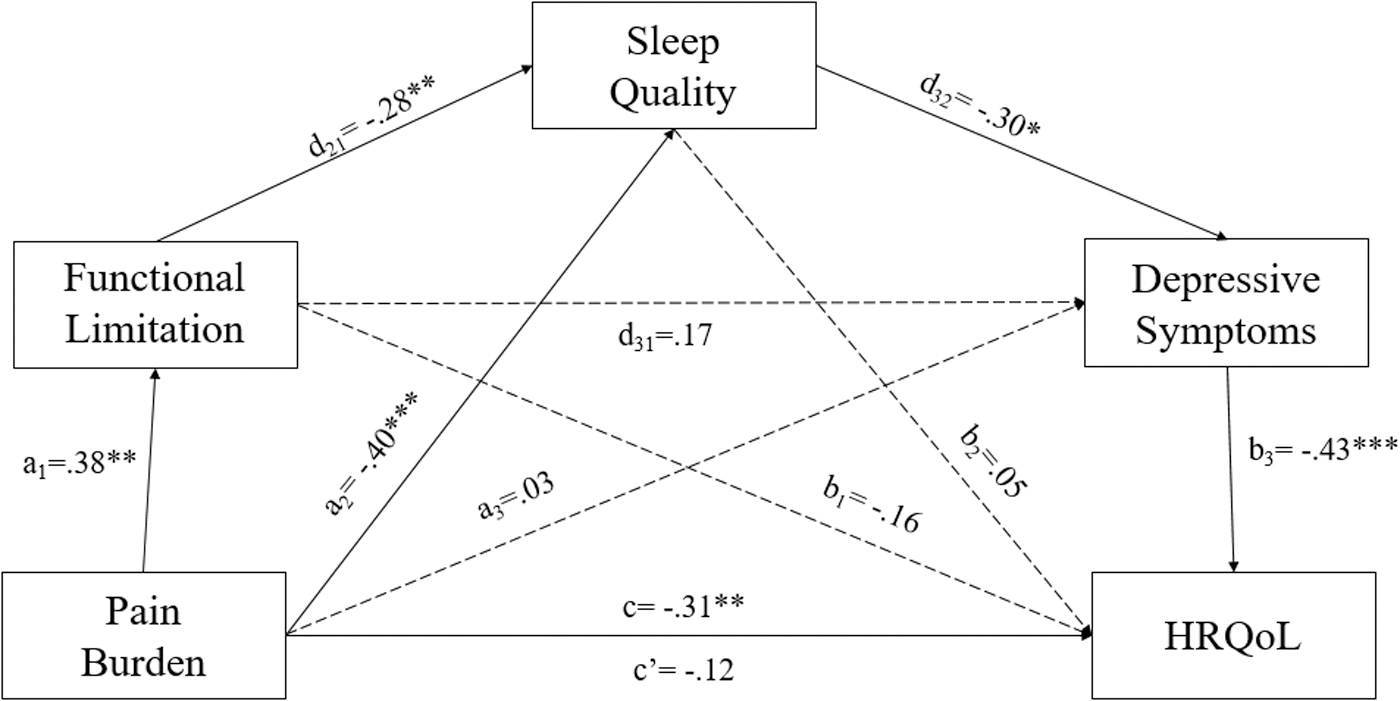
Indirect Effect of Pain Burden on Health-Related Quality-of-Life via Functional Limitation, Sleep Quality, and Depressive Symptoms (n = 98)
Standardized coefficients are presented.
CI does not include zero.
Discussion
This study aimed to better understand the relationship between obesity, pain, and HRQoL through a biopsychosocial approach. We assessed the indirect mediating effects of functional limitation, sleep quality, and depressive symptoms in the relationship between youth pain and HRQoL. This study demonstrated findings consistent with previous research showing significant relationships between youth obesity, pain levels, functional limitation, sleep quality, depressive symptoms, and HRQoL.6,16,21
Supporting our main hypotheses we found full serial mediation in the relationship between youth pain and HRQoL through functional limitation, sleep quality, and depressive symptoms, despite no other significant paths. There was a significant negative total effect between youth pain and HRQoL; however, the direct effect was not significant indicating full mediation.
Results show full serial mediation in the relationship between pain burden and HRQoL through functional limitation, sleep quality, and depressive symptoms. There was a significant negative total effect between pain burden and HRQoL; however, the direct effect was not significant indicating full mediation.
These findings are in line with past research that identified significant relationships between youth pain measures, functional limitation, sleep quality, symptoms of depression, and HRQoL,6,16,21 but is the first research to establish a significant predictive model between these variables. Youth pain and pain burden scores were significantly positively related to self-reported functional limitation, such that as pain increased, so did functional limitation, consistent with other studies. 16 Functional limitation then significantly negatively predicted sleep quality, such that as functional limitation reports increased, overall sleep quality decreased, as supported by past research. 36 Sleep quality ratings then significantly negatively predicted symptoms of depression, such that as sleep quality worsened, self-reported depressive symptoms increased, which is supported by prior studies. 21 Finally, symptoms of depression significantly negatively predicted HRQoL, such that as these symptoms increased, self-reported HRQoL decreased, which has been strongly supported in past research. 37
It was surprising to find no significant relationships between obesity levels and youth pain scores (hypothesis 1). This could be attributed to the fact that our sample only contained youth that have overweight or obesity and are in the 95th percentile for BMI (median z-score = 2.4, IQR = 2.2–2.6). Having a sample with more variation in BMI z-scores could potentially yield results consistent with our original hypothesis.
Limitations
First, our original dataset of 594 participants was reduced to 98 after adjusting for exclusion criteria and removing those with incomplete surveys. This small sample size reduces overall statistical power, effect size, and generalizability to this population. Although we do not think there are any significant differences between those who completed their measures and those who did not, we also cannot discount that kids with more depression or more pain who were not able to complete their measures. In addition, the sample consisted of only patients who were seen in the weight management clinic at Connecticut Children's Medical Center for an initial visit and does not include any underweight or healthy weight youth. Furthermore, analyses for this study utilized a correlational design, and causation cannot be determined between any statistically significant relationships that were found. Mediation analyses as well make assumptions about the ordering of the relationships between study variables can truly only imply causation when tested in longitudinal studies.
Contributions
This study uniquely contributes to existing research through the discovery of the serial mediating effects of functional limitation, sleep quality, and depressive symptoms in the relationship between youth pain ratings and HRQoL. These variables have been studied independently as influential in the relationship between obesity-related pain and HRQoL, but not together in a serial mediation model. In addition, findings in this study support past research that have found significant relationships between pain and functional limitation, sleep quality, depressive symptoms, and HRQoL.6,38,39 Finally, this study had a more diverse sample (30.6% Hispanic, 22.4% Black) than other research looking at similar processes.16,18,20,36
Footnotes
Impact Statement
The present study identified an important link in the relationship between youth pain associated with obesity and health-related quality of life. Variables of functional limitation, sleep quality, and depressive symptoms were significantly associated with obesity-related pain reports, and significantly mediated the relationship between pain and health-related quality of life in youth with obesity.
Acknowledgments
The authors acknowledge and give their greatest thanks to their advisor Joanne DiPlacido who made this work possible. Her knowledge and enthusiasm on this topic in class inspired us to investigate the subject even further as a Masters thesis, and now as a publishable work with her guidance. The authors also thank Melissa Santos and William Zempsky for their invaluable expertise on these topics and mentorship on this project, without which this research would not be possible.
Authors' Contributions
C.B.T.: conceptualization (lead); formal analysis (supporting); investigation (lead); methodology (lead); visualization (lead); writing—original draft (lead). J.D.: conceptualization (supporting); formal analysis (lead); methodology (supporting); supervision (lead); writing—review and editing (equal). W.T.Z.: supervision (supporting); writing—review and editing (equal). M.S.: conceptualization (supporting); resources (lead); supervision (supporting); writing—review and editing (equal).
Funding Information
No funding was received for this article.
Author Disclosure Statement
W.T.Z. is a consultant for GSK and Glycomimetics, and a member of the Data and Safety Monitoring Board for Lundbeck. There are no other conflicts of interests to disclose.