
Abstract
This study was performed to explore the association between attention-deficit/hyperactivity disorder (ADHD) and the risk of overweight/obesity in both children and adolescents. The PubMed, Web of Science, and Cochrane Library databases were searched for relevant studies published before July 12, 2022. Studies with data for calculating the odds ratio (OR) of childhood overweight/obesity and ADHD were included. The literature value was assessed by the cross-sectional evaluation criteria proposed by the Agency for Healthcare Research and Quality (AHRQ). All analyses were conducted using StataSE 11 and RevMan 5.3 software with random-effects models. This review included a total of 16 studies covering 14,981 cases and 128,916 controls.According to the meta-analysis, children with ADHD had a significant risk for co-occurring overweight and obesity [OR 1.56; 95% confidence intervals (CI) 1.32–1.85], especially boys (OR 1.45; 95% CI 1.10–1.90), people in Asia (OR 3.25; 95% CI 1.70–6.21) and Europe (OR 1.85; 95% CI 1.61–2.12), and patients not using medication (OR 1.54; 95% CI 1.22–1.94).ADHD has a significant association with overweight and obesity in both children and adolescents, which may be altered by factors such as geography, gender, and medication use. Timely treatment should be provided to children and adolescents diagnosed with ADHD to inhibit the emergence of overweight and obesity.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a general neurodevelopment disorder among children and adolescents that results in a maintained pattern of inattention and/or hyperactivity and impulsivity with less appropriation or more disruptiveness compared with children of the same age, leading to functional dysfunction in many settings, and is present for at least 6 months. 1 The incidence of ADHD in children is ∼7% worldwide and continues to increase each year, 2 with an estimated incidence of 3% annually between 1997 and 2006. Studies have demonstrated the development of this disease during childhood in up to 65% of adults with ADHD 3 ; as a result, childhood is a critical stage to screen and diagnose ADHD. The most commonly utilized diagnostic guideline for ADHD is the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). 4 In the current clinical guidelines, a treatment approach allowing multimodal individualization is recommended, including psychoeducation, pharmacological interventions, and nonpharmacological interventions.
Stimulants (methylphenidate, amphetamines) and nonstimulants (atomoxetine, guanfacine, clonidine) are the main medications used for treatment. 5 ADHD, as a highly prevalent mental health disorder, can lead to an increased risk of longer term adverse outcomes in children, such as a reduction in educational and employment attainment, 6 which is also correlated with destroyed long-term self-esteem and social function reactions compared with individuals without ADHD. 7
Overweight and obesity are the primary risk factors for various diseases and are treated as global public health concerns because the worldwide prevalence is increasing at a substantial rate. Approximately 2 billion people have been reported to be overweight, one-third of whom are diagnosed with obesity. 8 Although the rates vary among countries, the prevalence has been maintained over the past 40 years, doubling in more than 70 countries since 1980 and even tripling in several developing countries. 9 Because children are experiencing a critical stage of growth and development, the identification of overweight and obesity in children cannot be performed in the same way as in adults.
At present, there are several different international diagnostic criteria for children. According to the Centers for Disease Control and Prevention (CDC) diagnostic criteria, overweight is defined as a BMI in the 85th–95th percentile, and obesity is defined as a BMI greater than or equal to the 95th percentile; the World Health Organization (WHO) criteria are the 85th–97th percentile for overweight and greater than or equal to the 97th percentile for obesity; and the International Obesity Task Force (IOTF) criteria are the 91st percentile for overweight and the 99th percentile for obesity. Obesity in children can have adverse impacts on almost all the systemic organs that lead to serious outcomes, such as hypertension, dyslipidemia, insulin resistance, dysglycemia, fatty liver, and psychosocial complications. It also contributes to increased health care expenditures. 10
As more research has been performed, the correlation between overweight/obesity and ADHD has attracted increasing attention. Several hypotheses and possible mechanisms exist according to current research. The relationship between ADHD and overweight/obesity may be due to the causative environment, genes, or interactions between the two; abnormal eating patterns and executive dysfunction in patients with ADHD; low physical activity; sleep disturbances; and hypotheses of inflammation. 11 A study by Chen et al. 12 found familial coaggregation of ADHD and clinical obesity, and the strength of the coaggregation decreased with decreasing genetic relationship. Other causes may be the common biological mechanisms shared by ADHD and obesity, that is, altered reinforcement mechanisms, brain-derived neurotropic disorder, and melanocortin-4-receptor deficiency. 13
A study demonstrated that the causal effects of cogenetic or familial backgrounds and/or potential on overweight and obesity are established in early childhood in children with ADHD and recommended intervention and prevention programs in the early stage. 14 The impulsivity and attention deficits caused by ADHD may lead to abnormal eating behavior patterns, thus inducing abnormal weight gain. 15 Studies have found that adults with ADHD have a higher frequency of unhealthy food choices than healthy people. 16 More than 50% of children with ADHD display abnormal eating behaviors, such as emotional eating, picky eating, and prolonged mealtimes. 17
Clinical symptoms in children with ADHD have been found to be influenced by abnormal eating behaviors to some extent. 18 The damaged circadian rhythm in ADHD patients elevates the risk of erratic eating patterns and ultimately obesity development. 19 Alertness and feeding behaviors in ADHD may be influenced by an imbalance in the hypocretin/orexin system, 20 which needs to be confirmed by more studies.
The objective of this work is to explore the correlation of childhood ADHD with overweight and obesity, as well as the possible impact factors between them, and to provide perspectives for intensive intervention for adolescents with ADHD with the ultimate goal of altering the trajectory of both disorders. Previous articles have indicated a high prevalence of overweight and obesity in two ADHD groups, 21 while no comparisons with healthy control populations have been carried out. This article explored the odds ratio (OR) for co-occurring overweight and obesity using studies with control populations compared with healthy populations.
A relevant study reporting OR with 95% confidence intervals (95% CI) was published in 2016, 22 and ADHD was found to be associated with obesity, a relationship that was evident in childhood and adolescence. ADHD is also significantly associated with being overweight. Meta-regression results showed no significant effect on the relationship between obesity and ADHD by sex, study setting, study country, and study quality. Data in recent years have provided new insights into the correlation of overweight with ADHD. Inspired by but distinguished from that study, this article focuses on adolescents younger than the age of 18 who are overweight/obese and further explored the geographical and gender factors that may influence the correlation between ADHD and overweight/obesity.
Methods
The research was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and criteria, and the protocol was registered with PROSPERO (CRD42022364727).
Literature Search
The PubMed, Web of Science, and Cochrane databases were searched using MeSH subject terms and keywords related to the subject for relevant studies published before July 12, 2022; the language of the studies was limited to English, and the search was not limited by geography. Studies were included in the analysis if they met the requirements listed below. Document retrieval and the selection of retrieval results were performed independently by two authors according to the qualified document collection standard. An example search strategy for the PubMed database is presented in the Supplementary Materials.
Study Collection
Studies that met the following criteria were included.
Type
Studies reporting the extent of the association between overweight/obesity and ADHD expressed as OR with 95% CI or the data for OR calculation were included. Population-based studies and clinical reports with ADHD patients and contemporaneous non-ADHD patients as controls were included. For longitudinal studies, data were extracted according to baseline or the earliest time point.
Participants
Individuals with ADHD are those who (1) met the DSM definition or ICD definition for ADHD, (2) had an ADHD diagnosis according to the medical record, (3) scored above the symptom sill on a validated ADHD rating scale, and (4) answered “yes” to the question “Did your doctor ever diagnose you with ADHD?” Considering that no global consensus has been reached on the definition of obesity and overweight, all definitions based on the recognized BMI cutoff were incorporated, including the CDC, the IOTF, and the WHO. Studies including individuals of both genders aged from 0 to 18 and including people without ADHD as controls were retained.
Data Extraction and Evaluation of Study Quality
The data were extracted independently by two authors and included the name of author, publication year, age (range), regions, gender, number of cases, number of controls, and medication use. Disagreements arising in the process of data extraction were decided by consultation between the two authors. The value of each study was determined by the cross-sectional study evaluation criteria of the Agency for Healthcare Research and Quality (AHRQ) with 11 items, each of which had answer choices of “yes,” “no,” and “unclear.” If the answer was “yes,” the item was scored 1. If a study scored 0–3, it was considered low quality; if a study scored 4–7, it was considered moderate quality; and if a study scored 8–11, it was considered high quality.
Statistical Analyses
All analyses were conducted using StataSE 11 (StataCorp LP, College Station, TX) and RevMan 5.3 software. The primary outcome of the meta-analysis was a pooled estimate of the risk of co-occurring overweight and obesity in children and adolescents with ADHD reported as ORs with 95% CI. The statistical heterogeneity across the included studies was evaluated using the I2 statistic with a random-effect model. Publication bias was assessed by quantitative Egger's and Begg's tests. Subgroup analyses were also completed according to sex (male, female), medication use (medicated, unmedicated), geographic region (the Americas, Europe, Asia), and degree of overweight (overweight, obesity).
Results
Characteristics and Quality of the Included Studies
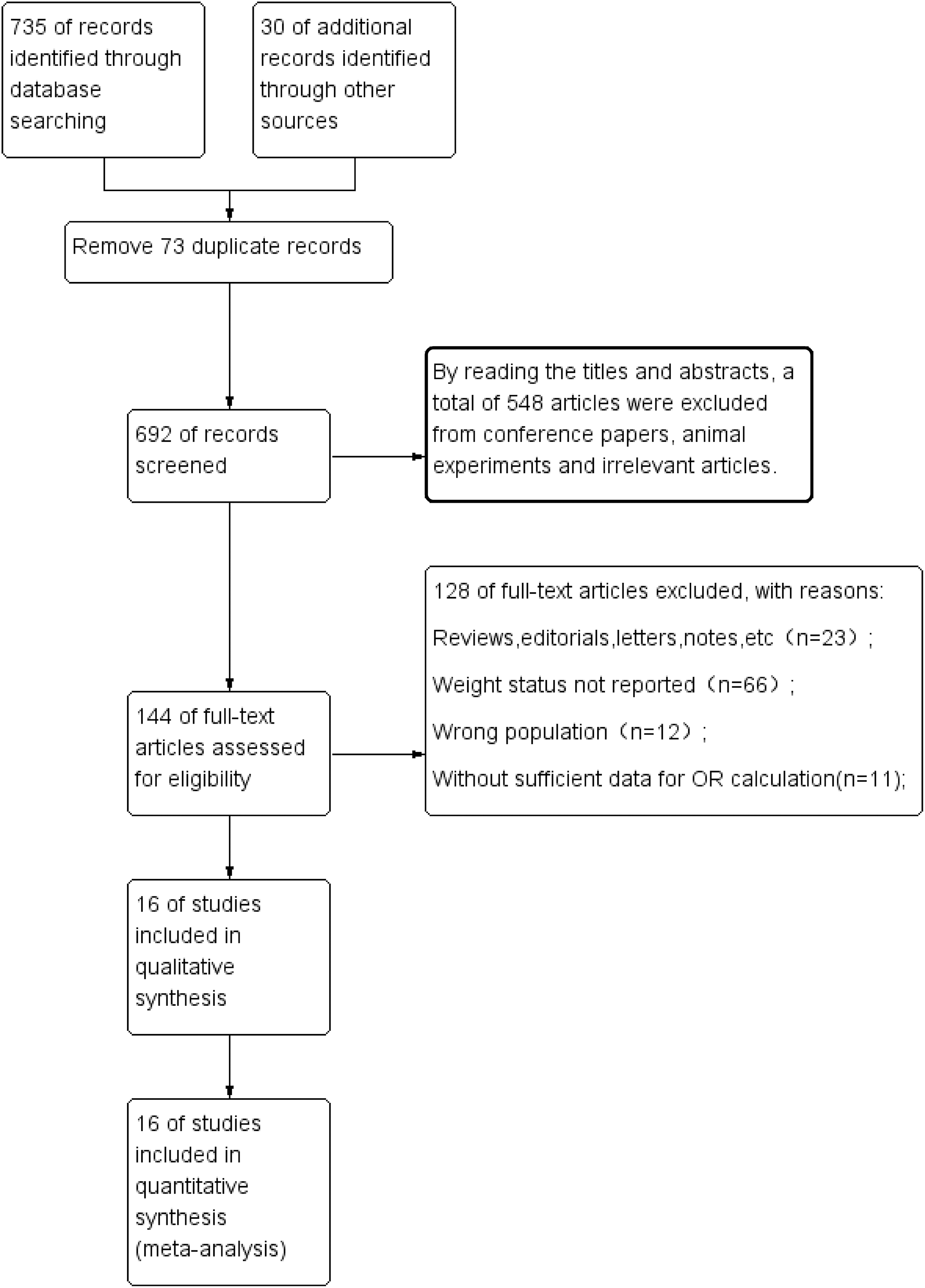
As shown in Figure 1, 735 related studies were initially identified through database searching, and 30 were identified through other sources. After removing duplicates, 692 records remained. We examined 144 full-text articles, and 16 studies with 14,981 cases and 128,916 controls were eventually included in this study.23–38
The information of the included studies is illustrated in Table 1; name of the author, publication year, study populations, regions, age (range), gender, number of cases, number of controls, and medication use were collected for analyses. The publication year of studies ranged from 2011 to 2022. Five of the studies were conducted in the Americas, five in Asia, and four in Europe. In terms of medication use, four articles reported medication use, and six articles reported no medication use. Eight studies reported on the co-occurring risk of overweight and obesity in boys with ADHD, and seven reported on girls. Nine studies measured the comorbidity of overweight in the ADHD population, and 12 studies measured the comorbidity of obesity in the ADHD population. The results of the literature quality evaluation indicated 5 high-quality articles and 11 moderate-quality articles.
Characteristics of Included Studies
ADHD, attention-deficit/hyperactivity disorder.
The Risk of Overweight/Obesity in Children With ADHD
The results of the meta-analysis indicated a significantly increased risk of developing overweight/obesity in children with ADHD (OR 1.56; 95% CI 1.32–1.85), as indicated in Figure 2. The outcome of the heterogeneity analysis was I2 = 88% (p < 0.01), and so, a random-effects model was selected. No significant publication bias was revealed according to Begg's test (p = 0.065) and Egger's test (p = 0.065).

Subgroup Analyses
Subgroup analyses by region, medication use, and degree of overweight were carried out. As illustrated in Table 2, in the gender subgroup analysis, boys with ADHD exhibited a significant risk of co-occurrence of overweight and obesity (OR 1.45; 95% CI 1.10–1.90) and girls did not (OR 1.33; 95% CI 0.88–2.00). For the medication subgroup analysis, the meta-analysis of ORs for overweight and obesity revealed a statistically significant result in the population without any medication (OR 1.54; 95% CI 1.22–1.94). However, the concurrent risk of being overweight and obese was not significant in the treated population with ADHD (OR 1.23; 95% CI 0.81–1.88). In terms of the degree of overweight outcomes, significant concurrent risks were revealed in both overweight and obesity.
The Results of Subgroup Analyses
CI, confidence intervals; OR, odds ratio.
Finally, the subgroup analysis based on the geographic location of the study population demonstrated a significant risk of co-occurring overweight and obesity in people with ADHD in both Europe and Asia, but not in the Americas (OR 1.06; 95% CI 0.91–1.23) (Supplementary Figs. S1–S5).
Discussion
The findings of this article indicate that ADHD has a significant association with overweight and obesity in both children and adolescents, which may be altered by factors such as geography, gender, and medication use. Consistent with the results found in this article, an umbrella review from 43 studies with 1,390,311 individuals 39 focused on associations between mental and physical conditions in children and adolescents reported highly suggestive evidence for the association between ADHD and obesity (OR 1.32; 95% CI 1.18–1.47) based on a large number of studies.
The role of geographic factors in overweight and obesity development in ADHD patients is complex, with too many confounding factors involved, such as genetics, race, and income level. As a result, more in-depth studies are needed. Some studies40,41 have indicated that residence may alter the risk of overweight, identifying dietary patterns, genetics, and race as potential impacting factors. The results of Choudhry et al. 42 exhibited an association between childhood obesity in ADHD and some socioeconomic factors, specifically that low-income families are associated with an elevated risk of ADHD.
One study found that the coverage of ADHD prevalence data for children aged 5–17 years in low- and middle-income countries in Europe and Asia was much lower than that in high-income countries in North America and Latin America. 43 This also suggests that research on ADHD and its comorbidities in low- and middle-income countries with high proportions of children and adolescents needs to be further enhanced. This may also account for regional differences. The treatment rates for ADHD and overweight are also lower in low- and middle-income countries than in high-income countries due to the level of socioeconomic development and medical care.
Furthermore, one study 44 found that minority children were less likely to be diagnosed with ADHD and its comorbidities and less likely to receive prescribed stimulant medication and adhere to it than nonminority children. These differences reflect the attitudes toward and the cultural diversity in the treatment of ADHD and its comorbidities of overweight and obesity (e.g., fear of social stigma), as well as the limited access to timely treatment for these populations. In addition, in those with ADHD, the prevalence of overweight and obesity may vary according to the choice of overweight diagnostic criteria, 45 which may also be one source of the difference.
Regarding the medication-using population, we derived the same conclusion as Cortese et al., 22 who found a significant risk of co-occurring overweight and obesity in a medication-naive population. The study by Tsujii et al. 46 found that patients taking amphetamine and its derivatives, methylphenidate and its derivatives, and atomoxetine showed decreased weight compared with patients taking a placebo. A common side effect of methylphenidate, which is a commonly utilized stimulant drug, is appetite suppression, leading to reduced weight gain and decreased appetite in patients, which ultimately affects BMI and body size. 47 Another alternative reason is a potential link between high BMI and several executive functioning deficits prevalent in patients with ADHD, 48 which could be alleviated by pharmacological interventions and thus reduce the development of overweight and obesity.
Studies have shown that ADHD and executive function deficits are a barrier to weight loss in obese patients, and if ADHD and executive function deficits are improved through timely treatment, then obesity in children with these two diseases can be effectively reduced or prevented. 49 ADHD treatment may significantly improve the effectiveness of weight management strategies. 50 However, Hanc et al. 51 indicated that the regulation of cool executive function may not be the cause of defects in overweight boys with ADHD, but may result from single nucleotide polymorphisms (SNPs) in three candidate genes, namely, DRD4 rs1800955, SNAP25 rs363039 and rs363043, and 5HTR2A rs17288723. Therefore, more comprehensive work is required to confirm the relationship of executive functioning with weight and BMI in ADHD patients.
Gender plays an essential role in exploring the association in the present study, and ADHD prevalence differs in boys and girls. The research conducted by Bauermeister et al. 52 revealed a 2.3 times higher occurrence of ADHD in boys than in girls. It has been suggested that more prominent behavioral/emotional problems may be required for girls with ADHD to meet the full diagnostic criteria, and gender differences often exist in parental perceptions of ADHD behavior and impairment. 53 This may explain why this correlation was more prominent in boys, and more studies including girls are required to confirm and explore the difference.
Fliers et al. 54 demonstrated ADHD as a risk factor for obesity in boys aged 5–17 years and girls aged 10–12 years; however, no association in girls aged 5–9 years and 13–17 years was observed. They speculated that the reason for difference was that girls aged 5–9 tended to accept parental discipline, while girls aged 13–17 showed more prominent body awareness relative to boys and younger children. In contrast, Aguirre et al. 55 proposed that girls with ADHD tend to develop overweight or obesity. Possible reasons for this difference may be that the inattentive subtype is more prevalent in female patients and the hyperactive-impulsive subtype is more prevalent in male patients. Girls with ADHD show decreased self-efficacy, poorer coping strategies, and increased rates of depression, anxiety, and eating disorders, which may result in excessive weight gain. Boys with hyperactive-impulsive ADHD exhibit increased resting energy expenditure, which may exert a protective effect on weight gain. Sleep dysfunction, loss of control/binge eating disorder, and anxiety are common complications of ADHD and obesity, 56 which cannot be ignored when investigating the association between ADHD and obesity.
Children and adolescents aged 18 and younger are covered in this article, which suggests the emergence of an association between ADHD and overweight/obesity in childhood and adolescence that deserves sufficient attention. Prompt medical attention should be given to patients with ADHD, with a focus on weight health and sleep dysfunction, loss of control/binge eating disorder (LOC-ED/BED), and anxiety along with ADHD treatment. However, there are some limitations to this study. Most of the data in this article were obtained from studies with cross-sectional designs, and the capability to verify the causal relationship between overweight and ADHD was not strong enough. Moreover, some of the original data in the literature were not specific, such as the age group. Further studies are still required to validate the above situation.
Conclusions
In summary, our meta-analysis indicated that ADHD may relate to overweight/obesity in both children and adolescents. The association may be altered by factors such as geography, gender, and medication use. Timely treatment should be paid attention to for children and adolescents with ADHD. However, given the limitations of this study, further studies are still required to validate this finding.
Impact Statement
We found that children with ADHD have a higher risk of being overweight and obese than people with healthy weight, especially boys, children in Europe and Asia, and untreated people. We recommend timely intervention in children with ADHD to prevent the occurrence of overweight and obesity.
Footnotes
Acknowledgments
We sincerely thank all the support from all the authors.
Authors' Contributions
Y.Z. and S.W. conceived and designed the study. Y.Z. and N.-N.W. completed literature search and data extraction. D.P. checked data extractions. Y.Z. and N.-N.W. carried out the statistical analysis and drafted the article. D.P. and S. W. provided critical review and substantially revised the article. All authors read and approved the final article.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.