
Abstract
Rates of class III, or greater, obesity have risen among adolescents in the United States. Metabolic and bariatric surgery (MBS) is a safe and effective treatment option for severe obesity among teenagers that results in improvements in cardiometabolic and psychosocial health. Despite its effectiveness, MBS remains largely underutilized and misconceptions exist among providers, parents/guardians, and adolescents. In addition, adolescents who have undergone MBS procedures report there are some topics they wish they had known more about before surgery and express concern that their unique needs are not understood. One potential solution to address these concerns includes preoperative educational materials tailored for adolescents. Currently, there are no standardized recommendations for preoperative educational materials. This editorial suggests the use of community-engaged research, and qualitative methodology, to consult with the primary stakeholder groups of preoperative adolescents, postoperative adolescents, parents/guardians, and clinicians to develop tailored materials that address the unique needs of adolescents undergoing surgical treatment for obesity.
Introduction
As of 2016, the prevalence of class III, or greater, obesity among adolescents has risen from 1.4% to 2.2% in ages 12–15 and 1.9% to 4.5% in ages 16–19. 1 However, given the impacts of the COVID-19 pandemic on food insecurity, behaviors related to diet and physical activity, and weight gain, it is likely that the prevalence of severe obesity is now higher among teenagers and the demand for evidence-based treatments is likely to increase. 2 Metabolic and bariatric surgery (MBS) is a safe and effective treatment option for adolescents with severe cases of obesity that results in cardiometabolic and psychosocial health improvements.
Among adolescents who undergo MBS, improvements in prediabetes, diabetes, abnormal kidney function, elevated blood pressure, and dyslipidemia are observed. 3 There are also improvements in weight-related and health-related quality of life.3,4 Despite its effectiveness, utilization of MBS as a treatment option is limited, and most individuals who undergo the procedures are White females with private insurance. 5 In addition to a lack of access to care, utilization of MBS may be further limited by parental and physician perspectives. In a sample of pediatricians and family physicians, 48% indicated they would never refer an adolescent for MBS. 6
Furthermore, very few adolescents receive counseling on surgical options and limited evidence examining the perspectives of MBS among parents/guardians indicates that the majority believe the minimum age to consider MBS is 18. 7 However, recent clinical guidelines from the American Academy of Pediatrics suggest considering adolescents aged 13 years and older with severe cases of obesity for MBS. 8 Therefore, due to the robust evidence of the effectiveness of MBS in improving cardiometabolic health outcomes, understanding perspectives of the patient, parent/guardian, and provider on MBS is crucial to improving the experience of pediatric MBS patients and promoting uptake of the procedure.
Although MBS is effective, qualitative data from adolescents who have undergone MBS procedures reveal there is concern about whether their unique needs are understood when they visit adult-oriented MBS centers. 9 In addition, although there is robust evidence of cardiometabolic improvements after MBS, evidence of psychosocial improvements is less pronounced and varies by gender, preoperative psychopathology, weight dissatisfaction, and weight change.4,10–15 Adolescents also experience a logical inconsistency before and after MBS.
Preoperatively, many adolescents believe surgery will “solve” their obesity and they will feel “normal,” but postoperatively they recognize MBS as a tool in managing their weight, not a cure for obesity.16–18 Thus, postoperative realities may not meet adolescents' prior expectations, a concept known as disillusionment, which could lead to reductions in psychosocial improvements.9,18–20 Considering adolescents' differential experiences, and that psychosocial factors are related to long-term weight maintenance, addressing this potential disillusionment among adolescent MBS patients is important to promoting sustained physical and mental health improvements.
One potential opportunity for addressing the issues of physician hesitancy, concerns from parents/guardians, and disillusionment (or misunderstandings of the complexities of obesity) from adolescents includes developing tailored preoperative educational materials. These materials may improve knowledge, adherence, and utilization of MBS by ensuring all relevant stakeholders feel comfortable during the treatment process. There is a unique opportunity to enrich educational materials by speaking with patients and parents/guardians, and consulting with providers. This editorial discusses what is missing from existing guidelines and presents actionable steps to addressing gaps through adolescent-specific tailored educational materials.
Existing Guidelines
Presently, requirements for MBS do not include standardized recommendations for preoperative educational materials. Current guidelines are based on the Teen Longitudinal Assessment of Bariatric Surgery (Teen-LABS) study, a longitudinal study of adolescent MBS patients that has recruited >200 patients from five centers across the United States. 21 Most centers included in the study provide printed materials, and two out of five centers offer adolescent specific weight-loss information and educational sessions, as opposed to having adolescents attend sessions with adults. 21 Additional guidelines recommend mandatory laboratory tests, including assessment of cardiac health and radiological diagnostics in addition to assessment of psychosocial readiness, which is subjectively determined through appointments with a mental health professional. 21
Beyond preoperative materials and guidelines, postoperative guidelines are also limited. Discussion of contraception, assessment of nutrition and psychological health in a multidisciplinary manner, and consideration of the transition from pediatric to adult care are suggested after surgery. 21 The most frequent postoperative requirement includes addressing nutritional deficiencies. 22
What Is Missing
There are limited data examining adolescents' perspectives on the MBS process, and existing qualitative evidence suggests there are topics missing from preoperative educational guidelines that adolescents prioritize. Ultimately, most teens report feeling prepared by their programs. In fact, in a study examining satisfaction with preoperative topics covered in clinic, 86.7% of patients would not change anything about the program. 23 Notably, this study quantitatively assessed preoperative topics by asking patients to identify which items in a list generated by a multidisciplinary team of health care professionals were adequately addressed. 23
However, when asked in an open-ended qualitative format, postoperative adolescents report they felt mostly prepared by their programs, but identify that they wish they knew more about some components of the postoperative experience such as pain management, weight-loss expectations, cosmetic changes (e.g., loose skin), and navigating reactions from family and peers.9,18 Moreover, there are barriers unique to teenagers that may impact adherence to postoperative requirements, which are not discussed in preoperative education. These barriers include navigating restrictions at school and work (e.g., time constraints), and interpersonal communication with family and friends. 9
Additional gaps exist. These include objective assessment of adolescents' understanding and psychosocial readiness and lack of information on current materials. Although there is a required psychological assessment before surgery, there is no standardized assessment of patient readiness. Thus, clinical decision-making may be subject to weight bias and discrimination. 24 Furthermore, although most centers offer printed materials, there is limited information available on their content and specificity; therefore, it is difficult to assess their quality and relevance for adolescents.
Utilizing Community-Engaged Research
The Active Community Engagement Continuum consists of three levels of engagement (consultative, cooperative, and collaborative) across five characteristics of engagement. 25 This framework is applicable to working with adolescents undergoing MBS as it includes community members in decision-making, a critical component of ensuring the relevancy of educational materials. A community-engaged approach is necessary to include a wide variety of perspectives (Table 1). It should be noted that currently most adolescents undergoing the procedure are White females with private health care insurance (Table 2). 5 However, as access to treatment improves, more diverse educational materials will be required. Developing tailored educational materials through a community-engaged approach will require a diverse community of adolescents, including teenagers who are diverse in age or developmental stage, race and ethnicity, family setting, and geography.
Insight Provided by Each Relevant Stakeholder Group
MBS, metabolic and bariatric surgery.
Developing tailored educational materials requires multiple steps, including discussions with adolescents and parents/guardians, development of the materials, consulting with physicians to ensure materials are comprehensive, assessing the acceptability and feasibility of implementation, and determining the effect of the educational materials on relevant outcomes. For the first step, it is important to consult three relevant groups: preoperative patients, postoperative patients, and parents/guardians.
There is a paucity of research examining the perspectives of preoperative adolescents. Patients undergoing this process can provide insight on potential areas of confusion (e.g., attending multiple appointments and acquiring insurance coverage), their opinions on current educational resources, how/why they decided on surgery as a treatment option, their understanding of obesity as a chronic condition, the role of clinical treatment in weight management, anticipated barriers and facilitators to postoperative behavioral adherence, and additional concerns regarding the procedure itself or preparing for the procedure (Table 1).
Qualitative data examining experiences of postoperative patients have provided initial insights into potential topics for preoperative education. 9 However, further topics should be explored with teenagers who have had MBS. This stakeholder group can provide additional information on what they wish they had known before surgery and challenges or facilitators related to adherence to postoperative requirements (e.g., consuming smaller portions, daily vitamin and supplement intake, and potential financial strain). In addition, they can provide insight as to what social support and interpersonal communication skills are necessary to navigate relationships after surgery and what health care system resources (e.g., behavioral specialists) may be required (Table 1).
Information from parents/guardians is also crucial to developing relevant tailored materials. To date, limited studies have examined the perspectives of parents/guardians regarding MBS among adolescents.6,24 This stakeholder group can provide further insight into challenges navigating the preoperative process, barriers, or facilitators to postoperative adherence, how they are supporting their adolescent through the preoperative process, their understanding of obesity as a disease, and the role of clinical treatment in weight management from their perspective (Table 1). Also, additional research is necessary to further understand the role of parents and guardians in decision-making for MBS among adolescents, but including their perspectives in tailored materials is crucial to ensuring resources are comprehensive.
Speaking with preoperative and postoperative adolescents and parents/guardians will help facilitate patient empowerment, providing them with feelings of control and inclusion. 11 Patients may feel more motivated and committed to the treatment plan, which could improve sustained psychosocial and cardiometabolic improvements.
Gathering information from these stakeholders can be completed through qualitative research approaches. After systematically assessing and reviewing perspectives from adolescents and parents/guardians, educational materials can be developed based on the input and topics generated by these stakeholder groups (Table 1). After materials are developed, consultation with a multidisciplinary team of providers will be necessary to ensure all relevant medical information is adequately covered as well.
Providers and adolescents will need to be consulted further to determine the best methods to implement the materials (e.g., determining whether adolescents prefer digital or printed materials and assessing barriers clinics will face in implementing materials). After the development of these tailored materials, it will be imperative to investigate their potential impact on postoperative behavioral adherence, and subsequently, cardiometabolic and psychosocial outcomes. Finally, a feedback loop should be created so adolescents undergoing MBS can consistently be involved in shared decision-making to ensure resources meet their needs and do not become outdated.
Qualitative work utilizing the Active Community Engagement Continuum is necessary to understand the needs of adolescent MBS patients and develop tailored educational materials to promote sustained improvements in psychosocial and cardiometabolic health. Qualitative research is the most powerful methodological option as it allows adolescents to inform researchers and clinicians using their own language, perspectives, verbiage, and needs in a way that can be translated to educational materials. The tailoring of materials will improve relevancy, promote behavioral adherence, and address pre- and postoperative expectations. Future directions include consultation with providers to ensure materials are comprehensive, implementation of materials, and assessing their impact on relevant outcomes.
Conclusion
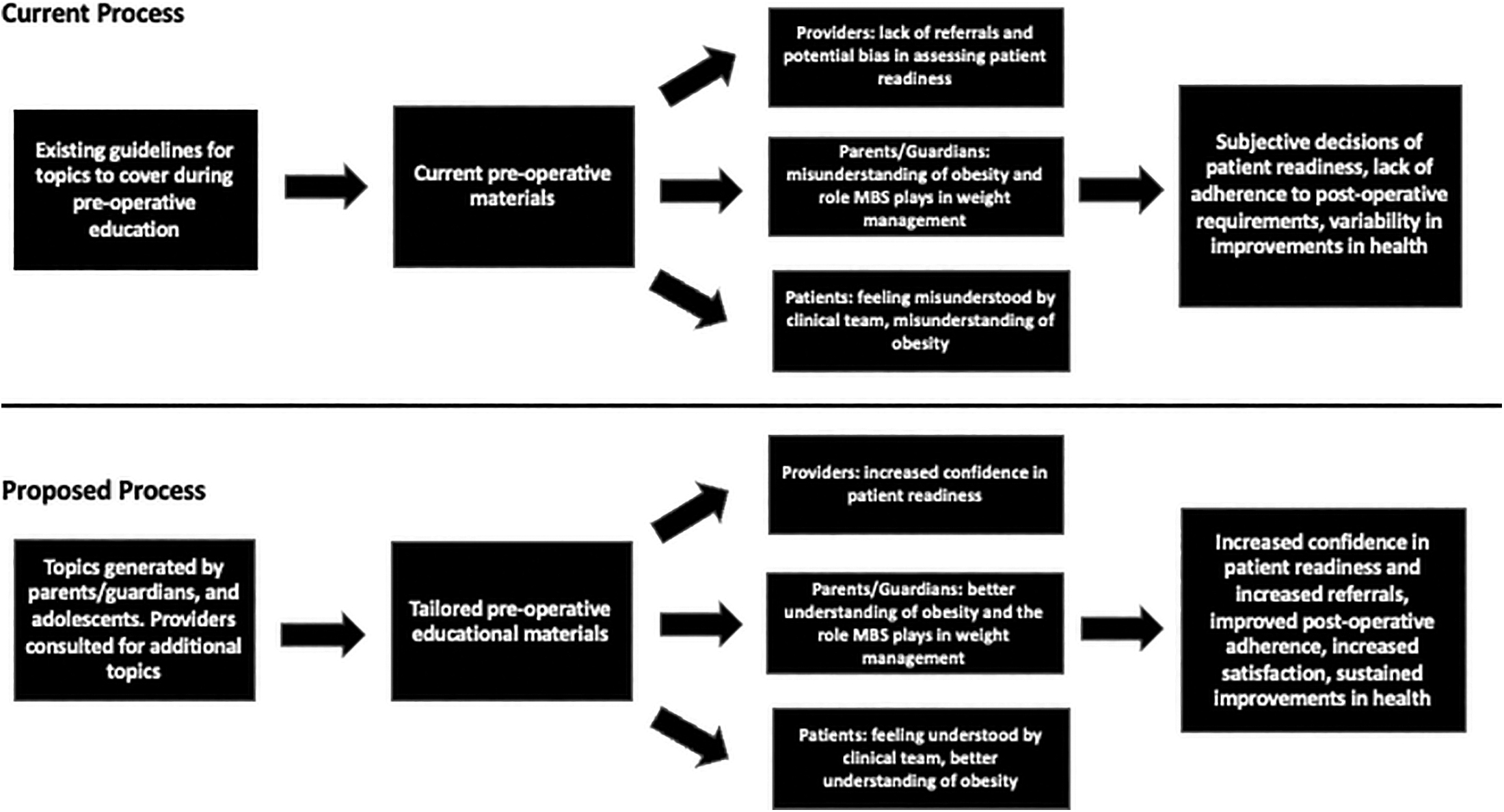
MBS is a safe and effective treatment option for adolescents. However, currently, adolescents report that their unique needs are not clearly understood, and that there are several topics they wish had been covered before surgery. 9 Furthermore, there is a paucity of research examining the perspective of parents/guardians of adolescents seeking MBS and what topics may be helpful for them to learn about preoperatively. Thus, tailored preoperative educational materials for adolescent MBS patients may help in ensuring teens, and their parents/guardians, feel comfortable and confident pursuing MBS as a treatment option.
Furthermore, these tailored materials may help providers feel less hesitant regarding patient readiness (Fig. 1). Thus, due to the effectiveness of MBS as a treatment option, and the recent clinical guidelines suggesting consideration of MBS for adolescents with severe cases of obesity, the development of tailored educational materials is a necessary endeavor to ensure the safety and satisfaction of teens, parents/guardians, and clinicians after surgery. 8
Impact Statement
Considering the recent release of clinical guidelines from the American Academy of Pediatrics for the treatment of obesity, there will likely be an increase in consideration of adolescents for metabolic and bariatric surgery (MBS). Although MBS is a safe and effective treatment option, there are opportunities to enhance the patient experience through the development of tailored preoperative educational materials.
Footnotes
Authors' Contributions
All persons who meet authorship criteria are listed as authors. F.A.N.H. drafted the initial article. A.A., A.V.B., S.M., and M.I.C. contributed to article revisions and edited for intellectual content. All authors approved the final version.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
FANH reports personal fees for consulting from Novo Nordisk and WW. MIC reports grants from nIH NHLBI, grants from WellCare Health Plans Inc., during the conduct of the study; personal fees and income from WW, personal feels for consulting from Amazon, consulting with Novo Nordisk where personal fees were not accepted, outside the submitted work.