
Abstract
Background:
Adverse social determinants of health (SDoHs), specifically psychosocial stressors and material hardships, are associated with early childhood obesity. Less is known about whether adverse SDoHs modify the efficacy of early childhood obesity prevention programs.
Methods:
We conducted a secondary analysis of publicly insured birthing parent–child dyads with Latino backgrounds participating in a randomized controlled trial of the Starting Early Program (StEP), a child obesity prevention program beginning in pregnancy. We measured baseline adverse SDoHs categorized as psychosocial stressors (low social support, single marital status, and maternal depressive symptoms) and material hardships (food insecurity, housing disrepair, and financial difficulties) individually and cumulatively in the third trimester. Logistic regression models tested effects of adverse SDoHs on StEP attendance. We then tested whether adverse SDoHs moderated intervention impacts on weight at age 2 years.
Results:
We observed heterogeneous effects of adverse SDoHs on outcomes in 358 parent–child dyads. While housing disrepair decreased odds of higher attendance [adjusted odds ratio (aOR) 0.52, 95% confidence interval (CI): 0.29–0.94], high levels of psychosocial stressors doubled odds of higher attendance (aOR 2.36, 95% CI: 1.04–5.34). Similarly, while certain adverse SDoHs diminished StEP impact on weight (e.g., housing disrepair), others (e.g., high psychosocial stress) enhanced StEP impact on weight.
Conclusions:
Effects of adverse SDoHs on intervention outcomes depend on the specific adverse SDoH. Highest engagement and benefit occurred in those with high psychosocial stress at baseline, suggesting that StEP components may mitigate aspects of psychosocial stressors. Findings also support integration of adverse SDoH assessment into strategies to enhance obesity prevention impacts on families with material hardships.
Trial Registration:
This study is registered on clinicaltrials.gov: Starting Early Obesity Prevention Program (NCT01541761); https://clinicaltrials.gov/ct2/show/NCT01541761
Introduction
Disparities in weight trajectories emerge in infancy, 1 prompting the development and implementation of early obesity prevention programs. Adverse social determinants of health (SDoHs) 2 —the conditions in which people are born, grow, and live—increase risk of childhood obesity 3 through poor feeding practices such as reduced breastfeeding 4 or nonresponsive feeding styles. 5 Adverse SDoHs may also adversely affect obesity prevention engagement and impacts.
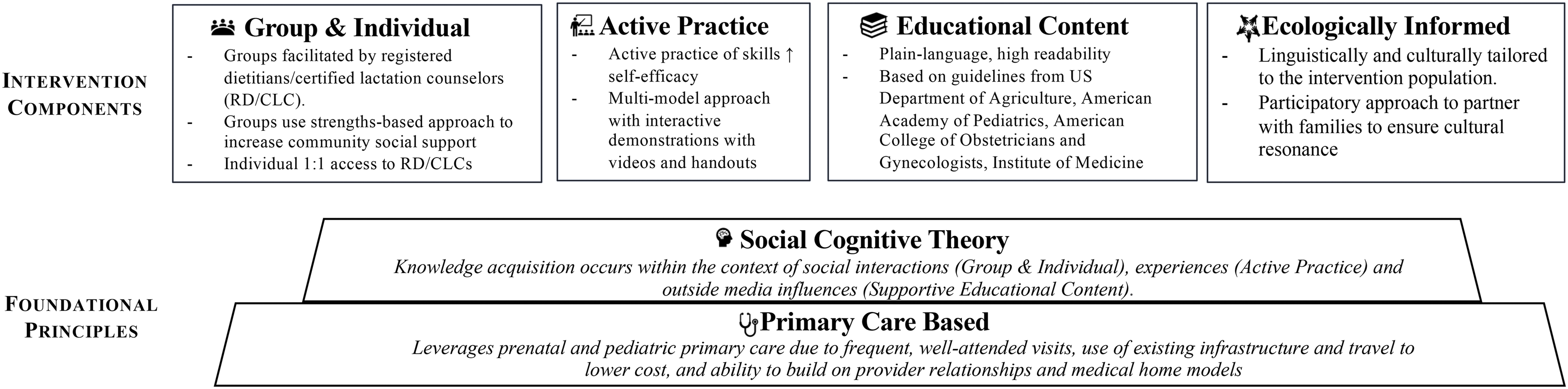
The Starting Early Program (StEP) is a primary care-based early childhood obesity prevention program that uses social cognitive theory and a group structure to promote healthy feeding beginning in pregnancy (Fig. 1). StEP is one of the first programs to show beneficial impacts on populations with high exposure to adverse SDoHs, with significantly lower weight-for-age z-scores (WFAz) at 2 years among StEP participants compared with controls. 6
Adverse SDoHs that influence health behaviors include two key domains: (1) psychosocial stressors or social conditions that intensify emotional stress and (2) material hardships or an inability to meet basic needs such as food and shelter.7,8 Adverse SDoHs may affect intervention impacts through several mechanisms. In families with young children, financial difficulties may exacerbate a lack of child care or transportation, increasing barriers to attendance at the in-person program.9–11 Alternatively, adverse SDoHs such as psychosocial stress or food access may interfere with one's capacity to follow program recommendations. 12
An ongoing challenge to population-level preventive initiatives is the engagement of families most at risk. 13 Yet, some program evaluations have shown that parenting intervention benefits were concentrated among participants with psychosocial stressors such as low social support and depression.14–16 Understanding intervention efficacy in the context of adverse SDoHs may highlight subgroups that are either more or less likely to benefit from the intervention, informing adaptations to enhance positive impacts.
While adverse SDoHs are widely understood to disrupt healthy feeding practices that prevent obesity, no studies, to our knowledge, have assessed whether adverse SDoHs modify the efficacy of early obesity prevention programs. To address this gap, we systematically examined whether (1) adverse SDoHs decreased StEP attendance and (2) adverse SDoHs modified weight impact at child age 2 years.
Methods
Study Overview
This was a secondary analysis of a randomized controlled trial (RCT) in the prenatal and pediatric clinics of an urban public hospital (Bellevue Hospital Center) and an affiliated health center in New York City. It was approved by the Institutional Review Board of NYU Grossman School of Medicine and NYC Health + Hospitals and registered on clinicaltrials.gov (NCT01541761). The trial was statistically powered for weight impacts, but we collected data on adverse SDoHs to examine subgroup impacts as part of the original study aims.
Starting Early Program
Figure 1 displays StEP components, where bilingual Spanish/English-speaking registered dietitians and certified lactation counselors facilitated nutrition and parenting support groups. StEP delivered 12 sessions, including two individual (third trimester; postpartum) and 10 group sessions for children between the ages of 1 and 24 months. Beginning at 1 month, StEP group sessions took place over 1 hour at lunchtime in coordination with the physician visit preceding or following the StEP session. Both the control and intervention groups received standard primary care.
Participants
All pregnant participants with a first prenatal visit between August 2012 and December 2014 were screened for eligibility and randomized at 32 weeks of pregnancy to either an intervention group that received StEP or a control group that received only standard primary care. Eligibility included age (at least 18 years), ethnicity (self-identification as Latina/o or Hispanic), language (English or Spanish speaking), and a singleton uncomplicated pregnancy with delivery after 32 weeks of gestation with planned pediatric care at the study sites. We excluded participants with severe medical, psychiatric illness, or fetal anomalies. We did not exclude infants born prematurely between 32 and 37 weeks of gestational age.
In the United States, Latino or Hispanic families have been disproportionately impacted by obesity and adverse SDoHs such as food insecurity, particularly in households with young children.17,18 The original StEP was culturally and linguistically tailored to serve Latino and Hispanic families. We use the term Latino, but acknowledge the limitations of using either Latino or Hispanic to generalize any sample of individuals.
SDoH Assessments
We collected adverse SDoH data during the third trimester as part of baseline enrollment. Two adverse SDoHs with prevalence below 10% [domestic violence (9.1%) and low neighborhood safety (8.0%)] were not included. Researchers have established that cumulative experiences of SDoHs have additive effects on child health. 19 The goal of our assessments was to examine both individual and cumulative effects of adverse SDoHs studied previously within the context of early obesity.4,5,20
We grouped adverse SDoHs in two domains likely to affect health through different pathways7,21: psychosocial stressors that intensify emotional stress (low social support, single marital status, and maternal depressive symptoms) and material hardships when families are unable to meet basic needs (food insecurity, housing disrepair, and financial difficulties). Different intervention approaches mitigate these domains—psychosocial stressors need behavioral health interventions 22 and material hardships require resource connections.2,23
Finally, we use the term “social determinants of health” to align with literature about adverse SDoHs and early childhood obesity, but we acknowledge evolving efforts to adopt the term “drivers” to better reflect a complex and modifiable social context.
Psychosocial Stressors
Low social support
We assessed low social support using an item from the validated Maternal Social Support Index, which asks participants the number of people they could count on in times of need. 24 Participants who reported fewer than two people were considered to have low social support, as per prior work showing a protective effect of two or more people on child weight. 20
Marital status
Parents with single marital status have been shown to be at increased risk for decreased social support, increased stress, and low socioeconomic status.25,26 We used the question, “How would you describe your marital status?” Responses were dichotomized as single (single, divorced, or widowed) versus legally married or living as married.
Maternal depressive symptoms
We used the Patient Health Questionnaire-9 (PHQ-9), a validated tool that includes nine questions assessing depressive symptoms (0–27), with higher scores indicating greater symptoms. 27 The PHQ-9 score was dichotomized using a clinically validated cut point of 5 or higher to indicate at least mild depressive symptoms. 27
High psychosocial stress
To identify maternal–child pairs with high exposure to psychosocial stressors, we counted the number of stressors of the three psychosocial stressors described above and dichotomized at two or more stressors, as per prior literature examining additive effects of adverse SDoHs.7,8
Material Hardships
Food insecurity
We assessed food insecurity using the Core Food Security Module from the US Department of Agriculture (USDA). 22 The module contains 10 questions assessing food insecurity in the previous 12 months. We classified households as food insecure if they reported three or more food insecure conditions, as per USDA guidelines. 22
Housing disrepair
We assessed housing disrepair using the Survey of Income and Program Participation (SIPP), a nationally representative longitudinal survey administered and validated by the US Census Bureau to evaluate national economic well-being. 23 Researchers have identified associations between SIPP's questions about financial and housing conditions and health outcomes.28,29
We classified housing disrepair if they reported any of the following: (1) a leaking roof or ceiling; (2) a toilet, hot water heater, or other plumbing that does not work; (3) broken windows; (4) exposed electric wiring; (5) rats, mice, and roaches or other insects; (6) holes in the floor; and (7) open cracks or holes in the walls or ceiling.
Financial difficulties
We assessed financial difficulties using two questions from the SIPP 23 : (1) “Have you had serious financial problems or have you been unable to pay monthly bills or rent or mortgage during the last 12 months?” (2) “In the past 12 months, has there been a time when your household had service turned off by the gas, electric, telephone or oil company because payments were not made?” We classified participants as having financial difficulties if they said yes to either question.
High material hardships
To identify participants with high exposure to material hardships, we counted the number of hardships of the three material hardships described above and dichotomized at two or more hardships, as per prior literature examining additive effects of adverse SDoHs.7,8
Higher StEP Attendance
We defined higher attendance at the highest tertile (attending 10 sessions or more) based on tested StEP outcomes: early childhood obesity rates decreased by 9.8% (p = 0.01) at this cutoff. 6
Child Anthropometrics
We collected child anthropometrics at 2 years from the medical record. These measurements were obtained as part of routine primary care by trained medical assistants. Due to validity concerns regarding clinically obtained lengths, 30 we used WFAz as our primary outcome, calculated using the World Health Organization Anthro macro. 31
Covariates
We treated characteristics that were not psychosocial stressors or material hardships as covariates in analyses examining associations between adverse SDoHs and higher StEP attendance. These included maternal age (years), US nativity (yes/no), high school completion (yes/no), prepregnancy obesity status (yes/no), child's firstborn status (yes/no), and child's assigned sex.
Statistical Analyses
In the full trial, 533 participants were randomized either to an intervention group receiving StEP (n = 266) or a control group (n = 267), with 529 live births. 6 We used the same analytic sample from the published RCT (additional details available 6 ), where most notably, weight outcomes were available for 358 (67.7%) children at 2 years. These 358 children did not differ significantly in baseline characteristics from the 175 participants missing child outcome data.
We summarized our analytic sample across control and intervention groups. In addition to the covariates above, we reported Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) participation, employment status, birth weight, and prematurity (birth at <37 weeks' gestational age). Within the intervention group, we used unadjusted and adjusted logistic regression models to investigate whether adverse SDoH variables were associated with higher StEP attendance.
Next, we performed stratified independent sample t-tests by subgroup to determine mean differences in WFAz by intervention group, using separate tests based on the presence or absence of each adverse SDoH variable. We used Cohen's d to determine effect sizes and to interpret the practical meaning of significant intervention outcomes.
Finally, we tested moderation in separate adjusted regression models that included an interaction term calculated by multiplying together the dichotomous variables defined for the moderator (presence or absence of adverse SDoH variable) and the predictor (intervention group). Statistical analyses were performed using Stata/SE, version 15 (Stata Corp, College Station, TX).
Results
Table 1 displays baseline characteristics for the intervention and control groups. About a quarter of mothers were working (25.7%), 18.4% were US-born, and the majority (88.0%) participated in the WIC program. There was frequent exposure to adverse SDoHs; only 20% had no exposure. However, there was heterogeneity in experiences of adverse SDoHs, with 19% having high psychosocial stress and 26.3% having high material hardships.
The analytic sample was followed from pregnancy to 24 months.
The intervention group received the Starting Early Program intervention, and the control group received routine primary care.
Defined as two or more psychosocial stressors.
Defined as two or more material hardships.
SD, standard deviation; WIC, women, infants, and children.
Adverse SDoHs and StEP Attendance
Table 2 shows that single participants had greater odds of higher StEP attendance than those who were married or living as married [adjusted odds ratio (aOR) 2.39, 95% confidence interval (CI): 1.17–4.87]. Participants with high psychosocial stress had greater odds of higher StEP attendance than those who did not (aOR 2.33, 95% CI: 1.02–5.31).
Higher attendance defined by the highest quartile of attendance (10 or more sessions).
Adjusting for maternal age, education, US-born status, prepregnancy obesity status, and child's sex and firstborn status.
Defined as two or more psychosocial stressors.
Defined as two or more material hardships.
p < 0.05; **p < 0.01.
CI, confidence interval; OR, odds ratio.
As for material hardships, participants with housing disrepair had half the odds of having higher StEP attendance (aOR 0.52, 95% CI 0.29–0.94) than those without housing disrepair. Other adverse SDoHs did not have significant associations with higher StEP attendance.
Intervention Impacts by Adverse SDoHs
Figure 2 displays stratified analyses of StEP impacts on WFAz at age 2 years for each adverse SDoH. Two graphic patterns are noted. Pattern A (shaded), noted for single marital status, food insecurity, housing disrepair, and financial difficulties, showed that the StEP group had less of a reduction in weight when the adverse SDoH outcome was present. For example, in the control group, those with and without housing disrepair had similar WFAz (0.79 vs. 0.82), but in the intervention group, those with housing disrepair continued to have much higher WFAz than those without (0.76 vs. 0.44).

Pattern B (not shaded), noted for low social support, depressive symptoms, and high psychosocial stress, showed that StEP had a greater impact on weight when the specific adverse SDoH was present, buffering the effects of the adverse SDoH. For example, in the control group, WFAz were higher in those exposed to low social support than those not exposed (1.13 vs. 0.74), but in the intervention group, WFAz were similar with or without exposure to low social support (0.58 vs. 0.53).
Table 3 displays the intervention effect size for those with and without each adverse SDoH. For those with high psychosocial stress, we found that the intervention had a significant impact on WFAz, with a medium to large effect size (Cohen's d = 0.70, 95% CI: 0.21–1.19), but not in those without high psychosocial stress (Cohen's d = 0.11, 95% CI: −0.12 to 0.34). For those with high material hardships, we found that the intervention did not have a significant impact on WFAz (Cohen's d = 0.09, 95% CI: −0.32 to 0.49).
Moderation of Starting Early Program Weight Impacts by Social Determinants of Health
Moderation tested in models with the interaction term calculated by multiplying together variables defined for the moderator (presence or absence of adverse SDoH variable) and the predictor (intervention group). These models adjusted for maternal age, education, US-born status, prepregnancy obesity status, and child's sex and firstborn status.
Defined as two or more psychosocial stressors.
Defined as two or more material hardships.
p < 0.05; **p < 0.01.
SDoH, social determinant of health.
However, for those without high material hardships, we found that the intervention had a significant impact on WFAz, with a small effect size (Cohen's d = 0.28, 95% CI: 0.04–0.52). The interaction term was statistically significant for high psychosocial stress only (B = −0.63, p = 0.03). Although not statistically significant, the interaction term for low social support was also notable (B = −0.51, p = 0.07).
Discussion
In this study, we found that the effects of adverse SDoHs on the StEP group were multifaceted, with heterogeneous effects on attendance and weight impact. This study builds upon existing knowledge about interventions in families with economic disadvantage 32 by examining adverse SDoHs. These findings support future strategies to integrate early childhood obesity programs with programs that address adverse SDoHs to optimize outcomes.
While the majority of material hardships were not associated with attendance, we found that housing disrepair decreased odds of higher StEP attendance. Housing disrepair may increase the risk for multiple moves or be a proxy for other structural factors such as safety concerns, which can decrease family capacity to attend in-person programs. 33 Future studies should examine how adaptations such as virtual delivery can increase engagement of participants with housing disrepair.34–38
In contrast to our findings on housing disrepair, high psychosocial stress more than doubled the odds of higher StEP attendance. Most early childhood interventions show that families with psychosocial stress have decreased attendance.13,39 The StEP group structure is designed to leverage community strengths by building social support or perceived assistance available through social relationships. Studies show that parents with psychosocial stress particularly benefit from social support, 40 which may increase engagement and attendance.
Even though we did not detect direct associations with attendance outside of housing disrepair, we found that StEP had decreased efficacy when participants were experiencing material hardships. These results extend prior studies showing how adverse SDoHs reduced impacts of parenting interventions seeking to improve early developmental outcomes and that adverse SDoHs may also reduce intervention impacts on early weight outcomes.14–16
Previous StEP evaluations have detected significant associations between increased StEP attendance and greater impacts on weight outcomes 6 ; studies have also conjectured that low attendance is a likely mechanism through which adverse SDoHs decrease program impacts.27,41 However, only housing disrepair significantly decreased odds of adequate StEP attendance, while StEP still had decreased efficacy in the setting of other adverse SDoHs.
Future qualitative studies should describe parental perceptions about how adverse SDoHs may decrease impacts through alternative pathways beyond attendance, potentially through additional barriers presented by food insecurity or financial difficulties.
On the other hand, we found that StEP appeared to buffer, or decrease, the adverse influence of multiple measures of psychosocial stress on child weight (low social support and maternal depressive symptoms). This “buffering” effect suggests that StEP may have been able to increase engagement among those with psychosocial stress, as evidenced by our attendance findings. StEP is designed to improve knowledge and skills related to feeding practices. Its efficacy may be augmented because of the increased social support inherent to StEP's group structure,20,42,43 which may mitigate mechanisms associated with poor feeding practices in the setting of increased psychosocial stress.21,44
The majority of our participants (∼80%) were immigrants from Latin American countries, who may have been at higher risk of isolation. The ability of StEP to apply a strength-based approach to build social support networks through a group-based intervention may provide greater benefit in this population.
Single marital status functioned uniquely, in that while it doubled the odds of higher StEP attendance, weight impacts were diminished in this subgroup. This may reflect the complexity of single marital status, in which participants may be at higher risk for both lower social support and material hardship.25,26
Given that StEP is a primary care-based intervention, program engagement may be synergistic with health care system engagement, thus facilitating increased receipt of preventive care supporting family medical resources for healthy practices. These findings are foundational to support future work to layer levels of prevention with primary care programs that target the same critical life stage with early parenting support in the setting of adverse SDoHs, such as HealthySteps. 22 Future research should also examine how adverse SDoHs may interact with the mode of intervention delivery; for example, whether SDoH experiences predict increased engagement in individual versus group interventions.
This study had many strengths as it was built upon an RCT with detailed assessment of baseline adverse SDoHs and clinically measured weight outcomes at age 2 years.
Limitations in this study include the self-reported nature of adverse SDoHs, which may result in recall and social desirability biases. Future studies may consider including other adverse SDoHs such as maternal anxiety as a psychosocial stressor 21 or child care precarity as a material hardship. 45 Participants were recruited at a public hospital serving low-income families that self-identified as Hispanic or Latino, limiting generalizability to other populations. We used WFAz rather than a more ideal weight for length because of implausible lengths obtained from the medical record. Finally, our study question relied on subgroup analyses, which may have been underpowered for our interaction analyses.
Conclusions
This study broadens current literature by describing the influence of adverse SDoHs on StEP weight impacts. We detected heterogeneity in the influence of adverse SDoHs on StEP attendance and impacts, endorsing efforts to integrate intervention components to address adverse SDoHs as essential context for optimizing program impacts.
Impact Statement
This study is one of the first to describe how adverse social determinants of health affect attendance and modify the efficacy of an early childhood obesity prevention program beginning in pregnancy. These findings endorse efforts to measure and address the detailed social context of health practices to optimize program impacts.
Footnotes
Acknowledgments
The authors would like to thank the StEP staff who contributed to this project.
Authors' Contributions
C.D.-L. and R.S.G. were involved in conceptualization, methodology, analysis, and writing—original draft preparation. M.J.M. and M.W.K. were involved in investigation, data curation, analysis, and writing—reviewing and editing. C.N.K. and M.A.S. were involved in data curation, analysis, and writing—reviewing and editing. A.L.M. was involved in methodology and writing—reviewing and editing. The authors of this article take responsibility for the reported research. All authors approved the article as submitted.
Funding Information
All phases of this study were supported by the National Institute of Food and Agriculture, US Department of Agriculture, under award number 2011-68001-30207. Funding was also provided by the National Institutes of Health/National Institute of Child Health and Human Development (K23HD081077; PI Gross), National Heart, Lung, and Blood Institute (K23HL159326; PI Katzow), and National Institute of Environmental Health Sciences (K23ES035461: PI Duh-Leong). The funders/sponsors did not participate in the work.
Author Disclosure Statement
No competing financial interests exist.