
Abstract
Background:
Adolescent obesity rates continue to rise. A better understanding of who engages in emotional eating, a maladaptive eating style, is needed. Despite emotional eating being a frequent research target, the prevalence of emotional eating in US adolescents is currently unknown.
Methods:
Nationally representative adolescents (n = 1622, m = 14.48 years, 63.8% non-Hispanic White, 50.6% female) reported eating behaviors in the National Cancer Institute’s Family Life, Activity, Sun, Health, and Eating (FLASHE) study. Frequencies and one-way ANOVAs were conducted to examine the rates of emotional eating across demographic and weight status groups. Correlations between emotional eating and dietary intake were examined.
Results:
In total, 30% of adolescents engaged in emotional eating. Older adolescents (35% of 17-year-olds), females (39%), non-Hispanic White individuals (32%), and adolescents with obesity (44%) had significantly higher rates of emotional eating. Controlling for weight status, greater adolescent emotional eating was correlated with more frequent intake of energy-dense/nutrient-poor foods (β = 0.10, p < 0.001), junk food (β = 0.12, p < 0.001), and convenience foods (β = 0.13, p < 0.001).
Conclusions:
This study fills a critical gap by providing insight into how common adolescent emotional eating is and highlighting demographic factors that are associated with higher rates. Nearly a third of adolescents in the United States reported eating due to anxiety or sadness, with rates higher in older adolescents, girls, non-Hispanic White adolescents, and adolescents with obesity. Emotional eating was associated with consuming less healthy foods, which conveys immediate and long-term health risks. Practitioners can intervene with emotional eating to reduce obesity and comorbid health risks.
The current rates of adolescent obesity have reached 20.6% and continue to rise. 1 Understanding modifiable targets within prevention/intervention models is an urgent public health priority to prevent comorbidity and mortality.2–5 Emotional eating is the tendency to eat in response to emotions, even when not physically hungry. 6 Adolescents engaging in emotional eating may prefer highly palatable, energy-dense foods 7 and rely on cues other than hunger and satiety to guide their eating habits, a behavior strongly associated with weight gain.8–10 Researchers and clinicians have identified emotional eating as an important intervention target,7,11–14 and yet, the prevalence rate of emotional eating in adolescents remains obscure and rarely reported in extant literature. This study addresses that critical gap using a large national dataset of US adolescents to characterize the prevalence of emotional eating by demographic characteristics.
The extant literature does not clearly characterize the percentage of adolescents who engage in emotional eating. Previous research has appropriately reported means/standard deviations for emotional eating scales. 15 However, readers cannot deduce the percentage of youth engaging in emotional eating from the sample means. The few studies that report frequencies have not yet been with a US national sample. For instance, Zoromba et al. reported emotional eating percentages by weight category in Egyptian adolescents (n = 184). 16 Emotional eating as a construct encompasses stress-induced eating, which occurs when people eat highly palatable foods following a stressor. Jääskeläinen et al. reported stress-eating prevalence in a large sample of adolescents from the Northern Finland Birth Cohort. 17 Stress-eating was more common in 16-year-old girls (43%) than among boys (15%). They also found that adolescents engaging in stress-eating had a higher prevalence of overweight and obese weight status. 17 The largest US-based study that reported percentages recruited seventh- and eighth-grade Los Angeles adolescents (n = 505, mean = 12.55 years), which found no gender differences in emotional eating rates 18 and did not report emotional eating rates by other demographic characteristics. These (pre)adolescents were young, and data are needed on older adolescents. Historically, Kagan and Squires (1984) reported that 11% of female adolescents engaged in emotional eating. 19 As the food environment has become more obesogenic (e.g., larger portion sizes) 20 and obesity prevalence in the USA continues to rise, 21 more recent estimates of emotional eating are needed.
Emotional eating is a learned behavior,22,23 in which individuals experience reinforcement of emotional eating if eating alleviates strong emotions. Beginning in childhood, 24 youth learn that eating certain energy-dense, nutrient-poor foods can alleviate uncomfortable emotions. Caregivers offering food for comfort (i.e., emotional feeding) may contribute to that learned association,25,26 as well as frequent exposure to eating certain foods at joyous occasions (i.e., birthday cake, extended family dinners). Related stress-eating literature is informative from a physiological lens. Elevations in cortisol following a stressor may increase insulin secretion, 27 promoting overeating. Dallman’s 27 learning theory outlines that stress-eating is reinforced because eating palatable foods does decrease discomfort. This reinforcement underlies the learned association between eating and emotional homeostasis.
Adolescence is a particularly important developmental period for understanding and intervening with emotional eating. Adolescents have increased eating autonomy. 28 Eating behaviors formed in adolescence may lay the foundation for lifelong patterns. 29 Adolescents experience a developmental mismatch between still-developing emotional regulation abilities and expectations for healthy decision-making. 30 Prospective longitudinal Australian data show an increase in mean self-report emotional eating scores from fifth to seventh grade, 31 providing some indication that emotional eating may increase in adolescence. When adolescents experience emotional dysregulation, they may choose maladaptive coping strategies such as emotional eating.
Hypotheses
Because emotional eating is a learned behavior 32 that can develop into a habit over time, 27 we expected that emotional eating would increase with adolescent age. Based on the extant literature,15,17,33 we also expected that female adolescents would be more likely to engage in emotional eating than male adolescents, and that adolescents with overweight or obesity would be more likely to engage in emotional eating than adolescents in a lower weight status category. We did not have an a priori hypothesis regarding rates of emotional eating by socioeconomic status or race/ethnicity in the USA but report the rates by White or Black race and Hispanic ethnicity. We examined the rates of emotional eating reported by the adolescents’ participating parents to supplement the findings. As adult research has shown differential relationships between distinct emotions and emotional eating,34–36 we explored prevalence rates for eating in response to sadness and anxiety separately. Finally, we examined dietary correlates of emotional eating, expecting that more emotional eating would be associated with more frequent consumption of energy-dense, nutrient-poor foods.
Method
Transparency and Openness Statement
This study uses publicly available cross-sectional data from the National Cancer Institute’s Family Life, Activity, Sun, Health, and Eating (FLASHE) study. 37 The sample was drawn from the Ipsos Consumer Opinion Panel and is similar to the US general population on sex, education, income, age, household size, and region. These data may be accessed from https://cancercontrol.cancer.gov/brp/hbrb/flashe-study.
Participants and Procedures
A national sample of US adolescent–parent dyads (n = 1622) 37 completed two online surveys assessing health-related behaviors. Participants completed electronic informed consent/assent and were compensated $5 per survey. All study procedures received ethical approval from the National Institutes of Health (NIH) and the Westat IRB.
Measures
Sociodemographic Variables
Sex was reported as male or female, and publicly available race and ethnicity information were reported as one variable with four levels: Hispanic, non-Hispanic Black, non-Hispanic White, and Other. As an indicator of socioeconomic status, parents reported whether adolescents were eligible to receive Free or Reduced-Priced School Lunch, which is based on family size to household income.
Weight Status
Parents reported their adolescents’ height and weight, which were converted into body mass index (BMI) percentiles using the Centers for Disease Control and Prevention’s SAS program. BMI percentile was then classified as underweight (<5th percentile), healthy weight (5th–84.99th percentile), overweight (85th–94.99th percentile), or obese (≥95th percentile). 38
Adolescent Emotional Eating
The FLASHE survey was developed in consultation with a group of 19 scientific advisors who were content experts in health behavior research and reviewed the survey items for congruence with validated measures. 37 Two items from the Eating in the Absence of Hunger Questionnaire (EAH-C) 39 were included (e.g., “How often do you start or continue to eat when you’re not hungry because…(Item 1) you feel sad or depressed? (Item 2) you feel anxious or nervous?”). Participants rated emotional eating frequency using the following scale: 1 (Never), 2 (Rarely), 3 (Sometimes), 4 (Often), or 5(Always). The Spearman–Brown coefficient estimate for reliability for two-item scales was good–excellent (ρ = 0.87). Sadness and anxiety were examined separately, and the two emotional eating questions were averaged into a total score. Consistent with Braet et al. 8 who used a score of 3+ to indicate emotional eating in children and adolescents, scores of >3 corresponding to Sometimes, Often, and Always responses were dichotomized as endorsement of emotional eating. 8
Dietary Intake
Adolescents responded to 27-item gauging daily food/drink frequency 37 with the following response options: I did not drink/eat [specific beverage/food] during the past 7 days, 1–3 times in the past 7 days, 4–6 times in the past 7 days, 1 time per day, 2 times per day, or 3 or more times per day. The first three weekly response options were divided by 7. Items were totaled, producing subscales that represent the average number of daily servings of sugar-sweetened beverages (e.g., sweetened juices/soda/energy drinks), junk foods (e.g., candy/cookies/chips/frozen desserts), and convenience foods (e.g., pizza/tacos/fried chicken). For energy-dense, nutrient-poor foods, a total score was calculated by summing the frequency of common less healthy foods/drinks. The FLASHE study team classified reported intakes corresponding to z-scores ≥3.29 as overestimates (≥99.95% of scores in a normal distribution), and the next closest value was imputed. 40 The FLASHE Dietary Screener has good validity, as it strongly corresponds to 24-hour dietary recalls. 40
Analytic Plan
The frequency of emotional eating endorsement was calculated for each age, sex, socioeconomic status, race/ethnicity, and weight status classification (Table 1 contains rates by specific emotion, and Fig. 1 contains overall emotional eating rates). One-way ANOVAs were calculated to determine if groups were statistically different in average emotional eating scores (continuous variable). Linear regressions controlling for weight status were conducted with the frequency of emotional eating (continuous variable) predicting dietary outcomes.
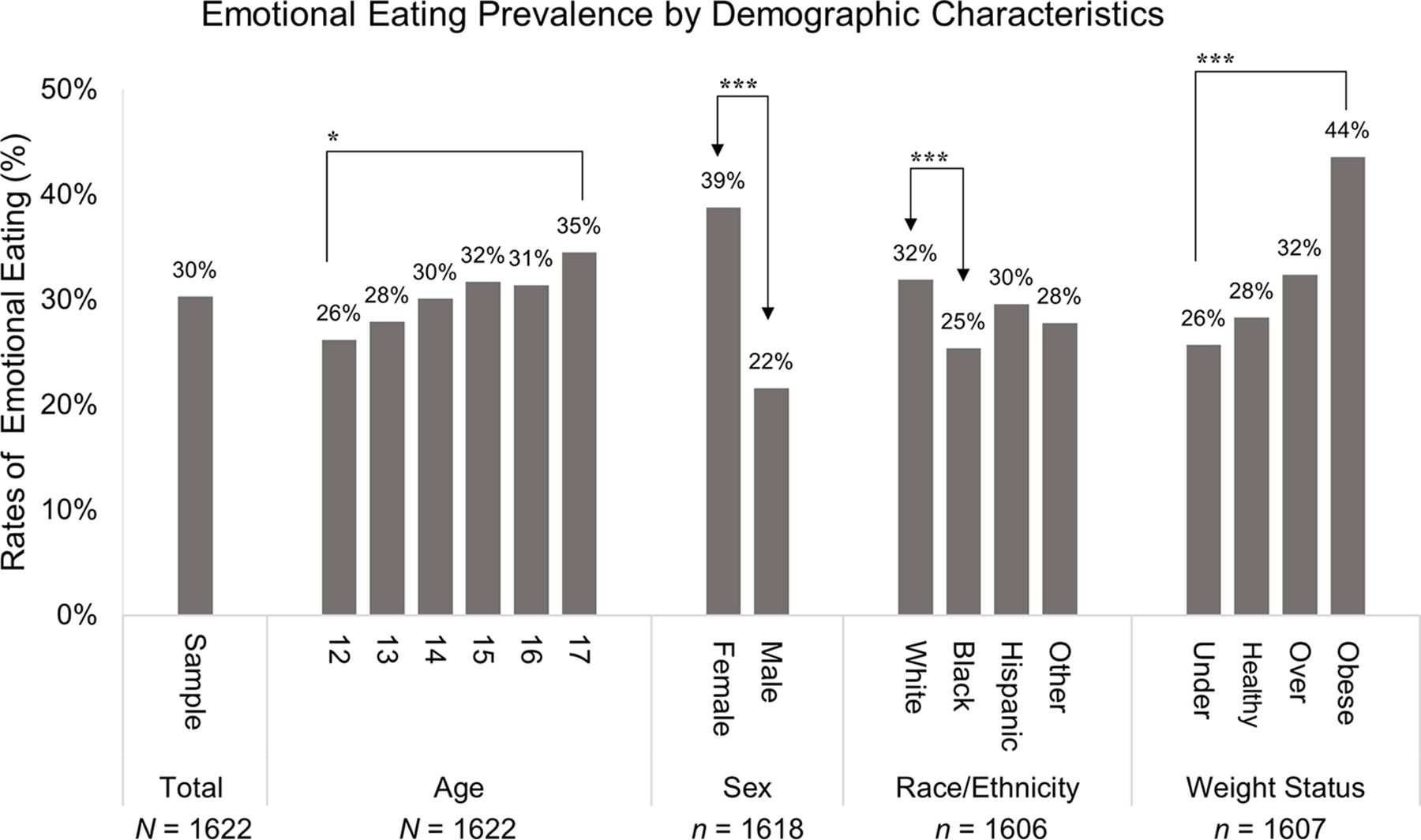
Sample rates of emotional eating by demographic characteristics. Significant within-group differences in emotional eating rates were found for age (p = 0.028) and sex (p < 0.001) such that older age and female sex corresponded with higher rates of emotional eating. Regarding race and ethnicity, adolescents reporting White racial identity endorsed significantly more emotional eating than those reporting Black racial identity (p = 0.001). Higher weight status was also indicative of more emotional eating (p < 0.001). *p < .05. ***p ≤ .001.
Frequencies for Emotional Eating Prevalence for Sadness and Anxiety Emotions Separately by Demographic Characteristics
Results
Participant Characteristics
Age (mage = 14.48) was well-represented with n = 218 12-year-olds, 322 13-year-olds, 272 14-year-olds, 286 15-year-olds, 324 16-year-olds, and 200 17-year-olds. Female adolescents comprised 50.6% of the sample. Participants reported race/ethnicity as 63.8% non-Hispanic White, 16.9% Black, and 9.9% Hispanic. The FLASHE study team collapsed the 9.4% of respondents who indicated another race/ethnicity category into an “Other” category.
Prevalence Rate for the Total Sample
As depicted in Figure 1, 30% of the total adolescent sample engaged in emotional eating (average of both sadness and anxiety items); 39.9% of parents reported emotional eating. Eating due to sadness and eating due to anxiety were highly correlated (r = 0.75), but there were nuanced differences in prevalence rates between these two emotions (see Table 1). Overall, rates to eating due to sadness were 34.6%, compared to anxiety at 39.9%, with a small significant mean difference in continuous scores (msad = 2.12, manxiety = 2.24, t = 5.30, p < 0.001).
Age
In total, 26.2% of 12-year-olds and 34.5% of 17-year-olds engaged in emotional eating. A one-way ANOVA examined age as a predictor of emotional eating scores, with a significant relationship between older age and higher emotional eating scores [F(5,1616) = 2.53, Mse = 0.97, p = 0.028, η2 = 0.008, 95% CI for effect size = 0–0.015].
Sex
In total, 38.8% of female participants and 21.6% of male participants engaged in emotional eating. A one-way ANOVA examined the relationship between sex and emotional eating scores, with female adolescents engaging in more emotional eating [F(1,1616) = 64.98, Mse = 0.94, p < 0.001, η2 = 0.04, 95% CI for effect size = 0.02–0.06].
Race/Ethnicity
In total, 31.9% of White participants, 25.4% of Black participants, 29.6% of Hispanic participants, and 27.8% of adolescents reporting another race/ethnic category engaged in emotional eating. A one-way ANOVA indicated significant group differences in emotional eating scores by race/ethnicity [F(3,1602) = 5.50, Mse = 0.96, p = 0.001, η2 = 0.01, 95%CI for effect size = 0.002–0.02]. Post hoc tests for multiple comparisons indicated that White adolescents [m = 2.11, SD = 0.92] had higher emotional eating scores than Black adolescents [(m = 1.99, SD = 0.99; p < 0.001]. There were no other significant group differences in race/ethnicity.
Socioeconomic Status
Of adolescents eligible for Free or Reduced-Priced School Lunch, 32.6% endorsed emotional eating. Of adolescents not eligible based on higher household income to family size, 29.6% reported emotional eating (no significant group difference).
Weight Status
Results indicated that 25.7% of participants in the underweight category, 28.3% of participants in the healthy weight category, 32.4% of participants in the overweight category, and 43.6% of participants in the obese category engaged in emotional eating. A one-way ANOVA indicated adolescents with higher weight status classification engaged in more emotional eating [F(3,1603) = 9.82, Mse = 0.96, p < 0.001, η2 = 0.02, 95%CI for effect size = 0.01–0.03].
Dietary Correlates of Emotional Eating
In regression models controlling for adolescent weight status, adolescents with greater emotional eating scores had significantly greater dietary intake of energy-dense/nutrient-poor foods (β = 0.10, p < 0.001), junk food (β = 0.12, p < 0.001) and convenience foods (β = 0.13, p < 0.001). Interestingly, although there was a significant bivariate correlation between emotional eating and sugar-sweetened beverages (r = 0.06, p = 0.03), this relationship was suppressed when controlling for adolescent weight status (emotional eating β = 0.04, p = 0.09; weight status β = 0.08, p = 0.003).
Discussion
This study leveraged a large, cross-sectional, nationally representative study of US adolescents to characterize emotional eating prevalence by demographic factors. Thirty percent of adolescents reported emotional eating in general, with 34.6% at least sometimes eating when sad and 39.9% eating when anxious. Adolescents who were female, non-Hispanic White, older, and in an obese weight category engaged in significantly more emotional eating. The demographic results are consistent with existing research using large national samples in other countries 17 and add new information regarding race/ethnicity differences in the USA. While 31.9% of White adolescents were classified as emotional eaters compared to 25.4% of Black adolescents, when examining the continuous mean scores of emotional eating, there were statistically significant but not clinically meaningful differences (mean score of 2.11 versus 1.99). Additionally, supplemental parent data revealed that adults reported rates of emotional eating (39.9%) consistent with other research with adults on a variant of emotional eating (38% adults engaging in stress-eating). 41 Finally, adolescents with more emotional eating consumed more energy-dense/nutrient-poor foods, junk foods, and convenience foods, but not sugar-sweetened beverages, when accounting for weight status. However, the relationships between emotional eating and dietary intake were small effect sizes.
Few studies have reported percentages of adolescents who emotionally eat, with no recent published US national data. Van Strien and colleagues 42 reported that emotional eating mean scores in an adult Dutch 2009 sample were substantially higher than those in a similar Dutch sample collected in 1983. Similarly, the results from the current US sample are substantially higher than the percentages reported by Kagan and Squires in 1984. 19 Specifically, 30% of this 2014 sample vs. 7% of the 1984 sample were classified as emotional eaters using similar criteria with similar sample sizes and demographic characteristics. Emotional eating appears to be increasing over chronological time.
This study contributes to existing theory that emotional eating is a learned behavior that may increase from childhood to adulthood. Support for this theory comes from twin studies demonstrating that the shared environment between twins had the strongest effect on their emotional eating. 23 Additionally, young children often are not hungry when they experience strong emotions, yet some adults turn to food for comfort.43,44 As adolescents age, they may learn to cope with stress or negative emotions through emotional eating. The current study provides additional support for this theory as results indicate that emotional eating prevalence rates increased when comparing 12- to 17-year-olds.
Research and Clinical Implications
The results have clinical implications for practicing health professionals. Emotional eating on occasion likely would not be cause for concern; however, when emotional eating becomes a frequent coping mechanism, it may lead to poor physical and emotional health outcomes. Adolescents engaging in frequent emotional eating may turn to foods that are highly processed and low in nutrition. 45 As demonstrated by the current findings, adolescents with higher emotional eating had more daily frequency of energy-dense, nutrient-poor foods, junk food, and convenience food. Emotional eating can relieve feelings of sadness and anxiety, but it can also preclude healthier coping techniques and encourage escaping from emotional distress rather than distress tolerance. Health professionals can assess for emotional eating in response to sadness or anxiety and teach healthier coping skills. Furthermore, individuals with obesity reported the highest prevalence of emotional eating. Professionals in primary care and weight management clinics are encouraged to screen for emotional eating in patients with a higher weight status. A treatment to consider for all adolescents is using a parent emotion coaching model (treatment session outline and rationale available 13 ). Specifically for adolescents with overweight and obesity, the Preventing Emotional Eating Routines program has initial efficacy. 14
The current results also provide great value to researchers who would like to describe the scope of the problem in their article or grant introductions. Researchers will be better positioned to design studies and interventions if they know about how many adolescents are engaging in emotional eating. When examining an averaged emotional eating score, rates were lower than when examining endorsement of emotional eating to separate emotions. Future researchers may want to examine individual emotions to retain the nuanced differences in which emotions elicit eating for particular adolescents.
Limitations
Several limitations must be noted. First, the measure assessing emotional eating only assesses eating in response to sadness and anxiety using single items. Other important emotions including stress, shame, guilt, embarrassment, and anger are not captured. Further, eating in response to positive emotions was not assessed. Thus, the emotional eating rates may be underestimated. Moreover, emotional eating may exist on a continuum rather than as a binary construct, although there is value in describing prevalence rates. Importantly, researchers have questioned the validity of self-report questionnaires of emotional eating. 46 Researchers building nationally representative datasets in the future are strongly encouraged to include a more in-depth assessment of emotional eating that includes objective observation. Second, the study relies on reported BMI data in a trade-off to collect a larger nationally representative sample. BMI calculated from parent-reported height and weight is a significant limitation, as reported height and weight are both often inaccurate, and there are greater discrepancies in reported versus objectively measured BMI at higher BMIs. 47 To partially assuage this issue, the current study included categories of weight statuses rather than continuous BMI, as research has shown that when using reported heights and weights, adolescent weight status (underweight, healthy weight, overweight, obese weight) is more accurate than continuous BMI values. 47 Third, the FLASHE study team collapsed race/ethnicity into four response categories for the publicly available dataset which does not provide for nuanced reporting. This study was only able to compare White and Black as race categories and Hispanic as an ethnicity category. All other races and ethnicities were combined into an “Other” category. While this study did examine the rate of emotional eating for adolescents who were collapsed into this “Other” category, it is not clear who is in this group. The study team represented the US Census racial statistics from 2010 (US population: 75.8% White; 13.6% Black; US Census Bureau, 2022) such that the dataset was majority non-Hispanic White (63.8%) with 16.9% non-Hispanic Black. Future researchers are encouraged to strive for inclusive and representative samples. Fourth, the cross-sectional research design provides a snapshot of adolescent emotional eating rates but does not allow for prospective analyses. Future research should examine prospective relationships among adolescent age, weight status, and emotional eating to examine causality and temporal effects.
Conclusions
The current study establishes the prevalence of emotional eating among adolescents and highlights demographic factors associated with higher rates using data from a national survey. Thirty percent of US adolescents and 40% of parents engaged in emotional eating when sad or anxious. Adolescent emotional eating was the most prevalent in older adolescents (17-year-olds; 34.5%), females (38.8%), non-Hispanic White adolescents (31.9%), and those with higher weight status (obesity; 43.6%). Emotional eating was correlated with consuming less healthy foods, which conveys immediate and long-term health risks. Emotional eating is a common problem that practitioners can screen for and address in adolescents to reduce excess weight gain.
Impact Statement
Nearly a third of adolescents in the United States reported eating due to anxiety or sadness, with rates higher in older adolescents, girls, non-Hispanic White adolescents, and adolescents with obesity. Adolescents with more emotional eating also had more frequent consumption of energy-dense, nutrient-poor foods conferring risk for obesity.
Footnotes
Authors’ Contributions
K.M.K. https://orcid.org/0000-0001-6922-6831 CReDIT: Conceptualization, Formal Analysis, Writing—both Original Draft and Review and Editing, Supervision. M.A.M. https://orcid.org/0000-0001-8799-0665 CReDIT: Writing—both Original Draft and Review and Editing, Visualization. A.G.D https://orcid.org/0000-0001-5098-0498 CReDIT: Writing—both Original Draft and Review and Editing. J.L. Writing https://orcid.org/0009-0004-6733-7529 CReDIT: Writing—both Original Draft and Review and Editing, Visualization. A.V. ![]() CReDIT: Writing—both Original Draft and Review and Editing.
CReDIT: Writing—both Original Draft and Review and Editing.
Ethics Approval and Consent to Participate Statement
Participants completed electronic informed consent and assent. This study uses publicly available data. All study procedures received ethical approval from the National Institutes of Health (NIH) and the Westat IRB who conducted the FLASHE research study.
Availability of Data and Materials
This study uses publicly available cross-sectional survey data from the National Cancer Institute’s Family Life, Activity, Sun, Health, and Eating (FLASHE) study (National Cancer Institute, 2014; Nebeling et al., 2017). These data may be accessed from ![]() . Although this study uses an existing national dataset, the data contained in this article have not previously been reported.
. Although this study uses an existing national dataset, the data contained in this article have not previously been reported.
Funding Information
The enclosed article project received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
The authors declare that there is no conflict of interest nor competing interests.