
Abstract
Interventions in community settings, where children spend substantial out of school time, may enhance access to evidence-based lifestyle interventions. The Boys and Girls Club of Lawrence (BGCL) and New Balance Foundation Obesity Prevention Center at Boston Children’s Hospital partnered to revise, enact, and evaluate BGCL’s existing Healthy Living Club and then flexibly expand the program to increase access. The BGCL is within walking distance of three public housing communities and easily accessible to members, of whom 90% identify as Hispanic. The interventions comprised nutrition sessions and either fitness activity sessions (N+FA Cycle 1, n = 63, 26 hours; N+FA Cycle 2, n = 94, 27 hours) or academic basketball practices (N+AB Cycle 2, n = 99, 72–80 hours), leveraging time already in the schedule where fitness could be intentionally promoted by coaches. Among children aged 8–15 years, mean [95% confidence interval (CI)] changes (beginning to end) in percentage above the BMI median were significant [N+FA Cycle 1: −2.4 (−4.1, −0.8); N+FA Cycle 2: −4.3 (−5.4, −3.1); N+AB Cycle 2: −5.5 (−6.9, −4.1)]. Lifestyle interventions, implemented with flexibility in existing programs, had beneficial impact, indicating potential of community–academic partnerships.
Background
Children from low-income families, who are disproportionately affected by obesity, 1 often do not have access to prevention and treatment programs. 2 Even when referred to such programs, they face challenges in attending scheduled sessions owing to competing time demands (e.g., school, work), logistics (e.g., transportation), and priorities related to unmet social needs.3,4 Collaboration with community organizations, where at-risk children already spend substantial out of school time, is an important consideration for overcoming challenges and expanding access. 5
To foster community–academic partnerships, we developed the Boston Children’s fit kit— a set of resources with evidence-based messaging on nutrition, fitness, sedentary time, sleep, and stress—to support children (aged 8–15 years) and families in adopting healthful lifestyles (Supplementary Methods S1). During fit kit conceptualization, community organizations indicated that prearranged wellness curricula are not well received owing to lack of flexibility for tailoring content, staffing, and scheduling. Thus, by design, the fit kit is distinctively modular and flexible. As we balance flexibility with fidelity, Replicating Effective Programs (REP), from the Centers for Disease Control and Prevention, provides a useful framework.6,7
Key REP components include intervention packaging, training, technical assistance, and fidelity assessment.
6
Community organizations, in consultation with personnel from the
This report describes a partnership, between the Boys and Girls Club of Lawrence (BGCL) and OPC-BCH. In summer 2021, the two groups decided to focus collaboration on an existing Healthy Living Club (HLC) to (1) revise the nutrition component of the program using fit kit messaging and resources, (2) continue offering fitness activity sessions, and (3) update methods for impact evaluation. The BGCL successfully enacted the intervention during Cycle 1 of collaboration and then, encouraged by results of impact evaluation, expanded the program during Cycle 2.
Methods
Location
The BGCL is located in Lawrence, Massachusetts. Facilities are within walking distance of three public housing communities and thus easily accessible to more than 1900 members, of whom 90% identify as Hispanic.
Partnership
BGCL staff provided in-depth understanding of youth whom they serve, preferred strategies for program delivery, and input on survey and data collection methodologies. OPC-BCH personnel provided the fit kit, initial drafts of a nutrition program and lifestyle survey, and experience in impact evaluation.
Program Overview
For Cycle 1, BGCL staff invited children to participate in the HLC via flyers and announcements during meetings. The program included 12 nutrition sessions and 14 fitness activity sessions (N+FA, November 2021–May 2022, 60 minutes per session).
For Cycle 2, children entered via two paths, either responding to an invitation (consistent with Cycle 1) or as part of enrollment in academic basketball, a popular initiative that encourages academic success and team basketball. Regardless of entry path, the program included eight nutrition sessions (30 or 60 minutes per session, total of 6 hours), with each child participating in a fall, winter, or spring cohort. In addition to nutrition sessions, the program included either 21 fitness activity sessions (N+FA, October 2022–May 2023, 60 minutes per session) or 53–59 basketball practices (N+AB, October 2022–March 2023, 75 minutes per practice).
When expanding the program from Cycle 1 to Cycle 2, we considered available staffing and programming schedules. We leveraged effort of a part-time registered dietitian (BGCL employee) who facilitated all nutrition sessions, with support from a program assistant (teen volunteer during Cycle 1, adult employee during Cycle 2). We also leveraged time already in the schedule for basketball practices where fitness could be intentionally promoted by coaches.
Use of Boston Children’s fit kit Messaging and Resources
The dietitian used selected fit kit resources (Supplementary Methods S1) to convey nutrition messages (outlined below) and promote adherence to a low-glycemic load diet. 8 Each nutrition session included a brief lesson; recipe preparation and/or taste testing; and open discussion to foster comprehension, share reactions and preferences, and consider feasibility of applying new knowledge and skills at home.
Foundational content
Stay off the blood sugar roller coaster (Cycle 1: 2 sessions, 60 minutes per session; Cycle 2: 2 sessions, 30 minutes per session)
Main messages—nutrition
Eat “balanced” meals—follow a plate model (Cycles 1 and 2: 4 sessions, 60 minutes per session)
Eat “paired” snacks when hungry between meals (Cycle 1: 5 sessions, 60 minutes per session; Cycle 2, 1 session, 30 minutes)
Stop and think before you drink sugary beverages—drink water instead (Cycle 1: 1 session, 60 minutes; Cycle 2: 1 session, 30 minutes)
Main messages—fitness
BGCL staff and coaches encouraged exercise consistent with fit kit messages, based on public health guidelines. 9 Children could attend additional BGCL physical activity programs, as desired.
Exercise 60 minutes every day
Include at least 20–30 minutes of vigorous-intensity exercise 3 or more days per week
Data Collection
BGCL staff tracked attendance and collected data at the beginning and end of each cycle. Weight and height were measured using a calibrated digital scale (Etekcity) and stadiometer (Cycle 1: Seca; Cycle 2: Charder) to calculate BMI. The Progressive Aerobic Cardiorespiratory Endurance Run (PACER) was implemented to assess cardiorespiratory fitness. 10 A lifestyle survey, jointly developed by BGCL staff and OPC-BCH personnel using questions adapted from the Youth Risk Behavior Surveillance System, was administered electronically to assess frequency of behaviors related to nutrition and fitness.
The Institutional Review Board at Boston Children’s Hospital determined that impact evaluation was specific to existing programs and exempt from oversight.
Data Management and Statistical Analysis
OPC-BCH personnel were responsible for data management and statistical analysis. BMI was expressed as percentages above the BMI median (%BMImedian) and 95th percentile (%BMIp95) for sex and age. 11 These metrics were selected over more conventional BMIz because compression in the upper tails of the BMIz distribution compromises detection of change. 11 Mixed-model analysis of variance was applied to evaluate changes from beginning to end of each cycle, differences between N+FA and N+AB in Cycle 2 (given more contact hours for AB than FA), and changes across both cycles (including the interval between cycles) for children with repeated exposure. The Wilcoxon signed rank test was used to evaluate responses to lifestyle survey questions. Analyses were conducted using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Participant flow is presented in Supplementary Figure S1. On average (mean ± SD), participant age and contact hours were as follows: Cycle 1 N+FA (n = 63), 10.6 ± 1.1 years, 17.9 ± 4.0 hours (nutrition sessions: 8.7 ± 2.6 hours; fitness activity sessions: 9.2 ± 2.1 hours); Cycle 2 N+FA (n = 94), 10.1 ± 1.5 years, 12.8 ± 7.0 hours (nutrition sessions: 4.3 ± 1.4 hours; fitness activity sessions: 8.5 ± 7.0 hours); Cycle 2 N+AB (n = 99), 12.1 ± 1.1 years, 59.8 ± 11.5 hours (nutrition sessions: 4.4 ± 1.4 hours; basketball practices: 55.4 ± 11.1 hours).
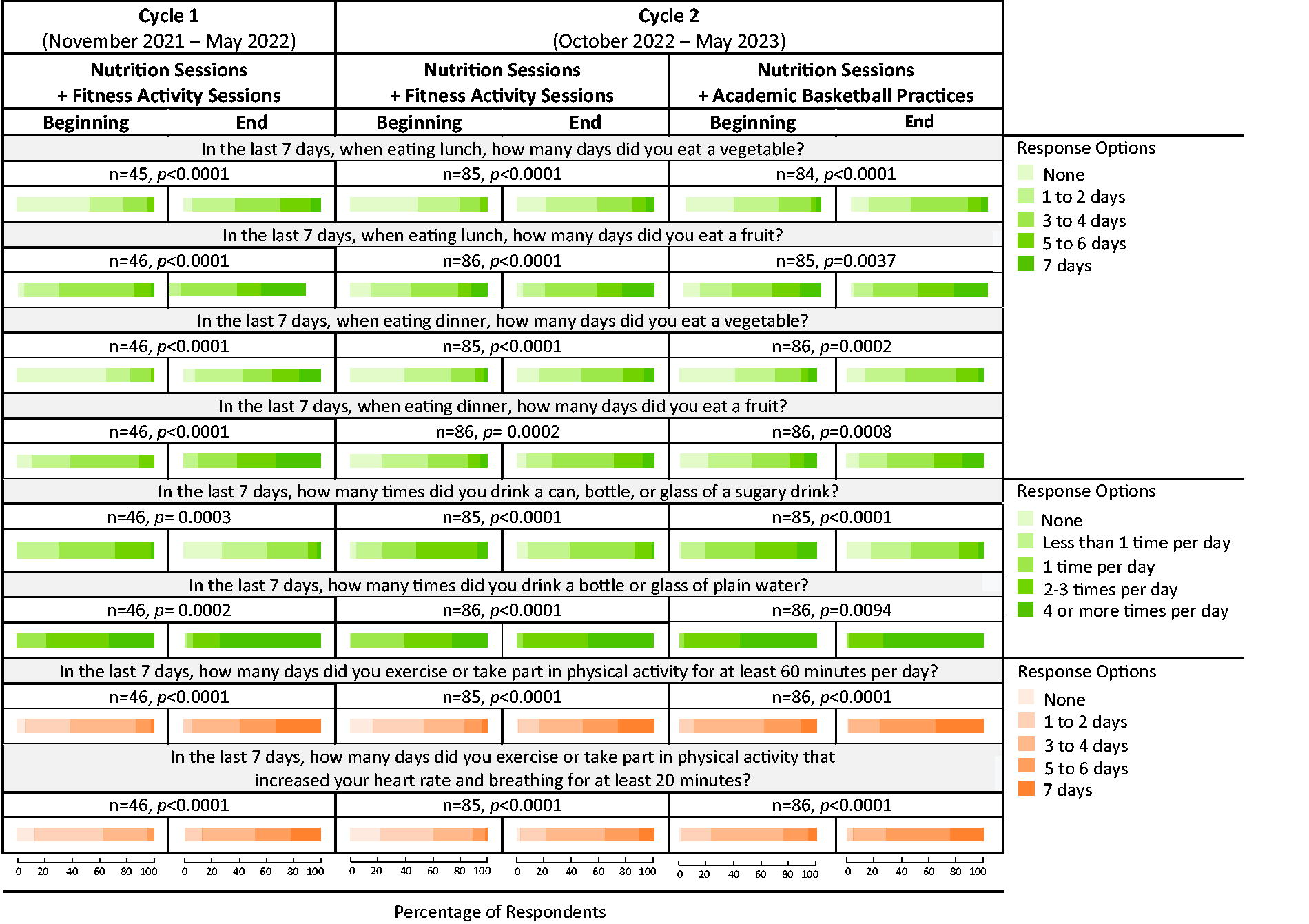
Outcomes (BMI metrics, PACER lap score) improved during each cycle (Table 1), along with changes in lifestyle behaviors related to nutrition and fitness (Fig. 1). For children with BMI ≥85th percentile at the beginning of each cycle, changes in BMI metrics were particularly notable. During Cycle 2, changes in BMI metrics did not differ significantly between N+FA and N+AB, but PACER lap score increased more with N+AB.
Change from Beginning to End of Each Cycle for BMI Metrics and PACER Lap Score
Mean (SE or 95% CI) from mixed linear model, testing the hypothesis of zero mean change (End–Beginning) using two-sided p value (unadjusted for multiplicity).
Determined from Centers for Disease Control and Prevention (CDC) growth charts. Models constructed without covariate adjustment (first row), with stratification by sex (male, female), and with adjustment for sex and stratification by beginning BMI (<85th percentile, ≥85th percentile indicating overweight or obesity). In Cycle 2, BMI metrics at the beginning did not differ between N+FA and N+AB.
Models constructed with adjustment for age and sex (first row), with adjustment for age and stratification by sex (male, female), and with adjustment for age and sex and stratification by beginning BMI (<85th percentile, ≥85th percentile indicating overweight or obesity). In Cycle 2, PACER lap score at the beginning was significantly greater for N+AB vs. N+FA, with adjustment for age and sex (p < 0.0001).
BMI, body mass index; %BMImedian, percentage above the BMI median; %BMIp95, percentage above the 95th percentile; PACER, Progressive Aerobic Cardiovascular Endurance Run.
For a subset of 33 children who participated in Cycles 1 and 2, %BMImedian decreased during Cycle 1, increased during the interval between cycles, and decreased again during Cycle 2 (Supplementary Fig. S2). For children with BMI ≥85th percentile at the beginning of Cycle 1 (n = 17), mean change in %BMImedian across cycles was −9.5 (95% CI: −15.1, −3.9).
Discussion
Changes in BMI metrics and PACER lap score indicate beneficial impact of the HLC, delivered in the context of a community–academic partnership. Improvements in BMI metrics among children with overweight or obesity compare favorably with outcomes of intensive family-based behavioral treatment in primary care, 12 interventions in community-based clinical practice settings, 13 and structured community programs for children referred by health care providers. 7 Improvements in PACER lap score compare favorably with outcomes of interventions in schools 14 and other community settings. 7
During Cycle 2, PACER lap score, but not BMI metrics, improved more for participants in N+AB vs. N+FA. Hours of basketball practice far exceeded time spent in fitness activity sessions, plausibly explaining differences. The literature indicates the potential of sports to increase physical activity and cardiorespiratory fitness but is inconclusive regarding impact on body weight, with heterogeneity across studies owing in part to diet. 15 The nutrition sessions did not differ between N+FA and N+AB, possibly contributing to similar changes in BMI metrics. However, BMI does not differentiate between changes in fat vs. fat-free mass, and results must be interpreted cautiously because participants were not randomly assigned to N+FA and N+AB.
Among children who participated in both cycles, %BMImedian decreased during each cycle with an interval of weight gain between cycles. This pattern of change, consistent with relapse observed during summer break among school children, 16 underscores the importance of ongoing intervention when treating obesity as a chronic disease. 5 Nevertheless, several children achieved clinically meaningful weight loss, based on suggested BMIz cut points of 0.7 (7 of 33 children) 17 or 0.25 (16 of 33 of children). 18
The HLC intervention was delivered pragmatically, to fit within schedules and workflows at the BGCL, and data were collected for impact evaluation. As such, this was not a controlled research study, and we cannot conclude that favorable outcomes were solely attributed to the HLC intervention. Moreover, data may not be generalizable to other community organizations, varying in geographic location and serving children with different demographic characteristics. But community–academic partnerships, using the Boston Children’s fit kit, hold promise for flexibly addressing unique needs of organizations where lifestyle interventions could help curb the childhood obesity epidemic among vulnerable groups. A future goal is to communicate with health care providers regarding progress of participants who are their patients, thereby linking these programs with clinical care, and recognizing personnel at community organizations as valued members of integrated care teams. 19
Impact Statement
At the Boys and Girls Club of Lawrence, lifestyle interventions were delivered within existing out of school programs, using resources selected from the Boston Children’s fit kit to address programming needs. BMI metrics improved significantly, indicating potential of flexible community–academic partnerships for curbing obesity among children at high socioeconomic risk for obesity.
Footnotes
Acknowledgment
The authors thank David S. Ludwig, MD, PhD for advice during preparation of the article.
Authors’ Contributions
B.R.: Conceptualization, methodology, investigation, resources, data curation, writing—original draft, visualization, and project administration. S.V.: Conceptualization, methodology, investigation, data curation, writing—review and editing, and project administration. J.H.: Conceptualization, methodology, investigation, writing—review and editing, and project administration. S.Y.: Formal analysis, data curation, writing—original draft, and visualization. D.S.: Writing—review and editing and funding acquisition. M.F.: Conceptualization, methodology, investigation, data curation, writing—review and editing, supervision, project administration, and funding acquisition. C.B.E.: Conceptualization, methodology, resources, writing—original draft, visualization, supervision, and funding acquisition.
Author Disclosure Statement
C.B.E. received grants to study a low-glycemic load diet from the National Institutes of Health (USA) and philanthropies unaffiliated with the food industry. Other authors have not stated any conflicts.
Funding Information
The
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.