
Abstract
Background:
The high prevalence of obesity in Latino families with low income necessitates prevention beginning in pregnancy and continuing through infancy. Due to systemic inequities, adverse social determinants of health (SDoH) and mental health symptoms may limit program efficacy by presenting barriers to attendance. We sought to assess: (1) the feasibility of the Starting Early Program (StEP) Prenatal, a 17-session intervention beginning early in pregnancy and continuing to 18 months postpartum; and (2) the effects of adverse SDoH (material hardship, low social support) and mental health symptoms (depression, anxiety, stress) on program attendance.
Methods:
We conducted a single-arm feasibility trial of StEP Prenatal, enrolling from December 2018 to February 2020 (n = 231). We assessed feasibility (recruitment, retention, fidelity, attendance) and direct and interactive effects of adverse SDoH and mental health symptoms on attendance. We used zero-inflated Poisson regression, adjusting for maternal age, marital status, nativity, education, and pandemic timing.
Results:
We recruited 57% of eligible participants, with 213 remaining eligible to receive the full program. Retention was 75%. Median fidelity for group format was 64%; median attendance per session was 69%; median number of program sessions attended was 13. Baseline material hardship and high perceived stress predicted approximately one additional session attended. Similar effects were seen for low social support in the absence of anxiety symptoms.
Conclusion:
Despite pandemic disruptions, StEP Prenatal was feasible to deliver and participants with adverse SDoH at baseline were particularly motivated to attend. Futures studies should tailor programs to baseline SDoH and test flexible implementation models.
Introduction
Childhood obesity is a public health crisis that disproportionately affects Latino families with low income due to historical injustices and systemic inequities affecting food, education, housing, and health care.1–4 Growth trajectories in infancy are especially consequential because they strongly predict later obesity5,6 and cardiometabolic risk,7–10 highlighting the importance of pregnancy and infancy as critical periods for obesity prevention at the system, policy, and individual level.6,11 With a team of Latino dietitians and community members, we developed the Starting Early Program (StEP). Led by bilingual/bicultural registered dietitian/certified lactation counselors (RD/CLC), this program delivered group nutrition education and parenting support in the primary care setting, culturally tailored to the Latino community. 12 Participants were recruited by bilingual/bicultural staff in the third trimester of pregnancy and offered 15 sessions until child age 3 years. The curriculum focused on breastfeeding support, responsive feeding, healthy sleep, physical activity, and general parenting. Although the StEP randomized controlled trial (RCT) showed significant beneficial impacts on behavioral and weight outcomes,12–14 analyses also revealed that socially determined but potentially modifiable risk factors for early child obesity were prevalent in pregnant participants at the time of enrollment, including poor prenatal diet quality and inadequate physical activity. 15 To begin to address these risks, we developed StEP Prenatal, an expanded prenatal version of the program, to begin in the first trimester of pregnancy and focus on maternal health more explicitly, aiming to equip families with tools useful for achieving healthy growth despite social adversity. Although scholars have recognized the first 1000 days as a critical period for both maternal and child cardiometabolic health, 16 few studies have reported on the feasibility of delivering continuous interventions spanning pregnancy and infancy. 17
In addition to the high prevalence of child obesity risk factors identified prenatally, analysis of StEP RCT data also showed a strong dose response: impacts on child weight were up to two times higher among families with high attendance compared with low attendance. 12 Subsequent analyses of these data demonstrated heterogenous effects of adverse social determinants of health (SDoH; the nonmedical factors and environmental conditions that influence health outcomes) and maternal mental health symptoms on attendance: high psychosocial stress was associated with higher attendance, and material hardship (specifically housing disrepair) was related to lower attendance. 15 Social support, a positive SDoH, is known to moderate adverse effects of stress on health behaviors and outcomes, 18 but little is known about the effects of social support on attendance in primary prevention programs and if it moderates the effects of other SDoH. StEP Prenatal was implemented in-person in prenatal and primary care beginning in fall, 2019, but all program activities were transitioned to remote delivery with the onset of the COVID-19 pandemic, creating a novel opportunity to study patterns of program attendance across both delivery modalities, and effects of SDoH and mental health symptoms during a time of particular adversity. Therefore, we sought to assess the feasibility of StEP Prenatal and to determine the effects of baseline adverse SDoH and mental health symptoms on participant attendance, including possible moderation by perceived social support. Based on our prior program and similar interventions, we hypothesized that the program would be feasible and that adverse SDoH and mental health symptoms would have heterogeneous effects on attendance.
Materials and Methods
Study Design and Setting
We conducted a single-arm feasibility trial of StEP Prenatal. The program begins in the first trimester of pregnancy and continues through child age 18 months. Supplementary Table S1 displays the intended content and format (individual vs. group) of the 8 prenatal and 9 parenting sessions. Sessions were delivered by bilingual RD/CLCs, who prioritized content delivery over fidelity to group format when feasible. Therefore, before the pandemic, if participants could not attend a prenatal group session, the content was delivered individually the next time they were in clinic. If participants could not attend a parenting group session, the content was only delivered individually if they were available in the clinic the same day. Program interventionists were always available to participants by text, email, and phone to address unanswered questions and direct participants to appropriate resources.
Participants
We screened all patients scheduled for a first prenatal appointment at a large, academic hospital-based obstetrics clinic in New York City and enrolled those who were in the first trimester, identified as Hispanic/Latina, fluent in English or Spanish, and intended to receive care at the study site. We excluded participants with severe medical or mental illness (e.g., untreated psychosis), homelessness, younger than 18 years, or uncertainty of last menstrual period. The New York University Grossman School of Medicine and New York City Health + Hospitals Institutional Review Boards approved this study and it was registered on clinicaltrials.gov (NCT01541761).
Remote Adaptation
StEP Prenatal procedures and content were adapted for remote delivery beginning in March, 2020, with the onset of the COVID-19 pandemic. From this point forward, we allowed sessions to be scheduled on days distinct from primary care visits to allow for additional flexibility. For the first 3 months of the pandemic, all session content was delivered via individual phone calls. Beginning in June 2020, we resumed group sessions remotely using videoconference software. Beginning in August 2020, individual sessions were allowed to resume in-person (group sessions were remote for the remainder of the program). Using videoconference software, we were able to maintain much of the program content with few changes. We adapted the active practicing of skills to accommodate remote delivery by instructing participants to use items and spaces available in their homes. For example, we asked participants to share food labels from their own pantries rather than providing precut labels. Similar to prepandemic, we prioritized content delivery over fidelity to group format when feasible. There was no limit to the number of scheduling attempts study staff made and a session was not considered “missed” until the target date for the subsequent session was reached.
Measures
Feasibility
We assessed four domains of feasibility, using relevant portions of the RE-AIM framework (Reach, Efficacy, Adoption, Implementation, Maintenance)19,20 and prior studies of prenatal21,22 and family-based preventive interventions.23,24 Domains and measures included recruitment (Reach), retention (Adoption), fidelity (Implementation), and attendance (Adoption), as defined in Table 1. To assess factors associated with attendance, we calculated the number of missed sessions for each participant (17 minus number of sessions attended) to be used as the dependent variable, as this had a frequency distribution that could be fit with a multivariable model (see the Statistical Analysis section).
Definitions and Descriptive Statistics for Feasibility Measures by RE-AIM Domain and Level of Analysis
The RE-AIM (Reach, Efficacy, Adoption, Implementation, Maintenance) framework organizes feasibility measures into relevant domains. Efficacy and Maintenance were outside the scope of this study.
IQR, interquartile range.
Adverse SDoH
We analyzed two adverse SDoH measured at baseline as predictors of attendance. Material hardship was a composite variable representing the presence of one or more of the following: food insecurity (measured by the 10-item core food security module) 25 ; housing disrepair (measured using an item from the Survey of Income and Program Participation [SIPP]) 26 ; unsafe neighborhood (measured using an item from the Pregnancy Risk Assessment Monitoring System) 27 ; and financial difficulty (measured using two items from the SIPP). 26 Social support was assessed using the Medical Outcomes Study Social Support Scale and classified as low if the overall score fell in the bottom quartile. 28
Mental health symptoms
We measured symptoms of depression using the Patient Health Questionnaire 9 (PHQ9) and symptoms of anxiety using the Generalized Anxiety Disorder 7-item screener, with a score of 5 or greater classified as positive.29,30 We measured perceived stress using the Perceived Stress Scale and classified participants with a score of 14 or greater as positive. 31 We referred participants with a PHQ9 score of 10 or above or suicidality to the clinic social worker.
Covariates
We used baseline demographic data, as reported by the study participant, for age, marital status, nativity, and education. We used time from study enrollment to March 7, 2020 (date of the New York State public health emergency declaration), as an additional covariate to account for duration of exposure to the pandemic.
Statistical Analysis
We used descriptive statistics to assess recruitment, retention, fidelity, and attendance. We used zero-inflated Poisson regression to assess predictors of attendance, based on the frequency distribution of program dose (Fig. 2). This generated incidence rate ratios of missed sessions in five separate models as follows: (1) material hardship; (2) low social support; (3) depression; (4) anxiety; and (5) stress. For each model, we estimated absolute number of sessions attended in the presence or absence of the predictor of interest, with covariate values at their means. We tested moderation by social support by including a social support interaction term with each predictor of interest in models 1, 3, 4, and 5.
Results
Study Sample
Table 2 shows baseline characteristics for 213 participants. The majority of participants were born outside of the United States (73.2%), and experienced at least one material hardship (68.5%). High perceived stress was present for 83.3% of the sample and low social support was present for 25.4% of the sample. Mental health symptoms were common, with 42.1% and 30.6% screening positive symptoms of depression and anxiety, respectively.
Baseline Characteristics of 213 Latina Participants, Enrolled in an Early Child Obesity Prevention Program Beginning in the First Trimester of Pregnancy
n = 209.
n = 156, question only asked to those born outside the United States.
n = 207.
n = 210.
Overweight/obesity defined as body mass index ≥25.
Type 2 diabetes mellitus: n = 4; gestational diabetes mellitus: n = 14.
n = 208.
Score of 14 or greater on the Perceived Stress Scale.
Medical Outcomes Study Social Support Scale score in the bottom quartile.
Score of 5 or greater on the Patient Health Questionnaire 9.
Score of 5 or greater on the Generalized Anxiety Disorder 7-item screener.
Feasibility
We screened 1405 individuals for eligibility between December 2018 and February 2020 and 421 were found to be potentially eligible to participate. Of those, 238 signed consent, resulting in a recruitment rate of 57%. There were 24 pregnancy losses and one participant developed severe mental illness in pregnancy, resulting in 213 participants eligible to receive the full 17-session program (Fig. 1). Seventy-five percent of participants completed at least one session in the second year of life and 74% of participants completed the final survey. We completed data collection after the final 18-month session, on 4/8/2022.
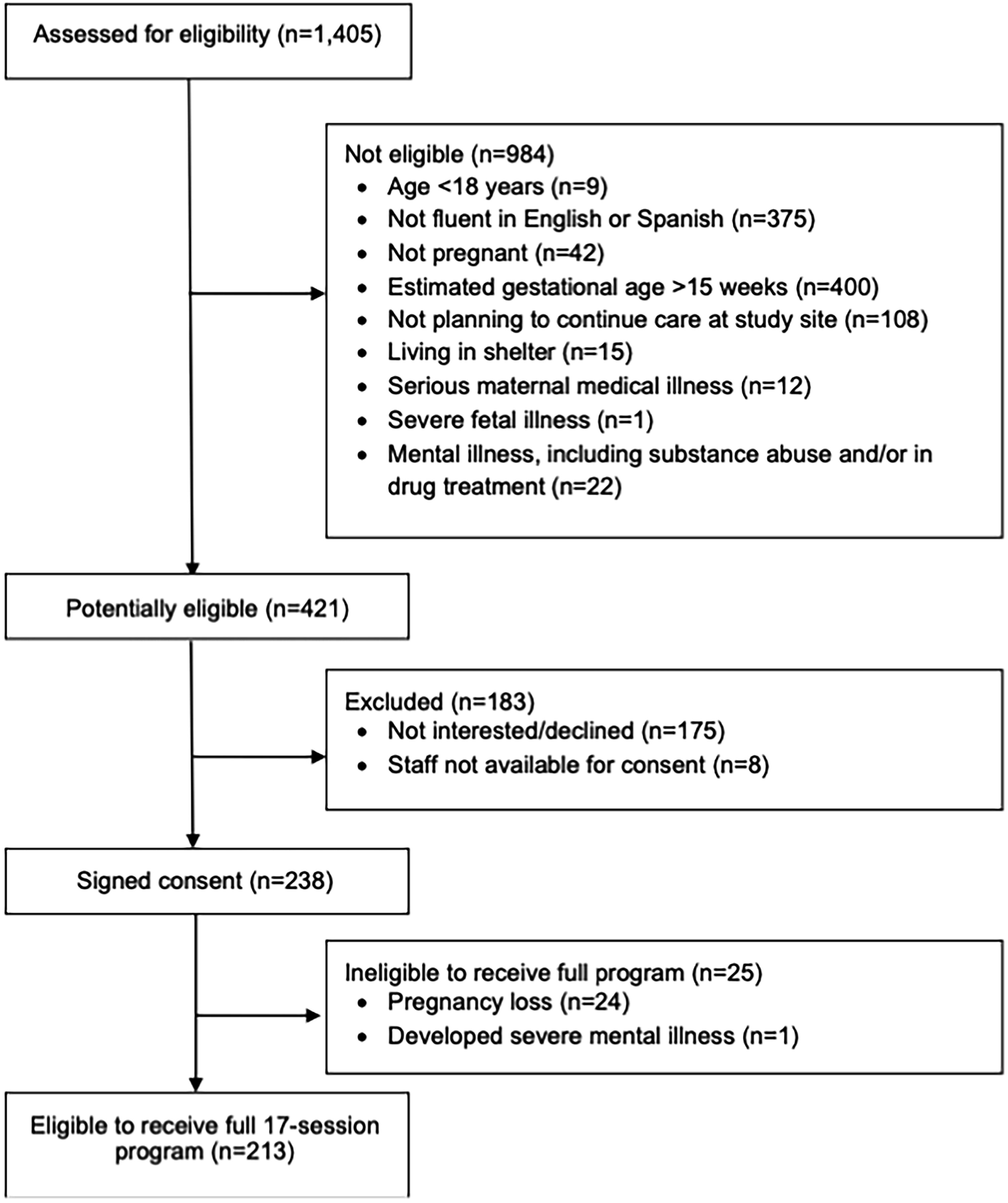
StEP Prenatal CONSORT diagram.
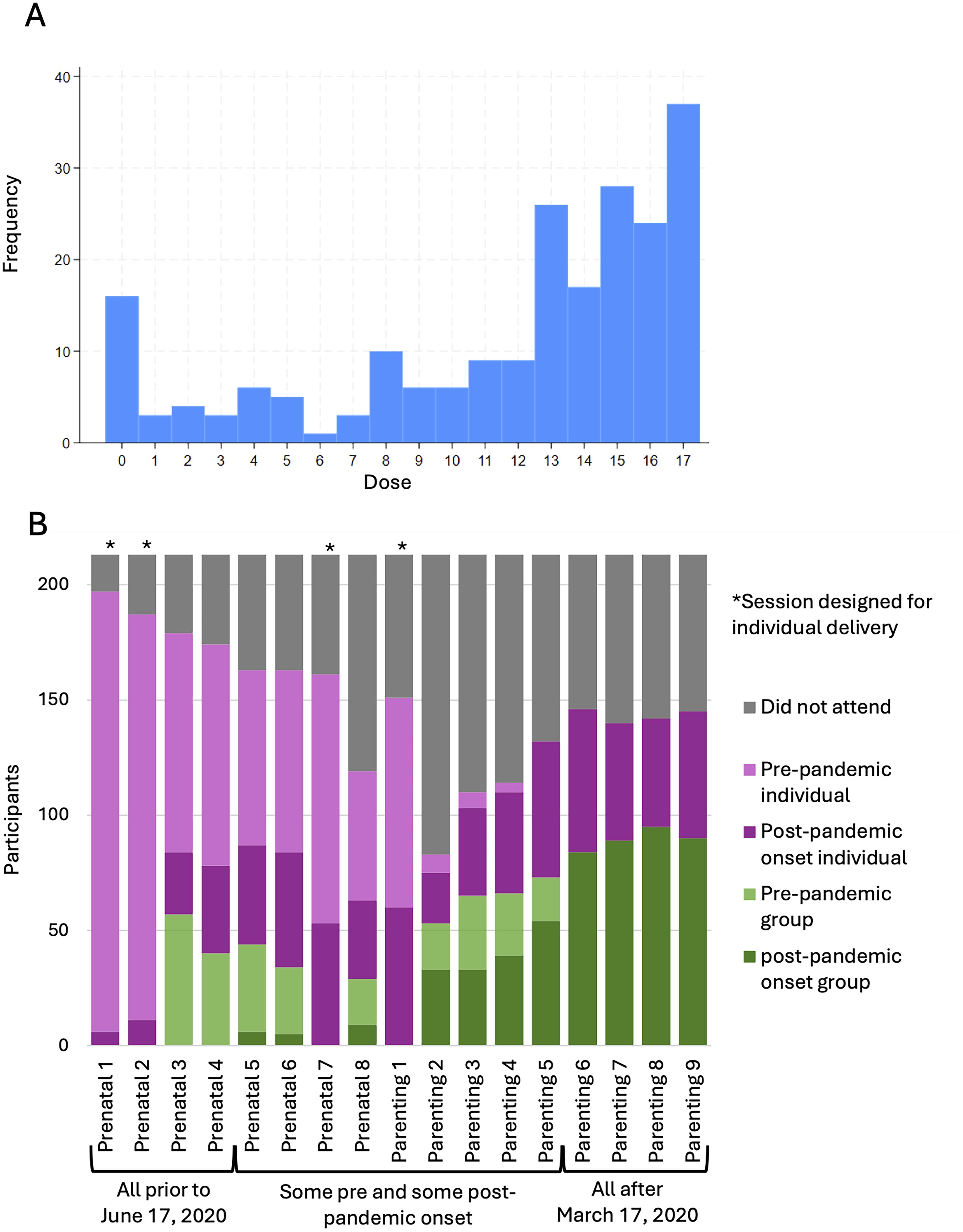
Panel A. Frequency distribution of number of program sessions attended. Program dose was defined as total number of sessions attended by each individual. Note that multivariable analyses used the inverse of dose (i.e., number of missed sessions) as the dependent variable to fit a zero-inflated Poisson regression model.
Fidelity and attendance are displayed in Figure 2. Due to the COVID-19 pandemic, group sessions were not available between March 17 and June 16, 2020. Median fidelity to group format outside of this 3-month period was 64% across all 13 sessions designed for group delivery. Median fidelity to group format for prenatal sessions was 24%, which was lower than median fidelity to group format for parenting sessions, which was 60%. Median fidelity to group format was lower before March 17, when all groups were offered in person (38%), than it was after June 16, when all groups were offered remotely (62%). Across all 17 program sessions, median attendance was 69%. Median attendance for prenatal sessions (79%) was higher than median attendance for parenting sessions (66%). Median attendance prepandemic (76%) was similar to median attendance postpandemic onset (68%). In general, sessions with higher attendance had lower fidelity to group format, and sessions with lower attendance had higher fidelity to group format. Across all 213 participants, median program dose was 13 sessions.
Associations Between SDoH, Mental Health Symptoms, and Attendance
Associations between adverse SDoH, mental health symptoms, and attendance are shown in Table 3. The baseline estimated program dose was 12.00 (95% CI 11.6, 12.4) with only covariates in the model. Having any material hardship was significantly associated with a 14% higher dose than having no material hardships (incident rate ratio [IRR] 0.86, p = 0.02). When tested individually, housing disrepair was the only material hardship significantly associated with dose (IRR 0.82, p < 0.01). High perceived stress was significantly associated with an 18% higher dose than low stress (IRR 0.82, p = 0.02). Low social support, depression, and anxiety symptoms were not significantly associated with dose.
Associations Between Adverse Social Determinants of Health, Mental Health Symptoms, and Number of Program Sessions Attended, Tested in Separate, Adjusted Zero-Inflated Poisson Models
Estimates represent IRR of missed sessions for each variable tested in separate models, adjusting for maternal age, marital status, nativity, education, and time from study enrollment to March 7, 2020 (declaration of COVID-19 public health emergency in New York State).
Model predictions made with all other variable values at their means. Bolded text represents statistical significance at the P<0.05 level.
IRR, incident rate ratio; SDoH, Social Determinants of Health.
Results of the four main interaction models are shown in Table 4. For each model, reference categories were chosen to represent the ideal conditions of the combined interaction, that is, absence of adverse SDoH and mental health symptoms, and significance was assessed for each of the other three possible conditions with respect to that reference. Material hardship, perceived stress, and anxiety all had statistically significant interactions with social support in predicting dose. Those with material hardship and high social support attended more sessions than those with no hardship and high social support (IRR 0.83, p = 0.02). Those with high stress and low social support attended more sessions than those with low stress and high social support (IRR 0.80, p = 0.04). Those with no anxiety and low social support attended more sessions than those with no anxiety and high social support (IRR 0.77, p = 0.01).
Social Support as a Moderator of the Effects of Perceived Stress, Material Hardship, and Mental Health Symptoms on Dose, Tested in Separate, Adjusted Zero-Inflated Poisson Regression Models
Estimates represent IRR of missed sessions for each variable tested in separate models, adjusting for maternal age, marital status, nativity, education, and time from study enrollment to March 7, 2020 (declaration of COVID-19 public health emergency in New York State).
Model predictions made with all other variable values at their means.
Discussion
This analysis shows that an early child obesity prevention program for Latino families with low income, beginning in the first trimester of pregnancy, is feasible, even when interrupted by the COVID-19 pandemic. Results also show that SDoH and mental health symptoms at baseline significantly predict program attendance from that point through the first 18 months postpartum. Specifically, experiences of material hardship or high perceived stress, and experiences of low social support without anxiety symptoms were associated with higher attendance. This suggests that a program designed to support healthy habits in prenatal and infant nutrition and feeding may also address psychosocial stress and lack of social support, expanding on our current understanding of the drivers of attendance in early prevention programs.
Few individual- or family-level prevention programs aimed at improving child health outcomes begin early in pregnancy and continue past the child’s first year of life, 32 despite the well-recognized importance of this stage in the life course for maternal and child health outcomes. 33 Many programs that do begin early in pregnancy focus solely on maternal health outcomes, 21 while those that aim to prevent adverse child health outcomes generally begin after the baby is born.34–37 This article is the first, to our knowledge, to demonstrate the feasibility of an intervention that spans all trimesters of pregnancy and the first 18 months of infancy. Recruitment early in pregnancy is challenging, and our recruitment rate of 57% can be compared with reported recruitment rates of 25%–33% for similar interventions.21,22 Our 75% retention rate and 69% median attendance rate are also comparable with other behavioral interventions in pregnancy,24,38 although these measures are difficult to compare across studies, and are often not defined or reported at all.
Our fidelity and attendance results should also be interpreted in the context of program-specific details. Prenatal Session 8, for example, which had relatively low attendance, is designed to occur between 36 and 40 weeks of estimated gestational age, but the actual window for content delivery is brief in many healthy pregnancies that deliver at 37 or 38 weeks. Apart from Prenatal Session 8, prenatal sessions had a higher overall attendance and lower fidelity to group format compared with parenting sessions. This may reflect the overall higher frequency of planned trips to prenatal clinic, compared with pediatric clinic, which resulted in more opportunities for individual “makeup” sessions if participants missed group sessions. With the onset of the pandemic, remote delivery enabled more flexible scheduling for “make-up” sessions, as there was no longer a need to align program sessions with a scheduled clinic visit. Remote delivery also may have facilitated fidelity to group format by easing scheduling difficulties. The inverse association between each session’s attendance rate and fidelity to group format rate likely reflect practical trade-offs that occur when staff resources are limited.
In general, specific determinants of preventive program attendance and intervention dose remain poorly understood, and our findings shed some light on this issue.38,39 Our analyses show that higher stress and presence of material hardship are associated with higher program dose, but social support and anxiety, when considered alone, are not. Our interaction models show that social support and anxiety are significantly associated with dose in certain situations, but the effect-size differences between conditions are quite small. Taken all together, the findings suggest that the presence of adverse psychosocial conditions may have motivated attendance in the program. While this contrasts with findings of some studies, 40 others, including our prior analysis of the StEP RCT, have shown some forms of adversity to be associated with better attendance. 15 It is likely that the benefits of participation in some programs are large enough to overcome the barriers presented by some adverse conditions, or that these programs address the practical and psychological barriers directly. 41 StEP Prenatal may have done both by building social connections and offering knowledge and skills that served to reduce stress. Our finding that housing disrepair was significantly associated with higher program dose directly contrasts with finding in our original cohort, 15 so this will need to be clarified in future studies, as will the minimum necessary dose of preventive interventions.
It is also important to note some study limitations, including unmeasured variations in program implementation over the course of the early pandemic, when crisis-prompted adaptations occurred in real time. It was also impossible to determine how decoupling of our program sessions from primary care visits affected primary care visit attendance, because this occurred simultaneously with the pandemic onset, which brought with it numerous other challenges to primary care delivery. However, we believe these to be outweighed by several important strengths, including our focus on a high-risk demographic group, our detailed measures of psychosocial adversity, and our use of the COVID-19 pandemic as an opportunity to examine program attendance patterns across in-person and remote modalities. As one of the only programs to deliver a continuous intervention across pregnancy and infancy, our program has the additional advantage of reaching families during the preconception period (i.e., infancy of one child is preconception period for the next), when preventive interventions are likely to have the biggest effect on long-term health outcomes. 42 Our relatively high rates of recruitment, retention, and program attendance in this population support the value of this model.
Conclusions
This study suggests that early child obesity prevention programming, tailored to Latino families with low income, beginning in the first trimester of pregnancy, is not only feasible to deliver in-person and remotely, but particularly desirable for families experiencing material hardship, psychosocial stress, and low social support. Future randomized controlled trials designed to compare different modalities and formats will be necessary to determine optimal program structure, and should include more detailed measures of program engagement to elucidate mechanisms of program effects. To address child obesity at a population level, it will be critical for programs at the individual and family level to consider flexible delivery models and adaptations tailored to baseline SDoH and mental health symptoms, and for programs at the system and policy level to target systemic inequities that contribute to nutrition-related health disparities in the first place.43–46
Impact Statement
The high prevalence of obesity in Latino families with low income necessitates prevention interventions throughout pregnancy and childhood; however, few programs offer this continuity. StEP Prenatal spans pregnancy and infancy, was feasible to deliver to Latino families with low income, and was well attended, particularly by families with social adversity.
Footnotes
Acknowledgments
We thank Stephanie Gonzalez, Fabiola Gomez, Cristina Vasquez, Paola Duarte, Sophia Jan, and the pediatric and prenatal staff at Bellevue Hospital.
Authors’ Contributions
M.K.: Conceptualization, data curation, formal analysis, funding acquisition, visualization, writing—original draft, and writing—review and editing. R.G. and M.J.M.: Conceptualization, funding acquisition, methodology, resources, supervision, project administration, and writing—review and editing. J.B.: Data curation, investigation, and writing—review and editing. C.K.: Data curation, project administration, supervision, and writing—review and editing. C.D.-L. and A.M.: Writing—review and editing. C.D.: Conceptualization, methodology, and writing—review and editing. M.S.: Supervision, formal analysis, and writing—review and editing.
Funding Information
This work was supported by the
Author Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.