
Abstract
Background:
Examining sedentary time (ST) by disaggregating the day into periods such as before, during, and after preschool allows interventionists to understand when sedentary behaviors are most severe. This study aimed to determine if there are sex differences in ST before, during, and after preschool hours in US preschoolers.
Methods:
A secondary analysis of a two-cohort study with a sample size of 292 preschoolers (67% African Americans/Blacks; 100% from low-income families) was used. Measures were collected in Fall 2017 and Fall 2018. Preschoolers wore an accelerometer on the non-dominant wrist for 8 consecutive days to obtain ST minutes before, during, and after preschool periods. Three separate linear regressions were conducted to test sex differences in ST before, during, and after preschool hours. ST for each period of the day was considered the outcome variable predicted by sex and covarying for BMI percentile.
Results:
Girls were more sedentary than boys during preschool (F (1, 226) = 5.15, p = 0.006; b = −0.09 [−0.15, −0.03]), but not before preschool (F(1, 225) = 0.98, p = 0.32; b = 2.50 [−2.46, 7.45]) nor after preschool (F(1, 227) = 3.62, p = 0.06; b = 6.60 [−0.21, 13.42]).
Conclusions:
This difference in ST could have an unfavorable health impact among preschool girls. Given that childhood obesity prevalence dramatically increases from preschool age to childhood, there is a need to design family-based interventions that provide parents/caregivers strategies to develop habits around healthy eating and physical activity that they can carry into later life stages.
Introduction
Multiple initiatives exist for preschoolers (3–5 years) to reduce sedentary time (ST), or time spent sitting, reclining, or lying down during waking hours that requires an energy expenditure ≤1.5 metabolic equivalent of the task (METs). 1 Recent trends also show that United States preschoolers engage in 31.1 2 to 46.1 3 minutes of ST per hour. The World Health Organization (2019) 4 recommends that children in this age group spend a maximum of one hour at a time being restrained (e.g., being in a pram or stroller) or sitting and avoid sedentary screen time as much as possible.
Although the ST recommendations are the same for male and female preschoolers, sex disparities are observed in ST. Literature has consistently shown that female preschoolers,5,6 children, 7 and adolescents 7 are more likely to be sedentary than males. In preschoolers, recent cross-sectional data reported that preschool girls spend an average time of 493.6 min/day in ST compared to boys who spend an average of 480 min/day in ST. 6 Similarly, cross-sectional data have shown that 4-to-5-year-old girls spend 331.6 min/day in ST compared to boys who spend 327.1 min/day in ST. 7 It is worrisome how sex disparities are present at an early age since research also supports that adopting healthy habits early in life can contribute to better health outcomes during adulthood. 8 Additionally, it is known that in the United States, ST is closely related to obesity during adolescence. 9 For instance, the ISCOLE study, which recruited 9-to-11-year-old participants to test the relationship between ST and obesity, reported that ST is directly related to obesity. 9 Thus, examining sex disparities in ST early in life is vital because ST can affect long-term health outcomes.
While researchers have gained valuable knowledge on which group is more likely to have higher ST levels across the entire day (min/day or h/day), less is known about the time of day when sex disparities are the most salient. Disaggregating the day into periods such as before, during, and after preschool could provide useful information. We believe that in the US examining these three periods makes sense since 59% of the 3-to-5-year-old children attended preschool in 2022. 10 Thus, most US preschoolers tend to have similar timeframe structure during the weekdays. Knowing which period of the day (before, during, and after preschool) drives the overall ST disparity allow interventionists, teachers, preschool administration, and parents to indirectly understand under who’s supervision (parents vs teachers) ST disparities are occurring and potentially address those periods to help reduce sex disparities in ST. For example, Hesketh et al. investigated during and out of preschool (i.e., before and after preschool) device-based ST patterns among 3- to 4-year-old British children. 11 The authors reported that boys accumulated less ST during the afternoon (3:00 p.m. to 6:00 p.m.) than girls. 11 Even though the authors defined the periods of the day they examined, they did not provide results during preschool (9:00 a.m. to 3:00 p.m.). A lack of information about the preschool period is limiting, as merging periods of the day prohibits the ability to determine if sex disparities in ST are occurring during preschool time.
Similarly, another British study used accelerometers to explore how ST patterns vary across the day in 4-year-old children. 12 Investigators reported that girls accumulated more ST in the mornings (6:00 a.m. to 12:00 p.m.), but not during the afternoon (12:00 p.m. to 5:00 p.m.) or evening (5:00 p.m. to 11:00 p.m.), compared to boys. 12 Authors reported that being a girl was associated with a 6.3-minute increase in ST during the morning. 12 Although great insight into sex disparities in ST among British children is provided, little is known about sex disparities in ST among US preschoolers, which limits the ability to apply this knowledge since we do not know if sex disparities in ST are manifested similarly across populations.
Despite current literature supporting sex disparities in ST, some gaps in the literature remain. First, timeframes for each period of the day should be well-defined and not merged to determine when ST disparities by sex are happening accurately. Second, data about ST during each period should be provided. Lastly, to our knowledge, only studies outside the United States have analyzed ST data by period of the day among preschoolers. Thus, this study aimed to determine if there are sex differences in ST before, during, and after preschool hours among a sample of US preschoolers. Based on the literature, it was hypothesized that girls will be more sedentary than boys during preschool (8:30 a.m. to 3:20 p.m./3:30 p.m.) and after preschool (3:21 p.m./3:31 p.m. to 8:45 p.m.) hours, but not before preschool (5:55 a.m. to 8:29 a.m.). We believe this since studies have reported that preschool boys are less sedentary during preschool 9 and after preschool 11 hours compared to preschool girls. Additionally, during preschool time, it is known that girls tend to have better self-regulation skills compared to preschool boys. 13 This can be translated into the classroom as preschool girls spending longer periods completing their tasks, which usually involve coloring, completing puzzles, and crafting, among other activities that involve sitting to facilitate teachers’ classroom management. We anticipate preschoolers will have similar routines before preschool hours, regardless of sex.
Materials and Methods
Study Design
This study was a secondary analysis of baseline data from a federally funded project (R01HL132979) that examined the effects of a motor skill intervention (CHAMP) on preschoolers’ physical activity, motor competence, and perceived physical competence. The protocol paper provides a detailed description of the project’s aims and procedures. 14 The study was approved and overseen by the University of Michigan IRB (HUM00133319). We contend that this secondary analysis is appropriate for answering our research question and allows us to comply with the NIH guiding principles of ethical research. 15 Particularly, this article addresses the social and clinical value principle by avoiding participants’ exposure to possible harms associated with the research study and time burden. 15 Parents/guardians completed a written informed consent, and children provided verbal assent before study enrollment.
Study Sample, Recruitment and Preschool Environments
The PATH study was a 2-cohort randomized control trial. Children from three Head Start centers in a small city in the Midwest were invited to participate. All children who were enrolled in the centers in the Fall of 2017 and Fall of 2018, were 3.5 years or older, and had no documented physical or learning disability were eligible to participate. In total, 303 children were enrolled in the study, but two were deemed ineligible due to incorrectly reported age or previously undisclosed failure to meet inclusion criteria and two withdrew before data collection. Thus, the final enrollment was 299 children.
All children had access to large indoor (gymnasium or multi-purpose room) and outdoor play spaces to support movement and gross motor development. A full description of the playgrounds, including schematics, has been published elsewhere. 16 All playgrounds included large play equipment (e.g., slides, climbing jungle gyms, swings) and open grassy areas. Two playgrounds also included a large blacktop area with a basketball hoop and the other included a bike path. Teachers at the schools had access to a few additional elements (e.g., balls or bean bags), and adding those elements was at the discretion of the classroom teachers.
Measures
Measures were collected depending on the year of enrollment (Fall 2017 or Fall 2018). Demographic variables such as age, sex, and race/ethnicity were parent-reported. Trained data collectors assessed height and weight to calculate body mass index (BMI) percentile. ST was obtained through accelerometry and reported in minutes per period of the day (e.g., minutes before preschool, minutes during preschool, and minutes after preschool; see below). Preschoolers were instructed to wear a GT3X+ ActiGraph accelerometer on their non-dominant wrist at all times (including showering or bathing) for eight consecutive days. No data collection occurred during the first day; thus, a full seven days of wear time were expected. Research staff performed the initial device placement and conducted daily checks during preschool days to identify preschoolers not wearing the device. Additionally, the research team adopted strategies to guarantee adherence and correct placement of the accelerometer. These included (1) a letter to parents explaining the device placement through a simple diagram, (2) putting stickers on the accelerometer to indicate correct placement, (3) reminders via text messages, phone calls, and flyers, and (4) an incentive gift card on the return of the device.
The ActiLife (Pensacola, FL) Software was used for accelerometer initialization, data downloading, and processing. Table 1 summarizes the accelerometer initialization parameters and data processing. The periods were defined as before (5:55 a.m.–8:29 a.m.), during (8:30 a.m.–3:20 p.m. or 8:30 a.m.–3:30 p.m.), and after preschool (3:21 p.m.–8:45 p.m. or 3:31 p.m.–8:45 p.m.). These periods were based on US preschooler data from Williamson et al. 18 and on the preschool center schedules that were enrolled in the study. It was reported that US preschoolers’ mean bedtime is 9:45 p.m., and the nighttime sleep duration is 9 hours and 10 minutes 18 resulting in an anticipated wake-up of 5:55 a.m. The during preschool period was defined as the time they were attending preschool, and it was based on the schedule of the preschoolers in this study. For some participants, it was between 8:30 a.m. and 3:20 p.m., and for others it was between 8:30 a.m. and 3:30 p.m. After preschool period was defined as the time between preschool ends (3:21 p.m./3:31 p.m.) and bedtime (9:45 p.m.).
Parameters and Descriptions of Accelerometer’s Initialization, Data Download and Processing
Johansson et al. 17
ST, sedentary time.
Statistical Analyses
Only participants that did not have any accelerometer data and that did not meet the wear time parameters were excluded from the analyses. Descriptive statistics were conducted for all continuous variables (ST before preschool, ST during preschool, ST after preschool, BMI percentile, and age), and frequencies were obtained for all categorical variables (sex and race/ethnicity). To test for sex differences in ST before, during, and after preschool hours, three separate linear regressions were fitted. For each linear regression model, ST for each period of the day (before, during, and after preschool) was considered the outcome variable as predicted by sex and adjusting for BMI percentile. ST weekly and monthly differences in minutes/period were calculated only if the adjusted regression model was significant. Linear regression assumptions such as normality, multicollinearity, homoscedasticity, autocorrelation, and linearity were verified. Variables that were not normally distributed (kurtosis exceeding ±3 or skewness exceeding ±1) 19 were transformed to achieve normality. Only minutes of ST during preschool were natural log-transformed. All analyses were conducted in Winter 2023 using SAS 9.4.
Results
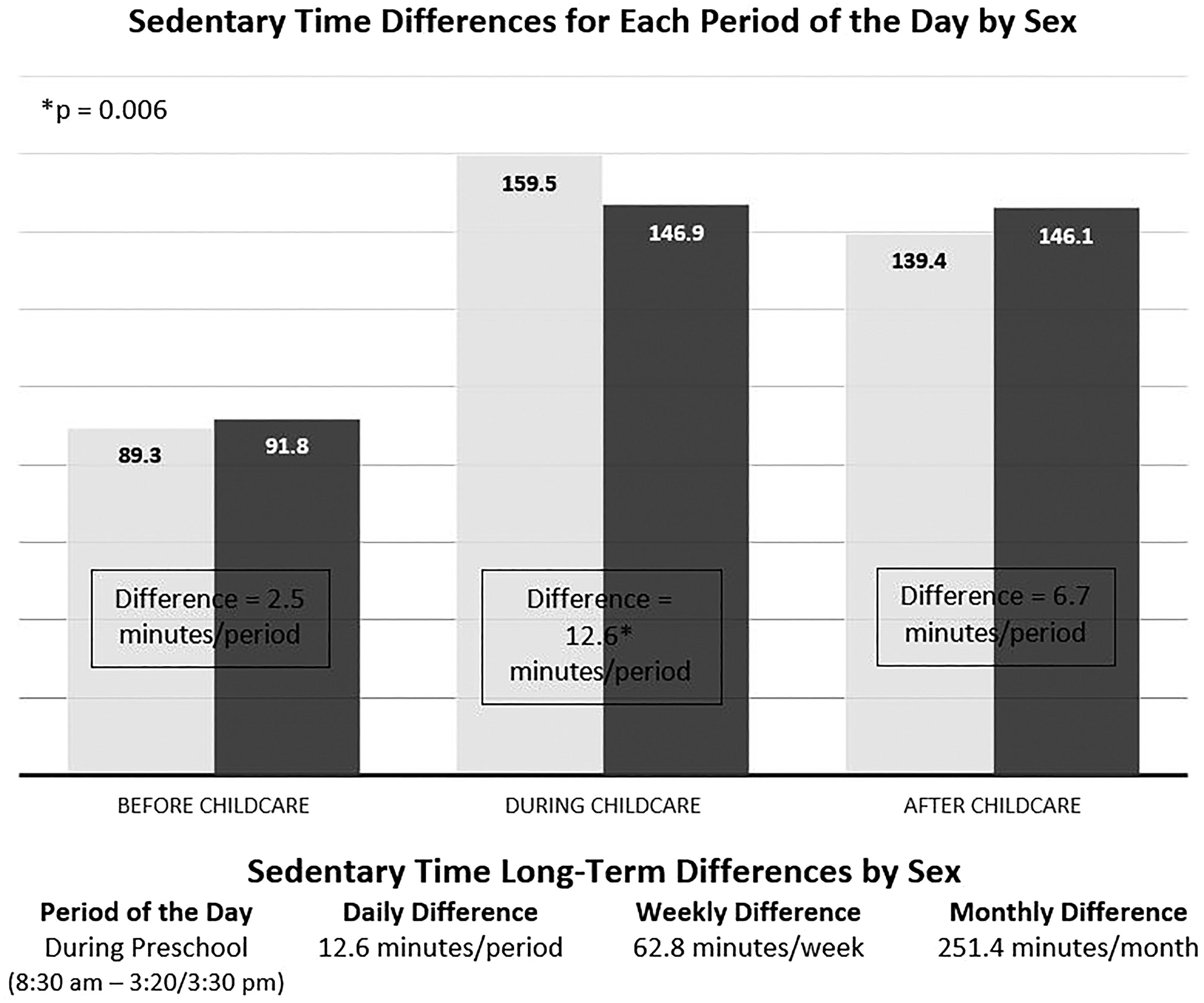
The original sample consisted of 299 preschool girls (mean age = 52.8 ± 3.6 months) and boys (mean age = 53.4 ± 3.9 months). However, seven participants did not have any data available. Thus, the final sample consisted of 292 preschoolers (girls: 155, boys: 137); most identified as African American/Black (African American/Black: 67.1%, White: 14.1%, Hispanic/Latino: 4.3%, Other: 2.9%, Asian: 0.4%, no response: 11.2%). Sixty-three participants did not have accelerometer data (i.e., missing data: n = 34, not meeting wear time validation criteria: n = 29). The remaining 229 preschoolers with accelerometer data accumulated an average of 6.5 hours/day of ST (girls: 6.5 ± 0.9 vs. boys: 6.4 ± 0.9 h/day), 90.5 minutes of ST before preschool (girls: 89.3 ± 19.7 vs. boys: 91.8 ± 18.3 min/period), 153.3 minutes of ST during preschool (girls: 159.5 ± 33.7 vs. boys: 146.9 ± 36.4 min/period), and 142.7 minutes of ST after preschool hours (girls: 139.4 ± 27.2 vs. boys: 146.1 ± 25.5 min/period). All 292 participants had data for age, and 248 participants had BMI percentile data. On average, participants had a mean BMI percentile of 66.2% (girls: 68.2 ± 26.5% vs boys: 63.9 ± 29.6%). The sample consisted of 4 participants classified as underweight (3 boys), 166 (74 boys) healthy weight, 43 (21 boys) overweight, and 35 (15 boys) obese.
The unadjusted linear regression analyses showed that sex was a significant predictor of ST during preschool (F(1, 230) = 9.82, p = 0.002; b = −0.09 [−0.15, −0.03]) but not of ST before (F(1, 225) = 0.98, p = 0.32; b = 2.50 [−2.46, 7.45]) nor after preschool (F(1, 227) = 3.62, p = 0.06; b = 6.60 [−0.21, 13.42]) periods. The adjusted linear regression model showed that sex remained a significant predictor of ST during preschool hours (F (1, 226) = 5.15, p = 0.006; b = −0.09 [−0.15, −0.03]). Therefore, it appears that girls were more sedentary than boys during preschool hours after adjusting for BMI percentile. Table 2 summarizes details about the unadjusted and adjusted models. ST differences by sex for each period of the day are presented in Figure 1.
Regressions of Sedentary Time by Periods of the Day on Sex
Unadjusted models only included sex into the model. Adjusted models included sex and body mass index in the model only if the unadjusted model was significant.
Discussion
To our knowledge, it is the first study in the United States to analyze preschoolers’ ST data by period of the day. The study aimed to determine if there are sex differences in ST before, during, and after preschool hours in US preschoolers. It was hypothesized that girls would be more sedentary than boys during preschool and after preschool hours, but not before preschool hours. Findings showed that girls were more sedentary than boys only during preschool, but not before and after preschool hours. The sex difference in ST during preschool was 12.6 minutes/day. Even though a small difference, it still has an unfavorable health impact among preschoolers. For instance, an isotemporal substitution analysis showed that substituting 5 minutes of ST with five minutes of vigorous physical activity is associated with a 0.2 increase in fat-free mass index in preschoolers. 20 Therefore, this 12.6 minutes/day ST difference could potentially represent a missed opportunity for girls to increase their fat-free mass index by at least 0.4. Furthermore, when looking at the weekly (63 min/week) and monthly (251.4 min/month) sex differences for the during preschool period, these could potentially represent a missed opportunity for preschool girls to increase their fat-free mass index by approximately 2.5 in a given week and 10.1 in a given month. Even though we are aware that not every single minute in ST can be substituted with vigorous physical activity, substituting at least half of it (∼ 6 minutes) in preschool girls can have the potential to reduce sex disparities in ST.
Although no other US studies examine differences in ST by periods of the day in preschoolers, results from a study using NHANES data, including US children and adolescents, mirror our findings. 6 The authors reported that girls were more sedentary than boys during school, after school, and on weekday evenings after controlling for race/ethnicity, annual family income, and BMI. Moreover, they also reported that girls were more sedentary than boys for the entire day (minutes/day or h/day) and that this disparity is mainly driven by the during school period. Interestingly, our findings only partially align with this work. We did not see any sex disparities in overall ST in the current study, but the sex disparity in ST during preschool time was significant whereby girls were more sedentary than boys. It is possible that the difference in ST during preschool time we observed is not as drastic as disparities noted in later life stages which reflect in both in school time and overall ST. Nonetheless, the difference in ST by sex during preschool time demonstrates that these disparities start in earlier stages (e.g., preschool), placing girls at a disadvantage. Moreover, a previous non-US study with a similar sample size reported sex disparities in overall ST assessed via accelerometry among preschoolers. 5 They reported a sex difference of 107 minutes/day in ST-favoring boys. 5 Thus, intervening early in life during preschool hours is important and could reduce ST sex disparities in subsequent developmental stages.
We are aware that the current study aimed to understand if and not why sex disparities in ST are occurring during preschool time. However, it is important to discuss the findings about known health, developmental, and behavioral factors such as BMI and self-regulation that can affect ST during preschool hours. For instance, a study testing the ST correlates among 331 US preschoolers reported that girls were more sedentary than boys and that for girls, ST was positively associated with BMI and negatively associated with coordination. 21 In the present study, more than 50% of the sample that was classified as obese were girls, which may be one reason for sex differences in ST. Although US national data shows that preschoolers (2-to-5-year-old) have a 13% prevalence of being classified obese and that African American girls and adolescents have a 31% prevalence of being classified as obese, 10 we still believe that our data should be interpreted with caution due to oversampling concerns. Thus, there may be an oversampling of obese participants in general or an oversampling of obese girls.
Regarding behavioral factors, it is known that preschoolers with better self-regulation skills are more likely to show fewer classroom behavior problems (i.e., problems accepting authority) compared to those with poor self-regulation skills, 22 and that girls tend to have better self-regulation skills compared to preschool boys. 13 This could result in girls sitting for more extended periods to complete a task compared to preschool boys. We believe that better self-regulation skills in girls allow them to be engaged for longer periods in activities such as drawing, coloring, crafting, and playing with puzzles, which normally results in more time sitting since it can help them do these tasks with ease. This current study did not examine self-regulation in preschoolers, but future studies should consider including these factors to further understand sedentary behavior in young children. Future research should also include observational tools to better understand activities occurring during preschool time that might lead to differences in ST between boys and girls. Thus, we recommend a mixed-method study to collect qualitative data from the teachers of the activities they asked children to do during preschool time as well as quantitative data such as (1) ST device-based data, (2) self-regulation scores, and (3) observational data to understand preschoolers ST preferences and ST activity differences between boys and girls.
Our hypothesis was partially supported since no sex differences were observed in ST during the after-preschool period. It is not clear why we did not find sex differences in ST during the after-preschool hours. It is possible that we did not consider other factors such as parental perceptions, which might explain the lack of sex difference in ST after preschool hours. For instance, an observational study recruited 388 preschoolers’ parents (57% Black or other/mixed race and 61% with an annual household income < 50K) from a midwestern city in the United States. 23 The study tested the parents’ attitudes and perceptions about their child’s physical activity and outdoor time at home and at preschool. The authors reported that although parents believed that physical activity was highly important for preschoolers, many (25% of the sample) thought their child could get sick from playing outside in the cold. Also, parents reported being more comfortable with their preschoolers playing outside at preschool than at home. Lastly, analyses by socioeconomic status showed that parents with a low annual household income do not feel comfortable with their preschoolers playing outside at home. 23 It is possible that these attitudes and perceptions are shared with the parents of our sample (most of them were African Americans and from low-income families) and may impact ST after preschool hours regardless of sex.
Limitations
To our knowledge, this study is the first to analyze ST by periods of the day in a US preschool sample, but it is not exempt from limitations. Findings from this study are not generalizable since all participants were recruited from the same geographical area, and the sample consisted mainly of African American preschoolers from low-income families. It is known that ST levels can be different for people based on their race/ethnicity. For example, African American children are more likely to be sedentary compared to their non-Hispanic White and Mexican counterparts. 24 Thus, the findings from this study had a stronger potential to apply to African American preschoolers.
Only standardized wake and bedtimes were used in the present study, which can limit our ability to accurately determine sleep time. Future studies should incorporate sleep logs and device-based measures to obtain sleep. Using sleep logs to supplement the device-based data, allows us to know when a participant’s bedtime and wake time allows us to make a more accurate estimation of sleep and avoids the possibility of including sleeping time as ST. Findings from this study should be interpreted with caution since only 4% of the variance in ST during the preschool period was explained by sex. This means that other variables that can potentially explain ST were not considered such as parental education and preschool curriculum. Literature has shown that parents with low educational backgrounds are more likely to spend time playing outdoors with their children, which is related to preschoolers’ lower ST levels. 25 Also, research shows that preschool curriculums that incorporate time for preschoolers to be physically active as part of their daily routines result in more active children during preschool time. 26 Additionally, the present study is a secondary analysis of baseline data of a cluster randomized control trial, in which the main outcome was physical activity instead of ST. Thus, daily sedentary activity logs and teachers’ qualitative data about preschoolers’ ST were not conducted. This limits our ability to complement our device-based data. Therefore, future research to determine why preschool girls are more sedentary than boys should incorporate sedentary activity, sleep logs, and teacher interviews to fully understand sex disparities in ST occur at an early stage such as preschool. Lastly, including a US representative sample will allow the translation of findings broadly to US preschoolers.
Conclusions
Findings show that sex differences in ST during preschool years are driven by the during preschool hours, which can represent an unfavorable health impact among preschool girls. The childhood obesity prevalence dramatically increases from 12% in preschool age (2-to-5 years old) into 21% during childhood (6-to-11 years old). 13 Thus, it is encouraged to implement family-based interventions during preschool to provide parents/caregivers and preschoolers practical strategies to develop habits and knowledge around healthy eating and reduction of ST for them to carry into childhood and so on.
Impact Statement
Findings show that sex differences in sedentary time (ST) exist during preschool hours, placing girls at a disadvantage which could have long-term health consequences such as obesity. Therefore, from an early childhood curriculum and policy standpoint, there is a need to further explore ST during preschool hours.
Footnotes
Acknowledgment
A special thanks to all the preschool centers and preschoolers that were part of the study.
Authors’ Contributions
M.E.S.R.: Conceptualization, methodology, software (SAS), formal analysis, data curation, writing—original draft, visualization. K.A.P.: Conceptualization, writing—review & editing, supervision, and resources. K.K.P.: Investigation, data curation, writing—review & editing, and project administration. L.E.R.: Investigation, resources, writing—review and editing, supervision, project administration, and funding acquisition.
Author Disclosure Statement
All authors declare that they have no conflicts of interest.
Funding Information
The study is funded by a 5-year grant from the National Heart, Lung and Blood Institute (NHLBI) at the National Institutes of Health (NIH); R01-HL-132979 $2 564 256. The Principal Investigator (PI) is Leah E Robinson, PhD, School of Kinesiology at the University of Michigan. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of NIH.