
Abstract
Background:
Maternal consumption of fruits and vegetables can reduce future childhood obesity risk. Health Bucks, a fruit and vegetable voucher program redeemable at New York City (NYC) farmers’ markets, supports access to fresh produce.
Methods:
In a cross-sectional analysis within a cohort study, we evaluated the integration of Health Bucks into the prenatal expansion of a primary care-based obesity prevention program. We analyzed data from 176 pregnant Latina participants at a NYC public hospital, with vouchers given to 114 (64.8%) participants. Later in infancy, we measured maternal outcomes (fruit and vegetable intake, stress) and food access (food environment, household food insecurity). We performed adjusted regression analyses to evaluate outcome differences between those who received vouchers and those who did not. Secondary analyses assessed whether voucher redemption or first-trimester timing of distribution were associated with outcomes.
Results:
Receipt of vouchers was associated with higher daily fruit and vegetable intake (incident rate ratio [IRR] = 1.3 [95% confidence interval [CI]: 1.1, 1.6]), and lower stress (B = −1.9 [95% CI: −3.7, −0.1]). Voucher redemption was associated with higher daily fruit and vegetable intake (IRR = 1.3 [95% CI: 1.04, 1.6]). First trimester receipt was associated with a favorable view of the neighborhood food environment (adjusted odds ratio = 5.5 [95% CI: 1.04, 28.6]) and lower stress (B = −3.8 [95% CI: −7.5, −0.1). We did not detect associations with food insecurity.
Conclusion:
Integrating Health Bucks into a prenatal obesity prevention program was associated with favorable outcomes. Subgroup analyses showed that voucher redemption and first-trimester receipt were associated with positive outcomes, guiding strategies for fruit and vegetable voucher distribution.
Introduction
Major public health efforts have focused on increasing fruit and vegetable intake given their nutritional content and ability to protect against obesity.1,2 Researchers have shown that limited healthful food access during pregnancy compromises maternal dietary practices and increases feelings of stress,3,4 with negative health consequences for both the pregnant person and their infant.5,6 Programs which work to expand fruit and vegetable access by lowering their cost relative to calorie-dense, less nutritious alternatives are on the rise.7,8 Optimizing access to these programs during pregnancy are likely to lead to positive effects on obesity prevention across the life course.
Growing evidence on fresh produce voucher programs—part of the rising “Food is Medicine” movement9,10—indicates favorable nutritional outcomes for children and their families.11,12 Higher rates of voucher redemption are associated with increases in fruit and vegetable intake.12,13 However, a greater focus on maternal-infant outcomes is needed to guide strategies to prevent the intergenerational transmission of obesity. 14
Other financial assistance programs help meet basic needs and reduce parental stress, 15 a driver of unhealthy feeding practices.16,17 Smaller-scale studies 18 have shown the potential of integrating vouchers into primary care programs to complement initiatives already promoting healthy infant feeding practices. The Starting Early Program (StEP) is a primary care-based pediatric obesity prevention program that promotes healthy nutrition and lifestyle practices. Expanded analyses showed reduced impacts on child weight when household food insecurity was present during the third trimester of pregnancy. 19 Thus, to address risks earlier, StEP was extended to the first trimester to initiate timely support in anticipation of pregnancy and early parenting.20–22
Health Bucks are fruit and vegetable vouchers redeemable at New York City (NYC) farmers’ markets—neighborhood marketplaces where farmers gather to sell fresh produce. For a subset of StEP-Prenatal participants enrolled during the 2019 farmers’ market season, the program distributed Health Bucks to acknowledge financial constraints, providing an opportunity to evaluate their outcomes compared with those who received StEP-Prenatal programming only. We hypothesized that pregnant participants who received Health Bucks would demonstrate better maternal outcomes (higher fruit and vegetable intake, lower stress) and higher food access (perceived healthier neighborhood food environment, lower food insecurity). We hypothesized that receiving vouchers for a greater duration (reflecting a higher dose), redeeming vouchers (indicating deeper engagement), or receiving vouchers in the first trimester (a formative life stage) would be associated with more favorable outcomes.
Methods
Study Setting and Participants
This study took place at Bellevue Hospital Center, the safety net hospital of NYC. Participants were from StEP-Prenatal, a single arm feasibility trial to expand an evidence-based intervention to the first trimester of pregnancy. 22 In StEP-Prenatal, registered dietitians deliver group-based nutrition and lifestyle support coordinated with well visits from first trimester into early childhood. Eligibility criteria for the trial included being in the first trimester of pregnancy, self-identification as Hispanic or Latina, English or Spanish speaking, and intention to continue primary care at Bellevue. We selected this criteria because Hispanic and Latino communities are at higher risk for obesity and food insecurity.23,24 The feasibility trial excluded participants younger than 18 years, uncertain pregnancy dating, severe mental illness, or shelter system residence due to challenges in following them over time as a cohort.
Study Design
This study was a cross-sectional analysis of data from a cohort study that enrolled pregnant participants between December 2018 and February 2020. We did not randomize receipt of vouchers to avoid withholding an intervention with probable benefits by chance.11,25,26 Instead, we distributed vouchers sequentially to the subset of pregnant participants during the May to November 2019 farmers’ market season. We distributed vouchers in the value of $0.50/day/household member in monthly installments for up to 6 months, continuing into early infancy if the parent delivered before the end of the season (Fig. 1). All vouchers were distributed and redeemed prior to closures from the COVID-19 pandemic. We measured maternal outcomes at three months postpartum to ensure the outcome assessment followed initial voucher distribution and to capture when maternal outcomes are likely to influence infant feeding practices. The Institutional Review Board at NYU Grossman School of Medicine and NYC Health + Hospitals/Bellevue approved this study.

Quasi-experimental study design.
Health Bucks Program
At the time of the study, there were 140 participating NYC farmers’ markets where people could redeem Health Bucks. To support voucher utilization, dietitians identified farmers’ markets close to home and designed recipes with families. The NYC Department of Health and Mental Hygiene tracked voucher redemption by serial number and we matched these serial numbers to participant-issued vouchers.
Assessments
Our outcome variables were assessed at baseline and at 3 months postpartum, except for food insecurity, which was assessed by the parent trial at 10 months postpartum.
Maternal Outcomes
Fruit and vegetable intake
We assessed maternal fruit and vegetable intake using questions from the Center for Disease Control’s Behavioral Risk Factor Surveillance System. 27 This assessment contains five questions that count the number of times respondents consumed the following: (1) fruit (nonjuice); (2) canned beans (e.g., baked, garbanzo); (3) dark green vegetables (e.g., broccoli, spinach); (4) orange-colored vegetables (e.g., sweet potatoes, carrots); and (5) other vegetables that are not fried (e.g., corn, eggplant). Respondents reported intake frequency as an open-ended response, then specified whether this was per day, week, or month. To ensure consistency, we standardized responses to reflect daily intake by dividing weekly intake by 7 and monthly intake by 30. To maintain granularity per prior work, 28 we assessed this variable as a count, representing event occurrences.
Maternal stress
We assessed maternal stress using the Perceived Stress Scale, a validated, widely used, 10-item instrument that assesses the degree to which life feels unpredictable and overloaded. 29 Participants answer on a Likert scale with a score of 1 indicating “Never” and 5 indicating “Very often” to capture stress frequency and intensity. Prior work with this measure show that scores are associated with feeding styles. 30 Scores range from 10 to 50 with higher scores indicating higher levels of stress. Per prior work, 31 we assessed this variable continuously.
Food Access Outcomes
Neighborhood food environment
We measured perceptions of the neighborhood food environment with the “Healthy Food Access” five-item subscale from the Neighborhood Characteristics Place-Based Survey. 32 The subscale evaluated how easy it was to purchase healthy food near the participant’s home. Participants answered on a five-point Likert scale ranging from “Strongly agree” to “Strongly disagree.” There is no validated cutpoint; to capture the most favorable perception, we chose a cutpoint of “Strongly Agree” to all five items.
Food insecurity at 10 months
We assessed household food insecurity using the 10-question US Department of Agriculture (USDA) Core Food Security Module. 33 We categorized households as food insecure using the validated cutoff 33 at whether they endorsed three or more food insecure conditions.
Predictor: Receipt of Health Bucks Enhancement
We measured the number of months that a participant received Health Bucks, and categorized participants into the voucher recipient group if they received vouchers at least once. To assess redemption and timing, we constructed two additional variables. First, we created a variable with 3 categories: those who did not receive vouchers (reference group), those that received vouchers but did not redeem them, and then those that received and redeemed vouchers. To assess first trimester timing, we created another variable with 3 categories: those who did not receive vouchers (reference group), those that received vouchers during the first trimester, and those who received vouchers after the first trimester.
Study Covariates
We reviewed prior work on food insecurity in this life stage to select covariates.3,4,28 We included maternal age (years), education (less/more than high school), partnership status (single/married or living as married), US born (yes/no), firstborn status (yes/no), employment status (yes/no), and whether they received benefits from Special Supplemental Nutrition Program for Women, Infants, and Children. As per prior work34,35 we also adjusted for the corresponding baseline corresponding maternal or food access outcome as described above to account for initial levels.
Statistical Analysis
We summarized sociodemographics, conducting groupwise comparisons between recipients and nonrecipients of Health Bucks. We used regression models to assess associations between receipt of vouchers and our outcomes. For our count outcome, daily maternal fruit and vegetable intake, we used Poisson regression 36 to report adjusted incident rate ratios (IRR). We used linear regression to assess our continuous maternal stress outcome, and logistic regression for our dichotomous food access outcomes (neighborhood food environment and food insecurity). With similar models, we also assessed whether the number of months a participant received vouchers were associated with outcomes. We adjusted for the above covariates and for the relevant baseline variable (e.g., baseline maternal stress for models assessing maternal stress).
In secondary analyses, we investigated differential effects of voucher redemption and initiation of voucher distribution in the first trimester. We compared sociodemographics using groupwise comparisons between participants who redeemed versus did not redeem vouchers and those who received them in the first trimester versus those who did not. Using variables described above, we performed separate adjusted regression models to predict whether there was outcome variation based on redemption or first trimester timing. Given that first trimester timing is likely confounded by longer duration of Health Bucks receipt (e.g., those who started receiving vouchers near the end of pregnancy only received vouchers for 3 months at the postpartum assessment), in these models, we additionally adjusted for duration of voucher receipt in months.
All estimates were presented as incidence rate ratios (IRRs), odds ratios (ORs) or unstandardized ordinary least squares coefficients (Bs) with 95% confidence intervals (CIs). We conducted analyses with Stata/SE version 15 (Stata Corp, College Station, TX).
Results
Of 233 enrolled participants, we included 176 participants who were followed through infancy (>75% retention rate). The majority were non-US born (75.6%), partnered (72.7%), had at least a high school education (74.5%), and about half were working (52.8%). We did not detect significant sociodemographic differences between the group that received vouchers and the group that did not (Table 1). Over half (64.8%) of participants received vouchers. They began receiving vouchers at 20.1 weeks gestation (standard deviation = 7.5) on average and for a median duration of 5 months (Interquartile range: 3 to 6 months). The majority (96 participants, 84.2%) of those who received vouchers redeemed them. Table 2 summarizes the sample by voucher redemption status and first-trimester receipt.
Sample Characteristics by Health Bucks Receipt
No significant differences between groups at the p < 0.05 level.
SD, standard deviation.
Maternal Characteristics by Redemption Status and Timing
*Significant differences between groups at the p < 0.05 level.
Associations Between Receipt of Health Bucks and Main Outcomes
Table 3 and Figure 2 display that receiving Health Bucks vouchers was associated with higher daily maternal fruit and vegetable intake (IRR = 1.3 [95% CI: 1.1, 1.6]) and lower stress (B = −1.9 [95% CI: −3.7, −0.1]). Each additional month of vouchers received was weakly associated with higher daily fruit and vegetable intake (IRR = 1.1 [95% CI: 1.0, 1.1]), but not associated with lower stress (B = −0.3 [95% CI: −0.6, 0.1]). Our main analyses did not detect associations between receiving vouchers and food access as measured by neighborhood environment (adjusted OR [aOR] = 1.3 [95% CI: 0.7, 2.3]) or food insecurity (aOR = 0.7 [95% CI: 0.3, 1.6]).
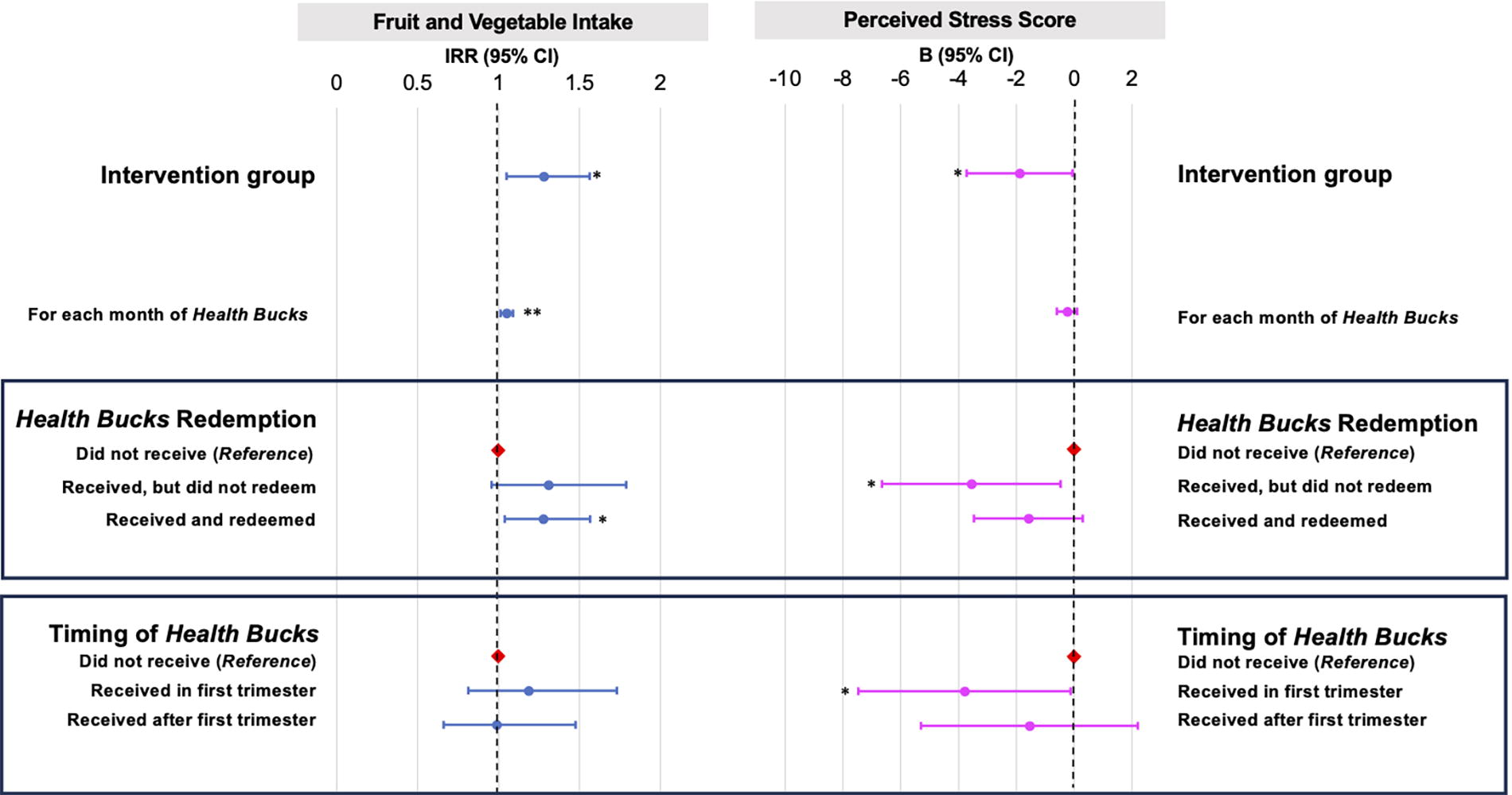
Associations between prenatal Health Bucks and maternal outcomes in infancy. Models adjusted for maternal age, education, partnership status, US born, first born status, employment status, whether they were participants in the Special Supplemental Nutrition Program for WIC, as well as baseline measurement of the corresponding outcome variable (e.g., baseline maternal stress for models assessing maternal stress). *p < 0.05; **p < 0.01. WIC, Women, Infants, and Children.
Associations between Prenatal Receipt of Health Bucks and Maternal Outcomes Measured during Infancy (n = 176)
p < 0.05; All adjusted models included maternal age, partnership status, US nativity, parity, maternal education, employment status, baseline use of Special Supplemental Nutrition Program for Women, Infants, and Children, as well as baseline measurement of the corresponding outcome variable (e.g., baseline maternal stress for the model assessing maternal stress).
Poisson regression model for a count outcome reported in incidence rate ratios.
Linear regression models examined continuous maternal wellness outcomes.
Logistic regression models examined dichotomous food access outcomes.
Outcome variables assessed when infant was 3 months old. Household food insecurity assessment measured with US Department of Agriculture Core Food Security Module, only available when infant was 10 months, n = 162.
aOR, adjusted odds ratio; CI, confidence interval; IRR, incident rate ratio.
Maternal Outcomes: Effects of Health Bucks Redemption and Timing
In our subgroup analyses, Figure 2 displays that redemption of Health Bucks vouchers was associated with higher daily fruit and vegetable intake (IRR = 1.3 [95% CI: 1.0, 1.6]). We did not detect associations between first-trimester voucher receipt and daily fruit and vegetable intake (IRR = 1.2 [95% CI: 0.8, 1.7]). As compared with participants who did not receive vouchers, voucher redemption showed a nonsignificant trend toward lower stress (B = −1.6 [95% CI: −3.5, 0.3]). However, the receipt of vouchers alone was still associated with lower stress (B = −3.6 [95% CI: −6.7, −0.5]). Receipt in the first trimester was associated with lower stress (B = −3.8 [95% CI: −7.5, −0.1]) as compared with those who did not receive vouchers. We did not detect associations with stress in those who received vouchers later in pregnancy (B = −1.6 [95% CI: −5.3, 2.2]).
Food Access Outcomes: Effects of Health Bucks Redemption and Timing
Table 4 displays that receiving vouchers first trimester was associated with higher odds of perceiving a healthy neighborhood food environment (aOR = 5.5 [95% CI: 1.04, 28.6]) as compared with those who did not receive vouchers. We did not detect effects of first trimester receipt of vouchers on food insecurity (aOR = 0.5 [95% CI: 0.1, 3.4]). We also did not detect effects of voucher redemption on food access outcomes including neighborhood food environment (aOR = 1.3 [95% CI: 0.6, 2.8]) or food insecurity (aOR = 0.8 [95% CI 0.3, 2.0]).
Food Access Outcomes: Effects of Health Bucks Redemption and Timing (n = 176)
p < 0.05; Logistic regression models examined dichotomous food access outcomes; All adjusted models included maternal age, partnership status, US nativity, parity, maternal education, employment status, baseline use of Special Supplemental Nutrition Program for Women, Infants, and Children, as well as baseline measurement of the corresponding outcome variable (e.g., baseline maternal stress for models assessing maternal stress).
All outcome variables assessed when infant was 3 months old. Food insecurity assessment only available when infant was 10 months, n = 162.
These models additionally adjusted for number of months Health Bucks were received.
Discussion
We evaluated a fruit and vegetable voucher enhancement of a primary care-based obesity prevention program among Latina pregnant participants at a NYC public hospital. We detected associations between prenatal receipt of Health Bucks vouchers with higher maternal fruit and vegetable intake as well as lower maternal stress postpartum. A key innovation of this study is its exploration of how redemption and timing may influence program outcomes. In subgroup analyses, we found that voucher redemption was associated with higher fruit and vegetable intake, and first trimester receipt was associated with lower maternal stress and a favorable view of the neighborhood food environment. Programs tailored for communities with obesity risk have largely focused on dietary educational strategies; this study presents findings about a program enhancement that acknowledges financial barriers.
Receiving Health Bucks vouchers was associated with higher fruit and vegetable intake, reinforcing prior findings.11,12,25 This interpretation is further supported by our significant findings on dose (months received) and voucher redemption. Vouchers were distributed in an obesity prevention program alongside nutrition counseling. The vouchers may have reinforced the value of healthy foods, serving as an educational cue. We did not detect statistical differences in sociodemographics between the redemption groups—likely due to insufficient power—but those who redeemed had higher baseline food insecurity as compared with those who did not. The relatively modest amount26,37 of vouchers distributed in this program alone are unlikely to improve a family’s overall financial circumstances. Thus, the enhanced educational component may explain the higher fruit and vegetable intake without a corresponding difference in food access.
We also found that receiving Health Bucks were associated with lower maternal stress. Parenting stress—a priority for the US Surgeon General’s Office 38 —is important for healthy infant feeding practices.16,17 Associations were pronounced when participants received vouchers first trimester, but this association was significant even when participants did not redeem vouchers. Simply receiving vouchers may reduce stress by making the healthy foods emphasized in nutrition education more financially accessible, fostering a sense of control over diet and well-being. Vouchers, particularly from a trusted primary care setting, may increase feelings of prenatal social support even without redemption, which has been associated with healthy infant growth. 39 Studies of unconditional cash transfers, which have no stipulations about how families spend the money, are associated with improved parent mental health; 15 this is one of the first studies to show that vouchers, or “near-cash,” benefits during pregnancy are also associated with lower parent stress. 40 First trimester recipients were more likely to be non-US born, which may contribute to the high value of social support.
We found no associations between Health Bucks and a favorable view of the neighborhood food environment, except when received first trimester. Attitudes may be most malleable early in pregnancy when people are navigating a new parental identity based on available resources.20–22 We accounted for the number of months that parents received Health Bucks in our models, but isolating the impacts of first trimester timing is challenging due to the high risk of confounding. Future studies could randomize participants to receive vouchers during first trimester or evaluate whether timing interacts additively with voucher redemption to strengthen outcomes. Perceptions of the food environment may also be confounded by distance to fresh produce, accounting for it as a future covariate may provide deeper insights.
We did not find associations between Health Bucks—whether received or redeemed—and food insecurity. This finding contrasts with other evaluations showing positive impacts of nutrition incentive programs on food insecurity.26,37 These larger studies, which involved 500 to over 3000 participants, enrolled more broadly—families with low income rather than pregnant individuals—and in many cases were able to distribute vouchers of higher value (up to $300 per household).26,37 Our study measured food insecurity dichotomously, potentially missing shifts from high to moderate food insecurity. Future work may also consider using the 18-item version of this measure 33 which includes questions for households with children. Our baseline food insecurity rate was about ∼20% (national rates are 13.5% 41 ), limiting our ability to detect differences.
These findings inform efforts to bridge food assistance with maternal–child health services. Programs to address resource needs like food range from “in-kind” provisions (e.g., directly giving food) to unrestricted cash transfers—these offer the greatest degree of autonomy but have less precision in targeting specific health behaviors. 15 We detected that receipt of a prenatal “near-cash” fruit and vegetable voucher—perhaps representing a balance between the benefits of an “in-kind” and unrestricted cash transfer—is associated with positive maternal outcomes in infancy as compared with those who did not receive a benefit.
The strengths of this study build upon limitations of prior studies, including the ability to assess exposure before outcome, the verification of voucher redemption (vs. self-report), as well as our sampling of participants at higher risk for obesity. 42 Observational correlational analyses have inherent limitations, including the inability to establish causality and unmeasured confounders. Health Bucks distribution took place during farmers’ market season, thus the comparison group was likely to have a different set of seasons during pregnancy. While there is likely a seasonal pattern to birth numbers, whether there is seasonality to maternal-fetal outcomes is mixed.43,44 Our survey measures were self-reported, vulnerable to recall bias. Finally, while the Health Bucks enhancement took place prior to the COVID-19 pandemic, our outcomes were assessed between November 2019 and January 2021, overlapping with pandemic-related stressors. This may have overshadowed subtle variations in stress or underestimated stress levels.
In conclusion, this study evaluates a fruit and vegetable voucher enhancement of a primary care-based obesity prevention program Our findings guide future study designs that include longitudinal repeated measures to increase causal inference and inform upcoming efforts to integrate “near-cash” voucher strategies to enhance primary care-based programs to optimize lifelong health.
Impact Statement
This study describes how fruit and vegetable vouchers integrated into primary care-based prenatal and pediatric obesity prevention are associated with maternal outcomes and food access, especially when redeemed or given early in pregnancy. These findings inform strategies to promote healthful dietary practices from the start of life to prevent obesity.
Footnotes
Acknowledgments
The authors are grateful to the Starting Early Program staff and participants for their contributions and involvement. The authors would also like to express their gratitude for the expertise and support provided by Kristyn Pierce, MPH, their departmental biostatistician.
Authors’ Contributions
C.D.-L. and R.S.G.: Conceptualization, methodology, analysis, and writing—original draft preparation. M.J.M. and M.W.K.: Investigation, data curation, analysis, and writing—reviewing and editing. C.N.K., E.R.W., and J.V.B.: Data curation, analysis, and writing—reviewing and editing. L.T.: Methodology and writing—reviewing and editing. As the authors of this article, they are responsible for the reported research. All the authors have all approved the article as submitted.
Author Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
Funding Information
This work was supported by the National Institute of Food and Agriculture, U.S. Department of Agriculture 2017-68001-26350, the Ample Table for Everyone Foundation, NIH/National Institute for the Environmental Health Sciences (K23ES035461), NIH/National Heart, Lung, and Blood Institute (K23HL159326), and the Sala Elbaum Pediatric Research Scholars Program. The funders did not participate in study design, collection, analysis, interpretation of the data, writing of the report, or the decision to submit the article for publication.