
Abstract

There is growing concern over the current ‘one-size-fits-all’ approach to drugs used in the treatment of autoimmune (AI) disease, which is in no small part a result of the difficulty associated with identifying AI disease subgroups. This inability to effectively stratify patient populations means that a drug designed to manage specific symptoms can have a range of effects in different patients based on an individual's genetic predisposition and unique physiological responses. In fact, most drugs used to treat autoimmune diseases show a maximum response rate of only 50 percent1. The result is a large number of patients undergo an often-lengthy trial and error period as clinicians search for the most effective treatment.
To mitigate the imprecise path to the most appropriate treatments, physicians are increasingly looking to companion diagnostics (CDx) that can help to evaluate and define patient subgroups with respect to their unique molecular profile and personalized responses to a particular drug, CDx allow for better patient stratification, and can significantly contribute to improved patient wellbeing, quality of life and long-term prognosis when paired with effective, personalized therapeutics.
CDx Challenges and Benefits
In order to enable the effective development of a companion diagnostic, the drug development program must be aligned with a CDx program from very early in the process. Unlike the development of a cancer drug CDx where the specific targeted genetic mutations are often known from the beginning, development of CDx for autoimmune diseases can be problematic, as no such genetic predispositions or stratification biomarkers are readily available. Thus, due to the lack of appropriate biomarkers drugs are often developed for the full market and the stratification need may not become apparent until relatively late in a clinical development program. Often this information is only brought to light when larger patient groups are being recruited in phase III trials and once their clinical responses or often lack of them are observed.
Aware of these shortcomings, drug development companies often use the expression levels of the drug target to stratify patients and to try and enrich the response rate, so far with a limited success rate. This means that a better understanding of the molecular nature of a disease is paramount in order to improve the success rate of novel autoimmune disease therapies.
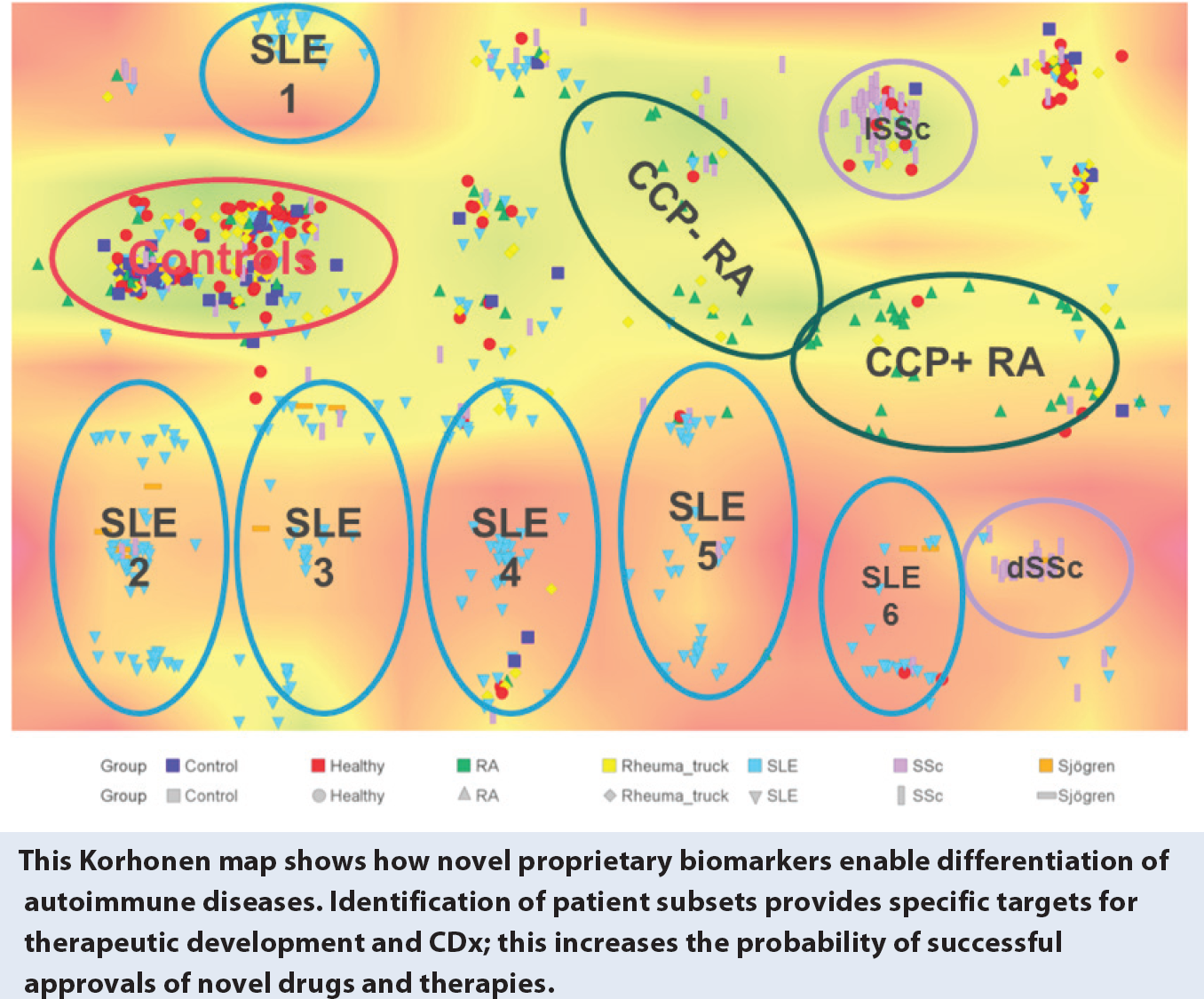
Many of the systemic autoimmune diseases, such as Systemic Lupus Erythematosus (SLE), are considered syndromes rather than single disease entities. Here, a better understanding via the molecular dissection of the disease can differentiate various subgroups via specific biomarkers. Such biomarkers can be used for a more targeted selection of patients, and lead to smaller, cheaper, more effective trials and ultimately development programs.
In addition, while not restricted to biomarker-selected patients, there are ethical issues around the inclusion of negative controls, i.e. patients known or expected not to respond to the drug. Fortunately, this is an issue that has been foreseen by the FDA, who released their Enrichment Strategies for Clinical Trials in 2012 with the intention of increasing the chance of clinical trial success even with smaller sample size.2
Selecting patients based on biomarker data means that trial endpoints around efficacy and safety are more likely to be achieved. Creating a strategy for CDx development early in the drug development cycle has additional benefits beyond improving patient outcomes. These include increased chances a drug will gain regulatory approval and can result in a drug being brought to market quicker. In addition, reimbursement policies and pricing issues are improved by demonstrating the combined effect of the CDx and the drug.
CDx and Stakeholders
All stakeholders, despite their varying interests, would agree that there is no way around a more personalized approach to patient management and treatment in autoimmune diseases and that CDx are the way forward. Although pick up has been slow and the field is probably 10-20 years behind oncology in this regard, there are considerable efforts to change this and to catch up as fast as possible.
Healthcare Professionals
Healthcare professionals focus on finding the best and most suitable treatments for their patients. CDx will allow them to prescribe drugs more accurately and tailor therapy to the individual, enhancing clinical utility. Freed from the trial and error method of finding the most appropriate treatment for each patients will help create more efficient, higher quality healthcare, which in turn will improve patient wellbeing, reduce repeat doctor visits, lower costs and significantly slow disease progression in those treated with an inappropriate drug regimen, especially in autoimmune indications which are generally progressive and so far incurable.
Pharma and Biotech
CDx will also open up a valuable market opportunity for companies currently working on the identification and development of clinically relevant biomarkers for autoimmune diseases. This in-depth research into under-served disease areas will result in a deeper insight into disease pathology and progression, which could potentially result in the discovery of novel therapeutic targets and treatments. Having the ability to stratify patient populations into disease subgroups provides an avenue for CDx development which can ultimately lead to much more targeted therapeutic options, including combination therapies, resulting in higher response rates.
Regulators and Payers
A major concern for healthcare payers is the reimbursement criteria for drugs and diagnostics. This is a topic of highest relevance in the U.S. and Europe. CDx have the ability to help discriminate between different subsets of patients, highlighting groups of patients eligible for a potentially expensive drug, while excluding others. This serves to save the healthcare system unnecessary costs and enables patients to receive adequate treatment earlier. However, CDx could also lead to conflicting interests, if companies are producing drugs with innately higher levels of efficacy and safety, but feel they are not being compensated financially for the enhanced technological level of these products.3
Many healthcare payers, both public and private, assess drugs and CDx as separate entities. They don't take an integrated, holistic approach to evaluate the CDx as tools that effectively improve care and lower costs by both eliminating non responders (and, in turn, reducing the amount paid for ineffective treatment) while pinpointing those patients who will respond best to the targeted treatment.
Too often today a drug, but not its CDx, will receive reimbursement. Looking to one of the oldest CDx for cancer treatment, Herceptin is widely reimbursed through the EU, while its CDx, HER-2/neu, varies in its reimbursement status: in France, the HER-2 test was authorized in 2000 but only reimbursed in 2007; in the U.K. and Germany it is publically funded; and in Spain, Pharma companies fund most of the testing. This lack of joint assessment can result in lower reimbursement prices, making it difficult for smaller companies to invest in the development of novel, effective CDx. In the U.S., the FDA released in 2014 guidance for in vitro companion diagnostics that paves the way to encourage the co-development of CDx with a drug moving through clinical trials.
The health cost burden for autoimmune diseases is already significant and growing annually. The progressive nature of these diseases demands an early and effective intervention. This can only be ensured via a personalized medicine approach in which novel therapies are developed for specific patient subgroups that are most likely to benefit from such treatments. The fast and efficient development, approval and reimbursement of appropriate CDx/drug combinations should be a major goal for all stakeholders involved in autoimmune diseases and will ultimately benefit everybody involved—first and foremost the patients suffering from these diseases.