
Abstract
Abstract
This study utilizes an innovative experimental paradigm to investigate the effects of virtual reality (VR) on dissociative experience and the sense of presence. A nonclinical sample of 30 people were administered measures of dissociation, sense of presence, and immersion before and after an immersion in a virtual environment. Results indicate an increase in dissociative experience (depersonalization and derealization), including a lessened sense of presence in objective reality as the result of exposure to VR. Higher preexisting levels of dissociation and a tendency to become more easily absorbed or immersed were associated with higher increases in dissociative symptoms resulting from VR immersion. Results are discussed in terms of imaginative processes underlying the dissociative experience and potential implications to the treatment of anxiety disorders with VR.
Introduction
Cognitive-behavior formulations of dissociative experience and its pathological manifestations are still in the early stages, although imagination inflation and fantasy proneness have been identified as relevant factors in dissociative experiences.3–5 In particular, it has been suggested that a tendency to become easily absorbed into the imagination may give rise to a feeling of detachment and sense of unreality toward the external world. More recently, cognitive-behavior formulations have also identified a strong focus on the self, often characterized by frequent questioning and catastrophic misinterpretation of transient symptoms, which may exacerbate feelings of DP/DR. 6
The construct of dissociation is ill defined, frequently referring to a wide variety of nonclinical and clinical phenomena, which often leads to confusion among researchers and theoreticians. 7 Holmes et al. 7 suggest two qualitative distinct forms of dissociation, one characterized by compartmentalization phenomena with dissociative amnesia as a central feature, and the other primarily characterized by feelings of detachment, which incorporates symptoms of DP/DR. A sense of detachment is a distinct feature of dissociative experience in general, which may take on either a pathological format as in the case of DPS or a nonpathological format when associated with fatigue or mild intoxication.
Interestingly, according to these definitions, research into virtual environments has also focused on concepts closely related to a sense of detachment from reality. In particular, it highlights the importance of constructs like the level of immersion and presence. The feeling of immersion, whether physical or psychological in nature, allows the user to either feel or believe that he or she has left the real world and is now interacting with a virtual environment. Unlike research on dissociative disorders, however, these constructs generally refer to level of immersion and presence with respect to a particular virtual environment (as opposed to the level of immersion and presence within objective reality). Yet the concepts are quite similar and seem closely interrelated. In fact, a higher degree of immersion or presence in a virtual environment would naturally imply a greater level of detachment from external reality. In particular, it has been suggested that those prone to dissociative symptoms have more difficulty tolerating discontinuity in perceptual environments, often reflecting a rigid stance toward perception.3,4 As such, perceptual discontinuity as induced by temporarily being immersed into a virtual environment while absorption into objective reality is discontinued would be expected to increase dissociative symptoms among those prone to dissociative symptoms.
The present study introduces an innovative experimental paradigm that identifies imaginative processes associated with dissociative experience using virtual reality (VR) to decrease the sense of presence in objective reality and increase feelings of detachment toward objective reality. We predict that (a) exposure to a virtual environment induces dissociative experience; (b) exposure to a virtual environment leads to a lower sense of presence in objective reality; (c) the level of presence in objective reality is associated with a higher degree of dissociative symptoms after exposure to a virtual environment; and (d) the degree of dissociative symptoms induced by a virtual environment is associated with preexisting imaginative tendencies and level of dissociative symptomatology.
Method
Participants
Participants were recruited through an advertisement in the employee newspaper of the staff of Hôpital Louis-Hippolyte Lafontaine (Montreal, Quebec). Participants were initially screened by a telephone interview utilizing a mental health screening questionnaire, the Questionnaire sur la santé. 8 People with a potential anxiety disorder, depressive disorder, substance abuse disorder, or psychotic disorder were excluded. The final sample consisted of 30 participants (14 females, 16 males). The average age was 33.1 (SID = 8.2; range 22–49). Educational levels were as follows: 3.3% had a primary education, 0.0% had a secondary education, 36.7% had a postsecondary preparatory college education, and 60.0% had a university education. Marital status was as follows: 56.7% married or cohabiting, 40.0% single, and 3.3% divorced or separated.
Questionnaires
Cambridge Depersonalization Scale–Trait Version (CDS-T)
The CDS-T 9 measures the frequency and duration of DP/DR symptoms over the previous 6 months (trait version). It was tested on a sample of 77 patients suffering from a DSM-IV depersonalization disorder (35), an anxiety disorder (22), or a temporal lobe epilepsy (20).The scale consists of 29 items capturing the frequency (0, never, to 4, all the time) and general duration of symptoms (1, few seconds, to 6, more than a week). The scale showed good discriminant validity (r = 0.25–0.29), convergent validity (r = 0.80), and high internal consistency (α = 0.89). 9 In addition, the total score of the scale differentiates patients with DSM-IV depersonalization disorder from the other groups.
Cambridge Depersonalization Scale–State Version (CDS-S)
The CDS-S 9 has 22 items representing clinical manifestations of depersonalization symptoms using a visual analogue scale that requires the participant to mark answers along a numerically anchored 100-millimeter line. The scale ranges from 0% (“I'm not having it at all”) to 100% (“It's as bad as it gets”). Most of the items correspond to the trait version but were adapted by the original authors to allow for the state measurement of symptoms of depersonalization. The total score is calculated by adding the item scores. The scale showed excellent internal consistency and reliability in the present study (α = 0.92).
Adapted Igroup Presence Questionnaire (AIPQ)
The AIPQ is an adapted version of the Igroup Presence Questionnaire (IPQ).
10
The IPQ and its modified version, the AIPQ, contain original items from previously developed questionnaires.11–14
The original IPQ was constructed using a large pool of items and two survey waves with approximately 500 participants. Items are answered on a 6-point scale (−3 to 3). The AIPQ used only those items from the original IPQ whose contents allowed for the measurement of sense of presence in objective external reality as well as in a virtual environment. In some cases, items were rephrased so that they could apply to both objective reality and a virtual environment. In addition, because one purpose of the present study was to measure sense of presence in both virtual and objective reality, two different versions of the AIPQ were used, and while there were no differences in the item set, each version had a slightly different instruction. For the measurement of presence in objective reality, the instruction was as follows:
Now you'll see some statements about experiences. Please indicate whether or not each statement applies to your experience in the last 5 minutes. You can use the whole range of answers. There are no right or wrong answers, only your opinion counts. Note that the expression “world surroundings” refers to the physical, “real” world.
For the measurement of presence in a VR environment, the phrase “physical ‘real’ world” was replaced with “the virtual world only.”
The AIPQ consisted of nine items answered on a scale ranging from −3 to 3. Item-total correlations of the AIPQ for the first measurement (in objective reality) ranged from 0.23 to 0.66 (Cronbach's α = 0.73). Item-total correlations of the AIPQ for the second measurement (in the virtual environment) ranged from 0.12 to 0.86 (Cronbach's α = 0.86). Higher (recoded) scores indicate a greater sense of presence in objective reality, or alternatively, if the instruction applied to VR, higher scores indicated a greater sense of presence in VR.
Immersive Tendency Questionnaire (ITQ)
The ITQ 15 measures the tendency or capability to be involved or immersed in activities, including the ability to concentrate and block out distractions. Typical items include “Do you ever become so involved in a daydream that you are not aware of things happening around you?” “How good are you at blocking out external distractions when you are involved in something?” The scale consists of 18 items answered on a 7-point scale. Reliability of the questionnaire is satisfactory (α = 0.75).
Dissociative Experiences Scale (DES)
The DES16,17 is a self-report questionnaire designed to identify patients with dissociative psychopathology and to provide a means of quantifying dissociative experiences. Content for the scale's 28 items was garnered from interviews with dissociative patients and from consultations with clinical experts. The scale taps a broad range of dissociative experiences, including disturbances in memory, identity, and cognition and feelings of derealization, depersonalization, absorption, and imaginative involvement. The final score is calculated by dividing the total score by 28. Reliability findings from various studies range from 0.85 to 0.93. Factor analysis performed on data from nonclinical samples yields a different factor structure than on clinical samples. 18 Specifically, in nonclinical samples, most of the variance is explained by an absorption factor with factor loadings from 10 DES items (12, 14, 15, 16, 17, 18, 20, 22, 23, and 24). Hence, for the current study, only the subscale Absorption was used (DES-AB), which reflects a higher degree of dissociative experiences characterized by absorption and imaginative involvement (e.g., “Some people have the experience of not being sure whether things that they remember happening really did happen or whether they just dreamed them”). The total score on the DES-AB is determined by calculating the average score for all items.
Inferential Confusion Questionnaire–Expanded Version (ICQ-EV)
The ICQ-EV 19 is a 30-item questionnaire based on the original version of the Inferential Confusion Questionnaire. 20 The total score represents a tendency to confuse reality with imagination, including a distrust of the senses and a tendency to easily get absorbed in the imagination. The ICQ-EV has strong psychometric qualities with a high reliability (α = 0.96) and validity.
Beck Depression Inventory II (BDI)
The BDI 21 is a 21-item measure that assesses the severity of depressive symptoms experienced by respondents during the previous 2 weeks. The BDI is highly reliable and valid (α = 0.92).
Beck Anxiety Questionnaire (BAI)
The BAI 22 is a 21-item anxiety symptom checklist on a 0 to 3 scale. The instrument shows high internal consistency (α = 0.91), good test–retest reliability (r = 0.75), moderate convergent validity (r = 0.51), and good discriminant validity (r = 0.25).
Procedure
At the beginning of the experiment, participants were asked to fill in the consent form and complete the entire battery of questionnaires. This included a measurement of sense of presence in objective reality during the last 5 minutes (AIPQ). Upon completion of the first battery of questionnaires, participants were instructed to explore the virtual environment at will for the next 15 minutes. To enhance immersion, participants were asked to note the number of people and cars encountered in the VR environment.
Following 15 minutes of exploring the VR environment, participants were removed from the environment and asked to fill in the AIPQ with the instructions pertaining to the VR environment (e.g., how he or she felt during the last 5 minutes while inside the VR environment). Once the AIPQ was completed, participants were asked to explore the VR environment once more for another 10 minutes. Therefore, in total, each participant spent 25 minutes in the VR environment, which was considered sufficient time for immersion into a VR environment without triggering confounding factors such as cybersickness.
Once the last 10 minutes of exploration of the VR environment was completed, participants were asked to stay in the room for 5 minutes before completing the post-questionnaires (CDS-S and AIPQ). During post-measurement, the AIPQ was administered to measure presence in objective reality for the last 5 minutes. The participant was then debriefed and given an explanation of the study's purpose.
Material
The VR environments were displayed using a computer with Windows 2000 (Pentium III, 4.2 GHz, 1 GB of RAM, with a nVidia GeForce4 Ti 4200 128 MB), anIntertrax2 motion tracker from Intersense (USB model, 3DOF, update rate 256 Hz), an I-Glass SVGA head-mounted display by IO-Display (800 × 600, 26° FoV diagonal), and a Gyration wireless mouse. The VR environments were created using a 3D game editor (see
Results
Means and standard deviations
Means and standard deviations of the administered questionnaires before exposure to a VR environment are shown in Table 1.
Baseline intercorrelations between the questionnaires
To provide further insight into the relationships among the various constructs and to better interpret the results of the experimental manipulation, we calculated the intercorrelations among the measures in the total sample (n = 30).
Most of the questionnaires measuring imaginative processes were strongly related to each other (Table 2). While the magnitude of correlations must be interpreted carefully due to the small sample size, this result is not surprising. To some extent, all the questionnaires relate to absorption or imaginative involvement. In particular, immersion tendencies, as measured by the ITQ, were strongly related to dissociative experiences characterized by absorption as well as feelings of DP/DR, as measured by the CDQ. Likewise, a tendency to confuse the imagination with reality, as measured by the ICQ-EV, was significantly related to most other imaginative measures. Sense of presence in objective reality related most strongly to depression, as measured by the BDI, and related moderately to feelings of DP/DR as measured by the CDQ. However, sense of presence did not relate to any of the measures such as the ICQ-EV, the ITQ, and the DES-AB. Most of the other measures related to general distress, as measured by the BAI and BDI. However, a tendency to become more easily immersed, as measured by the ITQ, was not significantly related to the BAI and BDI.
Note. *p < 0.05; **p < 0.01; ***p < 0.001; BDI, Beck Depression Inventory; BAI, Beck Anxiety Questionnaire, ICQ-EV, Inferential Confusion Questionnaire-Expanded Version; CDS-T, Cambridge Depersonalisation Scale-Trait Version; DES-AB, Dissociation Experiences Scale-Absorption Subscale; AIPQ, Adapted Igroup Presence Questionnaire; CDS-S, Depersonalisation Scale-Trait Version.
Effects of VR on DP/DR
The effects of VR on symptoms of DP/DR (as measured by the CDS-S) are shown in Figure 1(A). Paired samples t test revealed a significant difference between pre- and post-measures of symptoms of DP/DR: t(1, 29) = 3.03; p = 0.003, one-tailed. Overall, there was a significant increase in symptoms of DP/DR as the result of exposure to a virtual environment (4.9–14.5%).

(
To investigate the effects of VR in subgroups, participants were divided into high and low DP/DR subgroups on the basis of preexisting trait levels of DP/DR using the median score (11.69) of the CDS-T. The effects of VR for these subgroups on symptoms of DP/DR, as measured by the CDS-S, are shown in Figure 1(B). Repeated measures of variance revealed a significant interaction effect: F(1, 28) = 3.85, p = 0.03, one-tailed; η2 = 0.12; observed power = 0.47). Those with higher initial levels of symptoms of DP/DR showed a greater increase in state symptoms (Mpre = 89.8, SD = 147.2; Mpost = 245.8, SD = 318.9) than those with lower initial levels of symptoms of DP/DR (Mpre = 7.9, SD = 15.1; Mpost = 44.7, SD = 75.3).
Effects of VR on sense of presence
For the total sample, level of presence before, during, and after exposure to VR is represented in Figure 2. Level of presence in VR was significantly lower than in objective reality: t(1, 29) = 6.26 (1, 29); p < 0.001, one-tailed. Participants felt considerably less present in the virtual environment than they did in actual objective reality. Immediately after exposure to the VR environment, however, participants did not reach the same level of presence in objective reality as they had before: t(1, 29) = 3.64; p < 0.001, one-tailed).
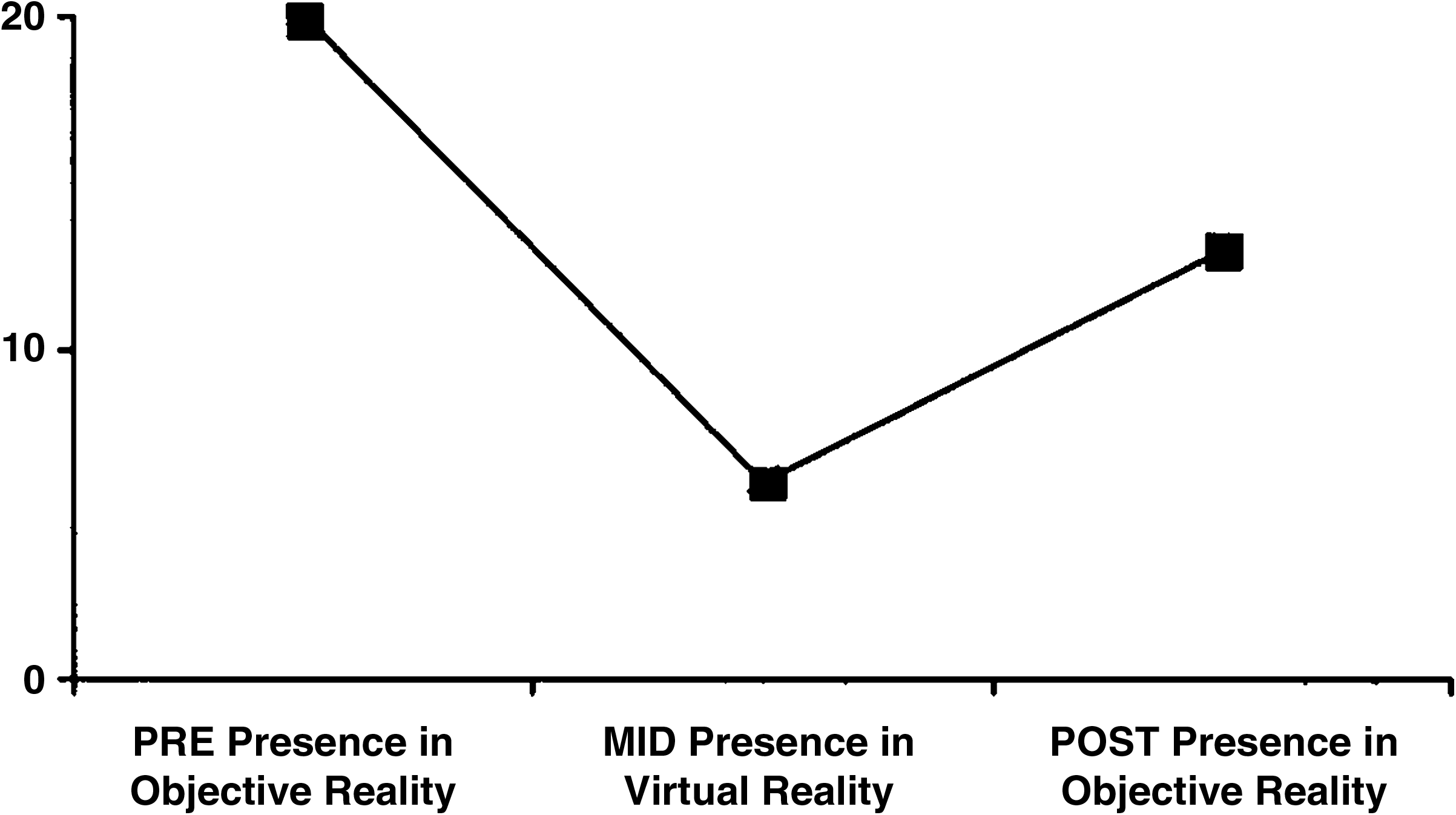
Effect of virtual reality on presence (AIPQ) in the total sample (n = 30).
In addition, repeated measures of variance showed that both subgroups (low and high on symptoms of DP/DR) felt considerably less present in objective reality after exposure to VR: F(1, 28) = 38.09; p < 0.001, one-tailed; η2 = 0.58; observed power = 1.00. However, there was no significant interaction effect between the groups when comparing preexisting levels of presence in objective reality with levels of presence in VR: F(1, 28) = 0.04; p < 0.42, one-tailed; η2 = 0.00; observed power = 0.05. In addition, when comparing the levels of presence in objective reality before and after VR, both the group high on symptoms of DP/DR (Mpre = 17.9, SD = 6.8; Mpost = 8.5, SD = 12.2) and the group low on symptoms of DP/DR (Mpre = 22.2, SD = 4.4; Mpost = 16.7, SD = 12.1) showed a decrease in sense of presence in objective reality: F(1, 28) = 13.15; p < 0.001, one-tailed; η2 = 0.32; observed power = 0.94. However, neither group showed a significantly greater reduction in level of presence than the other: F(1, 28) = 0.86; p < 0.18, one-tailed; η2 = 0.03; observed power = 0.15.
Correlates of change in presence and dissociative experience
What are the main variables that relate to change in symptoms of DP/DR symptoms and change in presence in objective reality as the result of an immersion in VR? To answer this question, we calculated the relationship between change in symptoms of DP/DR and level of presence in objective reality with all of the other measures. Results showed that change in symptoms of DP/DR due to VR exposure, as measured by the CDQ-S, was most strongly related to preexisting levels of DP/DR as measured by the trait version of the CSQ (r = 0.71; p < 0.001, two-tailed). Change in symptoms of DP/DR was also significantly related to the DES-AB (r = 0.52; p < 0.01, two-tailed). Immersive tendencies, as measured by the ITQ, were also significantly related to change in symptoms of DP/DR (r = 0.42; p < 0.05, two-tailed). In addition, change in symptoms of DP/DR was significantly related to a tendency to absorb oneself in imaginary possibilities, as measured by the ICQ (r = 0.45; p < 0.05, two-tailed). No significant relationship was observed with preexisting mood states as measured by the BAI (r = 0.33; p = 0.08) and BDI (r = 0.29; p < 0.13). Finally, change in symptoms of DP/DR was quite strongly related to change in presence in objective reality before and after immersion in VR (r = −0.58; p < 0.001, two-tailed). The greater the increase in symptoms of DP/DR, the greater the decrease in one's sense of presence in objective reality. Change in presence was not related to any of the other variables.
Discussion
The current study used an innovative experimental approach to investigate the effects of VR on dissociation experience and sense of presence in objective reality. Dissociative symptoms were measured before and after exposure to a VR environment, and results showed an increase in symptoms of DP/DR following VR exposure. In particular, those with initial higher levels of dissociative symptoms showed a greater increase in dissociative symptoms following exposure to VR than did those with lower levels of dissociative symptoms. Sense of presence in objective reality also decreased as the result of exposure to VR. However, this time, preexisting levels of DP/DR did not mitigate the effects of VR on level of presence.
The current results shed light on various imaginative factors involved in the production of dissociative symptoms. They showed that the feeling of presence in a virtual environment, which implies detachment from objective reality, may temporarily compromise one's connection with outer, objective reality. A tendency toward immersion or absorption, as measured by several different scales, related significantly to level of change in dissociative symptoms as the result of VR. The current results provide support for the notion that dissociative symptoms can be triggered through discontinuity in perceptual environments (in this case, from VR to objective reality), especially among those prone to experiencing dissociative symptoms. 4 Increasing the person's ability to tolerate perceptual discontinuities and adopting a less rigid stance toward perception has been proposed as a treatment target for those with DP/DR. 3
However, results suggest that the processes that increase dissociative symptoms as the result of a VR immersion may not be just pathological. As noted earlier, dissociative experiences lie on a continuum and may refer to completely normal imaginative processes like daydreaming. The effects of VR on dissociative symptoms were not in the clinical range or even within subclinical levels of dissociative experiences. The effects observed in the current study may be similar to spending several hours working at a computer and temporarily feeling more detached from objective reality than usual. It appears likely that the effects of exposure to VR disappear rapidly following subsequent immersion into objective reality. In addition, the dissociative effect itself may be dependent on the duration of VR exposure. Future studies need to shed light on the duration of the effect by following up with participants after VR exposure.
Nonetheless, it is possible that prolonged periods of discontinuity in objective perception may have harmful effects in vulnerable individuals. There are reports in popular media on Internet and computer game addiction being associated with neglect and suicide, sometimes inexplicably so.23,24 Of course, these anecdotal reports await further investigation, but the current findings may have bearing on such incidences if exposure to highly absorbing experiences such as Internet activity lead to a sense of detachment, a lowered sense of presence, and potentially an increase in depressive feelings. 25
Another potential implication of the current results lies in the use of VR environments to treat anxiety disorders with gradual exposure. 26 Those with higher preexisting levels of dissociative symptoms appeared to be more vulnerable to increases in symptoms of DP/DR as the result of VR. While the magnitude of these effects are unclear and may last for only a short duration after exposure to VR, it would be wise to take those results into consideration when using VR immersions with people who have preexisting clinical levels of dissociation. Alternatively, a controlled increase in symptoms of DP/DR could be viewed as a potential avenue for therapy, including the use of VR in exposing the individual to transient symptoms of DP/DR and correcting catastrophic misinterpretations of symptoms through cognitive-behavior therapy. 6
One limitation of the current study is the use of a nonclinical sample and a relatively small sample size. The current results provide only a preliminary account of the effects of VR on dissociative experiences and sense of presence in objective reality. In particular, the effects of VR on dissociative experiences appear to be exacerbated by higher preexisting levels of dissociation and the individual's propensity for immersion. Sense of presence in objective reality seems to suffer as well. Future research should establish the exact relationships among these variables as well as the exact clinical implications of the current findings.
Footnotes
Acknowledgments
The study was supported with a Fellowship Award from the Fonds de la Recherche en Santé du Quebec (FRSQ) to the first author and Grant No. MOP67059 from the Canadian Institutes of Health Research (CIHR) to the second author.
Disclosure Statement
No competing financial interests exist.