
Abstract
Abstract
Initial studies with healthy subjects and individuals with high risk for psychosis have suggested that virtual reality (VR) environments may be used to investigate social and psychological mechanisms of psychosis. One small study reported that VR can safely be used in individuals with current persecutory delusions. The present pilot study investigated the feasibility and potential negative side effects of exposure to different virtual social risk environments in patients with first episode psychosis and in healthy controls. Seventeen patients with first episode psychosis (FEP) and 24 healthy control subjects (HC) participated in four virtual experiments during which they walked for 3.5–4 minutes in a virtual café, looking for avatars with digits on their clothing. The level of paranoid thoughts, as well as psychological, physiological, and behavioral correlates of paranoid thoughts, were measured in different virtual social risk environments, manipulating two factors: population density and ethnicity of avatars. FEP and HC frequently had paranoid thoughts about avatars. Paranoia in the real world correlated strongly with paranoid thoughts about avatars in virtual environments (Spearman's ρ=0.67 and 0.54 in FEP and HC respectively, p<0.01). FEP kept a smaller distance to avatars than HC. In FEP, but not in HC, galvanic skin response was significantly stronger in virtual environments with avatars of other ethnicity than in the own ethnicity condition. These results suggest that VR is an acceptable and sufficiently realistic method to use in patients with first episode psychosis. VR research may help to increase our understanding of the social and psychological mechanisms of psychosis and to develop new treatment applications.
Introduction
P
The present pilot study investigated the feasibility of VR in patients with first episode psychosis and in healthy controls. We explored level of paranoid thoughts as well as psychological, physiological, and behavioral correlates of paranoid thoughts in different virtual social environments, manipulating two factors: population density and ethnicity of avatars.
Methods
Participants
Seventeen patients with first episode psychosis (FEP) were recruited from a specialist service for early psychosis in The Hague. Inclusion criteria for the study were: aged 18–40 years and a DSM IV diagnosis of schizophrenia, schizophreniform disorder, schizoaffective disorder, brief psychotic disorder, delusional disorder, or psychotic disorder not otherwise specified. Twenty-four healthy control subjects (HC) were recruited from Delft University of Technology staff and students. Written informed consent was obtained from all participants.
Virtual reality setting
The virtual environment was a café with an indoor and an outdoor part, adjacent to a shopping street, built by CleVR. Participants could navigate in the virtual environment, using a Logitech Chillstream Gamepad. They wore an Emagin Z800 3D Visor with a resolution of SVGA 800×600 24 bit, with 40° diagonal field of view, and built-in 3DOF tracker. Avatars walked in and out, chatted, and had drinks while sitting or standing at a table. Café background noises were played. The avatars were programmed to exhibit neutral behavior. They glanced up when participants approached them, and if participants blocked their way, avatars politely asked them to move aside.
Experiments
To engage the participants with the avatars, the system randomly assigned a number to five of the avatars that was visible on their clothing. Participants were instructed to find the numbered avatars and to memorize the numbers. This task had to be completed in three-and-half (HC) to four (FEP) minutes, after which the experiment ended. Patients were allowed more time because psychosis is associated with reduced cognitive performance.
The number of avatars in the café and the ethnic appearance of the avatars was manipulated. Both factors had two options. The ethnic appearance could be either mainly (95%) white European or mainly (75%) North-African (own or other ethnicity, depending on the ethnicity of the participant); the number of avatars could be either between seven and nine (low density) or between 34 and 38 (high density) avatars.
All subjects participated in four conditions: (a) own ethnicity/low population density, (b) other ethnicity/low population density, (c) own ethnicity/high population density, and (d) other ethnicity/high population density. All FEP started with own/low condition; the other experimental conditions were randomized for order of condition. A counterbalanced experimental design was used for the HC. While these designs are slightly different, both approaches were intended to prevent order effects.
Measurements
Before experiments
Baseline measures included the Green Paranoid Thoughts Scale (GPTS), 11 the Social Interaction Anxiety Scale (SIAS), 12 the Davos Assessment of Cognitive Biases Scale (DACOBS), 13 the Self-Esteem Rating Scale (SERS), 14 and the Simulator Sickness Questionnaire (SSQ). 15 Before the experiments, neutral physiological data were collected with a Mobi8 from TMSi with Xpod Oximeter. Heart rate (HR) and galvanic skin response (GSR) sensor were measured using two finger electrodes.
During and between experiments
During experiments, besides HR and GSR data, position of participants in VR relative to avatars was automatically recorded three times per second. After each experiment, paranoid ideations toward avatars were assessed with the State Social Paranoia Scale (SSPS). 16 Furthermore, subjective experience of distress was measured with visual analogue scales, ranging from 1 to 10.
After experiments
The SSQ was administered again in order to measure cyber sickness. The Igroup Presence Questionnaire (IPQ) 17 was used to explore sense of presence in the virtual environment.
Statistical analyses
Nonparametric tests were used for statistical analyses, or, in cases with two or more independent variables, linear mixed model analyses on aligned rank transformed data. 18 Real world symptoms at baseline were compared between FEP and HC with Mann–Whitney U tests for independent samples. In order to investigate whether real world experiences corresponded to VR experiences, nonparametric Spearman coefficients were calculated for correlations between degree of paranoid thoughts (and correlates of paranoia, such as social anxiety and cognitive biases) at baseline and paranoid thoughts about avatars in VR. Physiological and behavioral responses to virtual environments were explored by comparing GSR, HR, and distance to avatars, averaged over all virtual experiments, between FEP and HC. The GSR in micro Siemens (μS) values (δ) were set against the mean GSR value of the neutral (β) phase ((δ−β)/β), whereby an increase indicates an increase in sweating. Finally, psychological, physiological, and behavioral responses of participants were compared across four different virtual social environments. Since the virtual experiments combined ethnicity and population density conditions (e.g., other ethnicity and high, or own ethnicity and low), results for ethnicity conditions were averaged over population density conditions (low and high), and results for population density conditions were averaged over ethnic density conditions (own and other).
Results
Sociodemographic characteristics of the participants are shown in Table 1.
Note. FEP, first episode psychosis; HC, healthy control subjects.
Before the experiments, mean degree of paranoid thoughts was 66.8 (SD=44.4) in FEP and 41.7 (SD=6.8) in HC, Mann–Whitney U test, p=0.482. FEP had significantly more cognitive biases, higher subjective distress, and lower self-esteem than HC (Table 2).
Note. aSpearman nonparametric correlation coefficients between real world experiences and paranoid thoughts in VR. bMann–Whitney U test for independent samples, FEP compared to HC.
p<0.05; **p<0.01.
FEP, first episode psychosis; HC, healthy control subjects.
Total SSPS scores ranged from 40 to 96 in HC (40 indicates not a single paranoid thought during any of the four experiments; M=53.1; SD=17.1) and 40 to 181 in FEP (M=67.5; SD=44.1). Table 2 shows that baseline scores of paranoia, social anxiety, and cognitive biases in the real world correlated strongly and statistically significantly with degree of paranoid thoughts in VR.
Paranoid thoughts about avatars varied slightly with virtual condition (Fig. 1), but within-subject differences across conditions were not statistically significant, neither in the FEP nor in the HC condition.
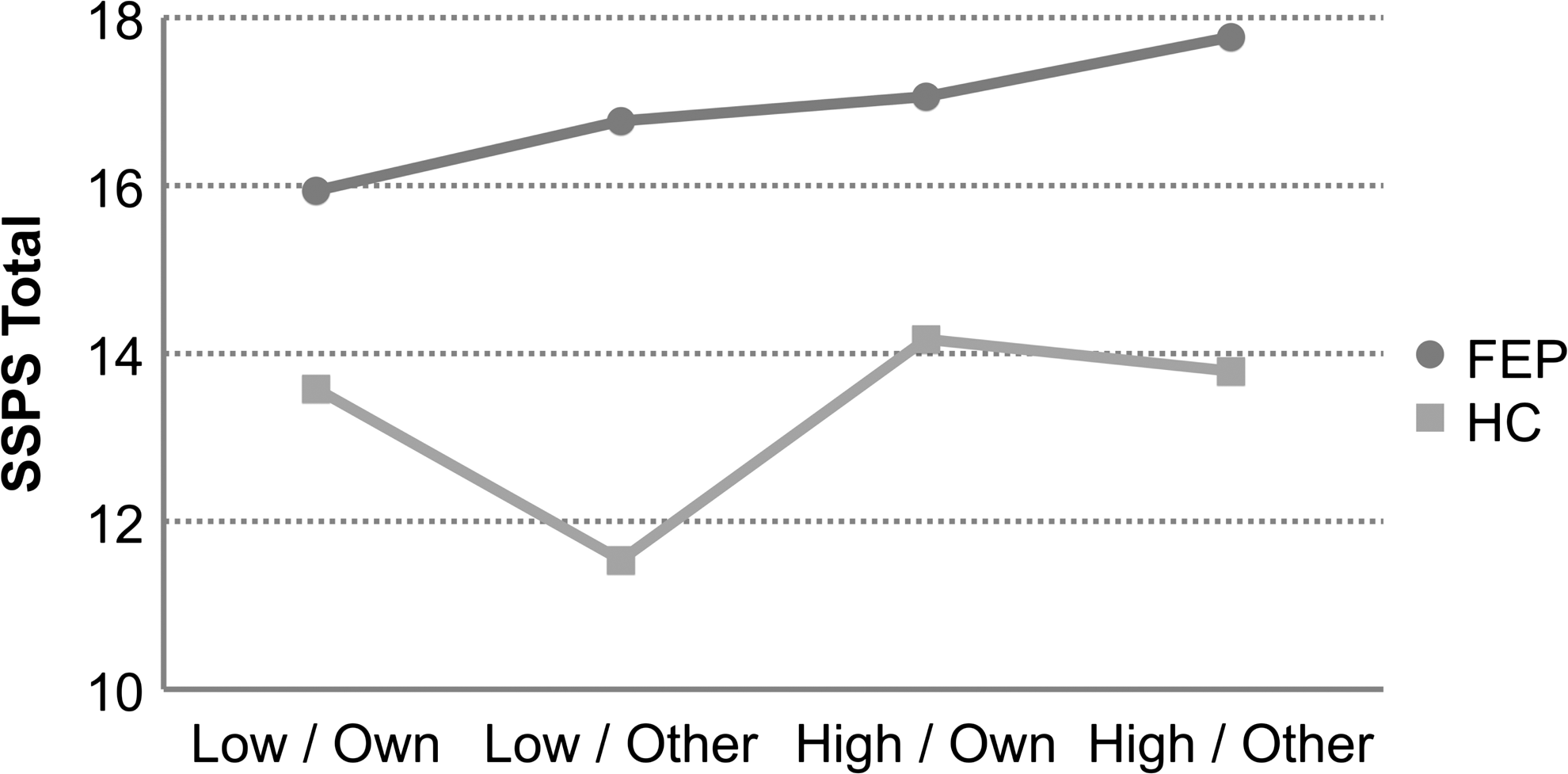
Paranoid thoughts about avatars in different virtual social environments: patients with first episode psychosis (FEP), and healthy control subjects (HC).
Differences between FEP and HC in physiological measures, averaged over all virtual conditions, were not statistically significant (GSR: 89.5 (SD=151.6) vs. 66.2 (SD=58.6) and mean HR: 87.4 (SD=16.2) vs. 82.9 (SD=11.0); Table 3). Heart rate did not vary much across virtual conditions. With regard to GSR, there was a two-way interaction effect of ethnic density and case-control status, df=1.32, F=9.824, p=0.004. In FEP, GSR was significantly higher in the other ethnicity (M=114.1; SD=156.8) than in the own ethnicity condition (M=64.9; SD=155.8), whereas this was not the case in HC.
Note. aAveraged over all experiments. bMissing data galvanic skin response for six FEP (n=11) and 1 HC (n=23). cp<0.05, Mann–Whitney U test.
FEP, first episode psychosis; HC, healthy control subjects.
Averaged over all conditions, HC kept significantly more distance to avatars than FEP: 1.29 meters (SD=0.06) versus 1.25 meters (SD=0.05), df=1.39, F=4.38, p=0.043. There was an interaction effect between ethnic density and population density. Participants kept more distance to avatars in the other ethnicity environment, but only if in the low population density condition, df=1.39, F=5.08, p=0.030.
Symptoms of simulator sickness were low. They slightly increased during experiments but were not statistically significant between pre and post measurement. The mean SSQ score was significantly higher in FEP than in HC before but not after the experiments. Sense of presence in VR did not differ significantly between FEP and HC. The mean total IPQ score was 41.53 (SD=12.61) in cases and 40.75 (SD=15.73) in controls, Mann–Whitney U Test=179, Z=−.029, p=0.977.
Discussion
Main results
In this pilot study of VR experiments linking social environment to psychosis, we have found that patients with FEP as well as HC frequently had paranoid thoughts about neutral virtual characters. Symptoms and correlates of paranoia in the real world strongly correlated to experiences in virtual environments, indicating that VR can be used for environmental studies of psychosis. It was feasible to expose FEP and HC to different virtual social environments. FEP kept a smaller distance to avatars than HC did. In FEP, but not in HC, galvanic skin response was significantly higher in virtual environments with other ethnicity avatars than in the own ethnicity condition.
Methodological and technical considerations
The pilot study was conducted in order to investigate the feasibility of virtual experiments in psychosis, and to explore responses of participants to different virtual environments. The main limitation is the small sample size, allowing only exploratory analyses. Based on these results, a larger study will be conducted.
Experience with use of physiological measures in VR is limited. Heart rate and skin conductance are commonly used in psychological and psychiatric research to assess an individual's emotional arousal and vulnerability to stress, as well as in studies of psychosis (liability).19,20 In our experiments, heart rate did not vary substantially across conditions. We used mean heart rate per condition, but variation may be detected only when smaller time windows before and after marked stressors are analyzed.
Participants were instructed to find and memorize numbers on the clothing of avatars. Because patients with psychosis often have cognitive deficits, they were given more time to complete the task. Still, since it may have taken a substantial part of their cognitive abilities to remember the digits correctly, some participants are likely to have paid less attention to the behavior of avatars and the virtual environment. This may explain why patients kept a slightly smaller distance to avatars than HC subjects.
A fully counterbalanced experimental design was used for the HC. For FEP, a crossover design was used in which the order of experiments was random except for the first. As a safety precaution, all patients started with the low population density and high ethnic density condition because this was considered the lowest social stress environment. Before the first experiment, they had some time in VR to get used to the virtual environment and the equipment, but the subjective distress and physiological arousal during the first experiment may still have been influenced by unfamiliarity with VR.
Previous research
There are few previous studies of VR in psychosis. One study exposed 20 patients with a current paranoid delusion and 20 control subjects to a four-minute ride in a VR underground train containing neutral characters. 9 The results were similar to our findings. A high proportion of the patients (65%) had persecutory thinking about the avatars. The VR experience did not raise levels of anxiety or symptoms of simulator sickness. Another study, using the same VR environment, reported that in 21 individuals with an at-risk mental state for psychosis, persecutory ideation in VR was predicted by higher levels of trait paranoia, anxiety, stress, immersion in VR, perseveration, and interpersonal sensitivity. 10 Initial findings from South Korea suggest that VR scenarios may be useful in evaluating social skills and emotions arising from social interactions in patients with schizophrenia.21,22
Conclusion
VR seems an acceptable and sufficiently realistic method to use in patients with first episode psychosis. It offers a unique way to expose individuals to controlled social environments. VR research may help to increase our understanding of the social and psychological mechanisms of psychosis and to develop new treatment applications, but larger studies are needed.
Footnotes
Acknowledgment
This study was supported by a grant from the Parnassia Psychiatric Institute.
Author Disclosure Statement
No competing financial interests exist.