
Abstract
Abstract
The study examined whether complementary therapy using robotic companions as social agents reduced pain and emotional anxiety in pediatric patients. A total of 18 patients, aged 6–16, and 18 parents participated in the study. The study explored whether the use of robotic animals as companion animals could reduce pain and emotional anxiety in patients and their parents. The study identified when robot-assisted therapy was most effective (alone or together with parent). The study hypothesized that engaging in robot-assisted therapy together would enhance parents' perspective taking, thereby triggering strong empathic resonance and parental modeling to bolster the children's coping skills. The robotic companion was more successful in decreasing pain and negative emotional traits when children and parents were engaged together with the robotic companion. The parent's ability to acknowledge the patient's pain accurately through robot-assisted therapy seemed to reduce pain and emotional anxiety.
Introduction
In recent years, many therapists have added animal-assisted therapy to their traditional approaches. Companion animals have demonstrated positive effects in both physiological measures (e.g., heart rate, blood pressure, and stress levels) and psychological measures (e.g., improvement in emotional well-being).3–5 The use of animals for complementary treatment has been linked to positive benefits in both children and adults.6,7 Studies have confirmed that even short visits with animals provided positive benefits, reducing patients' pain and emotional anxiety. 8 However, some patients' situations restrict complementary therapy using animals (e.g., isolation). If similar benefits can be gained from robots, they may be a promising, low-maintenance alternative without the worries of allergies, bites, scratches, and pet loss. When elderly patients suffering from dementia interacted with Paro for a period of time, their emotional well-being and depression improved.9,10 Later, Wada et al. 11 found that Paro facilitated human interactions rather than replacing them. Also, urine tests indicated that patients' stress levels were decreased after they interacted with Paro.
Humans seem to have an innate interest in lifelike artifacts, and such machines seem to evoke friendly feelings in humans. 11 This study examined whether robotic companion animals could reduce pain and emotional anxiety in patients and their parents.
A greater challenge may be to identify conditions in which robots have a positive influence on human behavior and to identify the mechanisms that elicit such response. Past studies have found that both live animal companions and robotic companions provide psychological benefit and serve as effective tools for socialization. 12 Thus, the study examined the conditions in which robot-assisted therapy may be most effective. Would patients gain greater benefit from interacting with the robot alone or with a parent? Children find ways to cope with fear by recalling how adults respond to a similar situation, 13 looking to adults, learning by observing, or recalling the examples of their parents. 14 In doing so, children often develop a coping response, even if the situation seems incomprehensible or uncontrollable to them. Since children use adults' responses to guide their own behavior, the study hypothesized that engaging together in robot-assisted therapy would help the parent understand the child's situation better and trigger strong empathic resonance and parental modeling in the child. This should help the children develop the coping skills that they need to reduce pain and emotional anxiety.
Materials and Methods
Participants
Eighteen pediatric patients (aged 6–16) and 18 parents participated in the study. The participants were admitted to a children's hospital in Palo Alto, CA, for different pathological symptoms. All participants were under the care of the hospital's management team. The study focused on female participants and caregivers for several reasons. When examining the literature on children and medical-related fears, several empirical findings15–18 suggested significant gender differences in children between the ages of 6 and 15 years. 15 Their findings showed that female children were more susceptible to medical-related fears compared to male children. Due to the limited time allowed in the hospital ward, and the similar age range of our participants, the decision was made to focus on female pediatric patients who, according to the literature, were more likely to experience stronger medical fear. Other additional reasons include controlling for pairs of the same gender (patient and caregiver) and having a reasonable sample size.
Procedure
The hospital staff verified that participating patients met the inclusion criteria. After obtaining the physician's permission, interested patients and parents were referred to the study, which was conducted under the guidance of a child life therapist and the pediatric pain management team.
The study consisted of two conditions: “alone” or “together with parent.” All participants completed a pretest form (i.e., pain rating scale and anxiety questionnaire). The patient and her parent were paired to form 18 groups. Each group was assigned randomly to one of the two conditions. In the “alone” condition, the patient was introduced to the seal robot, Paro, and instructed how to engage with the robot (e.g., pet, hold, talk to). When the patient felt comfortable, the experimenter left the room (Fig. 1). The parent was away from the patient and engaged in other tasks to minimize her interactions with the patient. In the “together with parent” condition, the parent was asked to sit by the patient, and they were introduced to Paro and given instructions on how to interact with it (e.g., pet, hold, talk to). The patient and parent were asked to take turns interacting with Paro, and the experimenter left the room (Fig. 2).
Patient in the “alone” condition.

Patient and parent in the “together with parent” condition.
In both conditions, the experimenter returned after 30 minutes, and the patient and parent completed the posttest form (FACES Pain Rating Scale and the anxiety questionnaire). In the “alone” condition, the patient was engaged with Paro for 30 minutes. In the “together with parent” condition, the patient and parent took turns interacting with Paro for 30 minutes.
Materials and measures
Paro is categorized as a class II medical device in the United States, and has been used in many pediatric hospitals and elder-care facilities in the United States and Europe (Fig. 3). Paro received Guinness World Record Certification in 2002 19 for “World's Most Therapeutic Robot.” Paro consists of sophisticated sensors, speech recognition, autonomous behavior, and reactive behavior from tactile sensing. The study consisted of two measures: (a) the Wong–Baker FACES Pain Rating Scale, 20 which asked participants to rate the extent to which they were experiencing pain at that time (on a scale of 1 to 10), and (b) an anxiety questionnaire that consisted of 11 questions on anxiety-related positive and negative emotions.

Robotic seal, Paro, a class II medical device.
For the FACES Pain Rating Scale, the patient completed the form by placing a check mark above the picture of the facial expression that best described her current pain. If the patient could not decide between two adjoining facial expressions, she placed the check mark between the two. The parent completed two forms: one on her level of empathetic pain as she watched her child, and one concerning her perception of her daughter's pain (perspective taking). Both the patient and the parent completed the FACES Pain Rating Scale twice, at pretest and posttest.
The anxiety questionnaire covered six positive emotional traits and five negative emotional traits. To determine differences between patient and parent, the items in the questionnaire were emotional trait items that overlapped between the two anxiety inventories, that is, the State–Trait Anxiety Inventory for Children (STAIC) 21 and State–Trait Anxiety Inventory (STAI), the adult version of the inventory. 22 Parents were asked to rate their emotional state on a scale of 1–4 (i.e., almost never, sometimes, often, and almost always, respectively). Initially the study found that younger children (e.g., 5–6 years old) had trouble reading and relating to the terms used in the questionnaire (e.g., jittery, pleasant). Therefore, the anxiety questionnaire was administered only to children in the mid-range of ages (9–10 years old), to older children (15–16 years old), and their parents. Patients over 9 years of age (n=12) and their parents (n=12) completed the anxiety questionnaire twice, at pretest and posttest.
Results
Reducing pain in patients and parents
A paired sample t test was conducted to compare the patient's mean scores for the FACES Pain Rating Scale from pretest to posttest (Fig. 4). In the “together with parent” condition, the pain rating decreased significantly from the pretest (M=4.89, SD=1.54) to posttest (M=2.78, SD=1.92) for the patients, t(8)=8.1, p<0.001. There was no difference for patients in the “alone” condition, t(8)=−0.89, p=0.397.
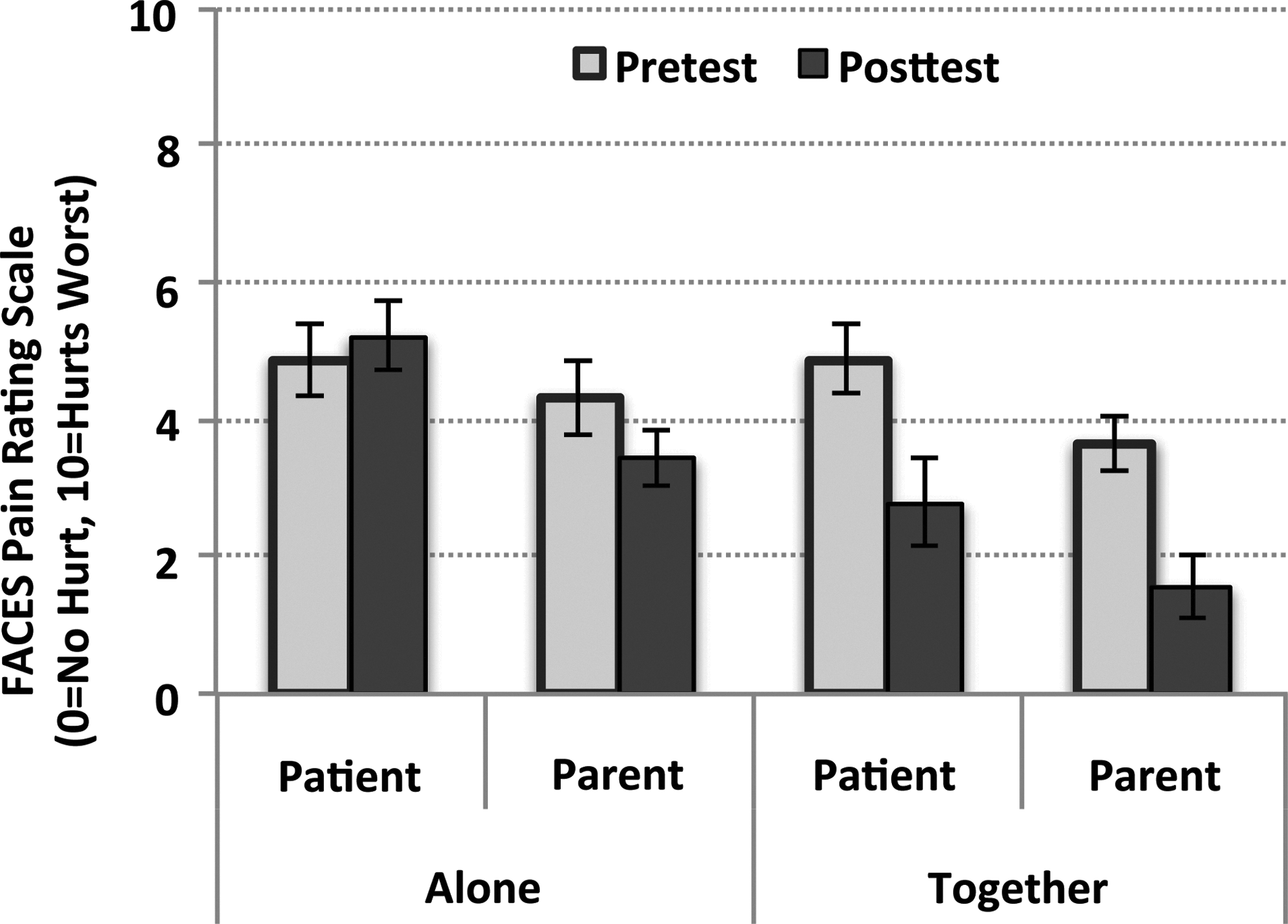
Pain rating in patients and parents across conditions.
For parents, a significant difference in pain rating was observed in both conditions, that is, “alone” condition, from pretest (M=4.33, SD=1.66) to posttest (M=3.44, SD=1.22), t(8)=3.41, p<0.01, and “together” condition, from pretest (M=3.67, SD=1.22) to posttest (M=1.56, SD=1.33), t(8)=10.54, p<0.001. The results suggested that engaging with Paro with the patient helped reduce pain, as did observing the patient as she engaged with Paro, albeit to a lesser degree.
In the “together with patient” condition, there was a positive correlation between the patients' and the parents' FACES Pain Rating Scale at r=0.761, n=18, p<0.01. In the “together” condition, when the parent's pain rating decreased, so did the patient's pain rating, possibly as a result of parental modeling. There was no correlation in the “alone” condition, r=0.420, n=18, p=0.083.
Parent's perception of the extent to which her child is experiencing pain
An independent sample t test was conducted to compare the “patient's rating of pain” to “parent's perception of her child's [patient's] pain” to determine whether the parent could acknowledge her child's state of pain accurately (Fig. 5). No differences were seen on the pretest, but significant differences appeared on the posttest between the patient's rating of pain, and the parent's perception of their child's pain. In the “together with parent” condition, parents acknowledged their children's pain accurately, that is, the patients' perceptions (M=2.78, SD=1.92) and parents' perceptions (M=2.56, SD=2.24) showed no significant difference, t(16)=0.23, p=0.82. However, in the “alone” condition, there was a significant difference between the patients' perceptions (M=5.22, SD=1.48) and the parents' perceptions (M=3.44, SD=1.88), t(16)=2.23, p<0.05. Parents in the “alone” condition underestimated the level of their children's pain.
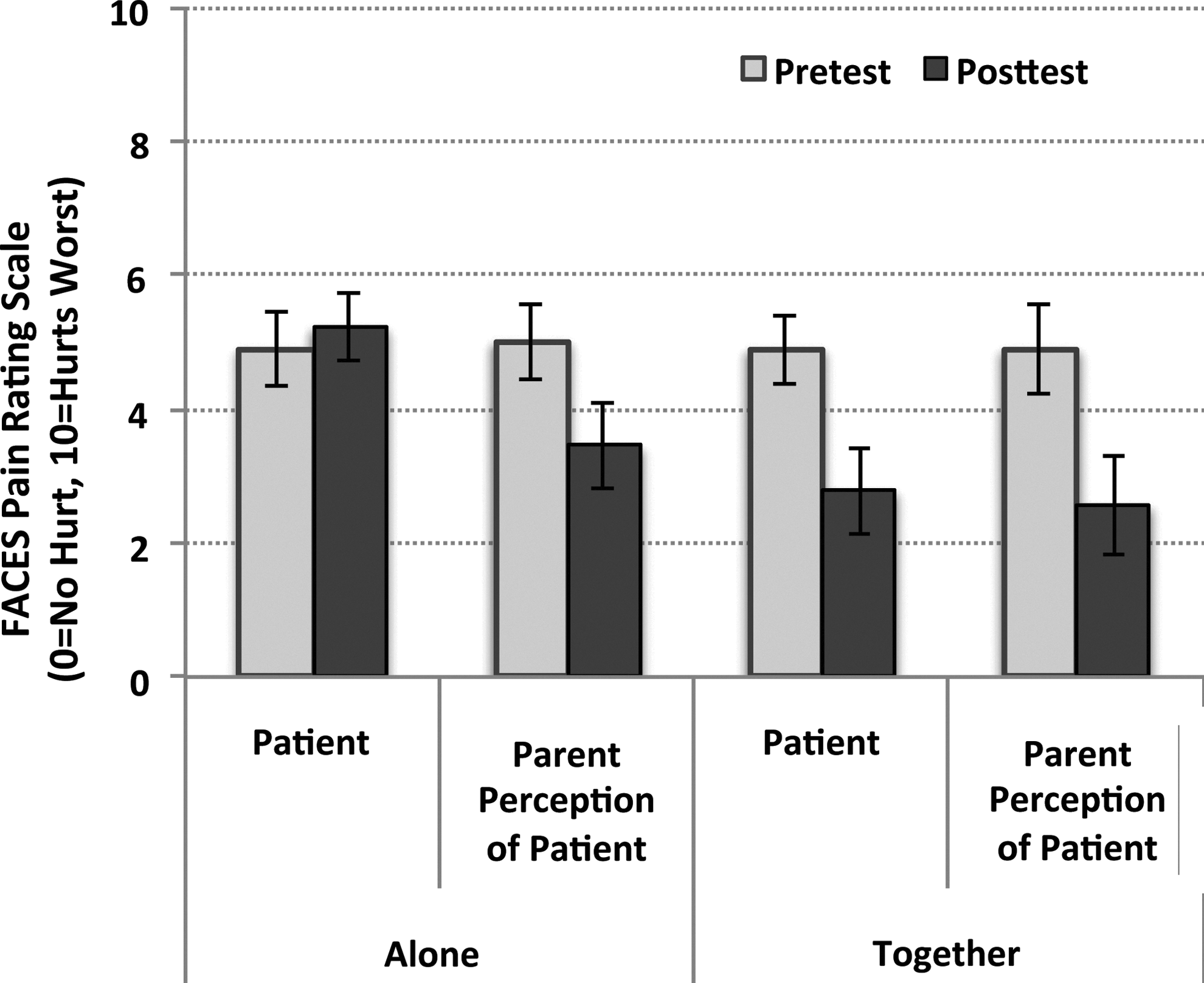
Parent's perception of patient's pain compared to the patient's own rating.
Reducing emotional anxiety in patients and parents
A paired sample t test was conducted to compare the mean scores of the anxiety questionnaire from pretest to posttest (Fig. 6). For patients in the “alone” condition, there was no difference. For patients in the “together with parent” condition, there were no differences in positive emotional traits, but there was a significant decrease in negative emotional traits from pretest (M=2.67, SD=0.38) to posttest (M=1.64, SD=0.31), t(5)=5.86, p<0.01.
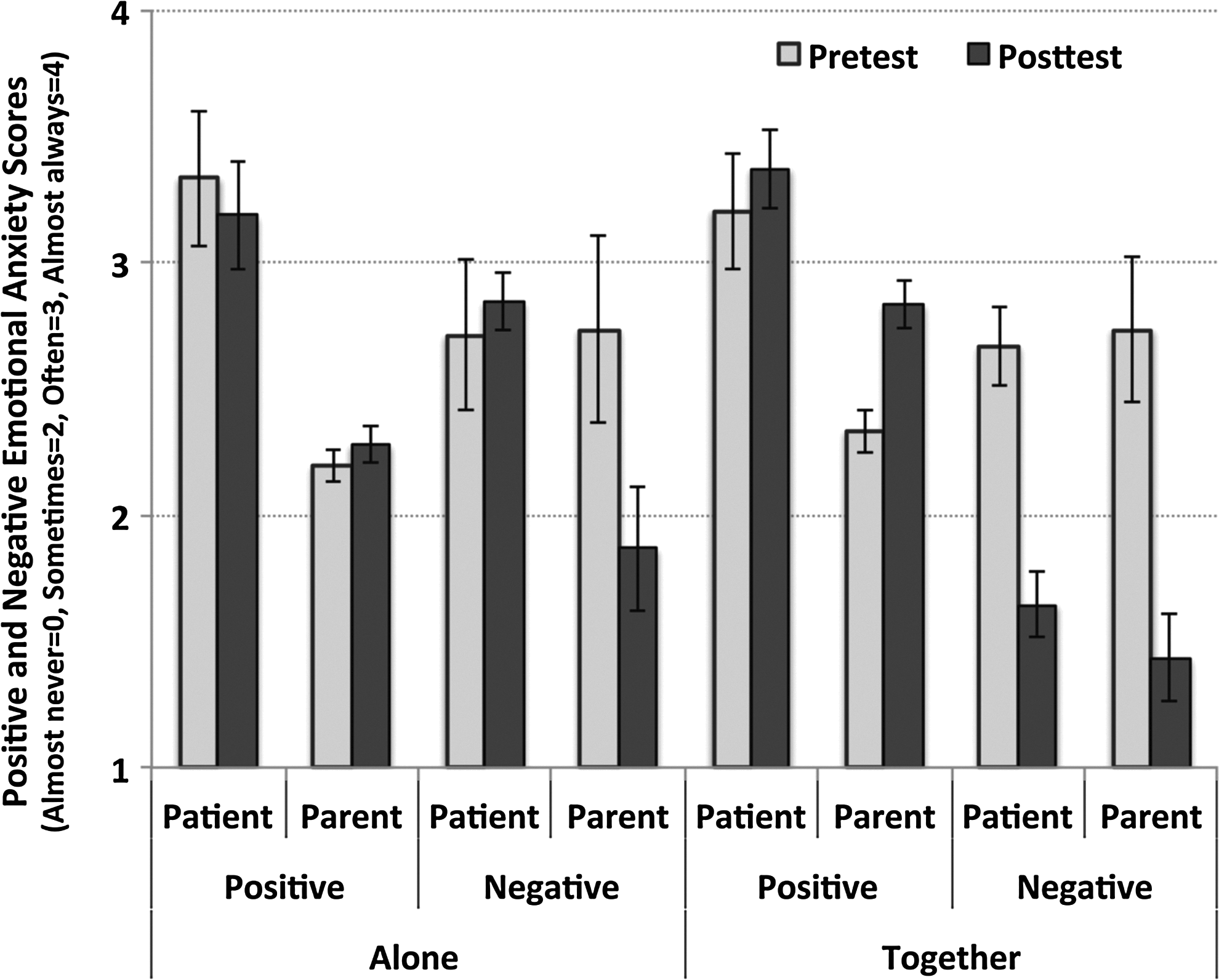
Effect of robot on the participant's positive and negative emotional anxiety scores across conditions.
For parents in the “alone” condition, there was no difference in positive emotional traits, but there was a significant decrease in negative emotional traits from pretest (M=2.73, SD=0.90) to posttest (M=1.87, SD=0.60), t(5)=3.61, p<0.05. Parents in the “together with parent” condition showed a significant increase in positive emotional traits from pretest (M=2.33, SD=0.21) to posttest (M=2.83, SD=0.24), t(5)=−8.21, p<0.001, and a significant decrease in negative emotional traits from pretest (M=2.73, SD=0.70) to posttest (M=1.43, SD=0.43), t(5)=7.05, p<0.01.
In the “alone” condition, there was a significant negative correlation between patient and parent for positive (r=−0.616, n=12, p<0.05) and negative emotional traits (r=−0.670, n=12, p<0.05); thus, when the parent's positive emotions decreased, the patient's positive emotions increased, and as the parent's negative emotions decreased, the patient's negative emotions increased. In the “together with parent” condition, there was a significant positive correlation between patient and parent for the negative emotional traits (r=0.579, n=12, p<0.05), that is, the patient's negative emotions decreased when the parent's negative emotions decreased.
Overall, the results suggested that Paro helped reduce pain and emotional anxiety when patient and parent were in complementary therapy together.
Discussion
The study found that patients who engaged with their parents with Paro showed greater reductions in pain and negative emotional anxiety than patients who interacted with Paro alone. The limited data acquired in this study preclude our addressing detailed questions concerning the mechanisms responsible for our results, but two possible underlying mechanisms are worth considering: parental modeling and perspective taking. Both appear to contribute to developing empathetic resonance between patient and parent.
When examining the origin of many pain-related beliefs in children, parents often take the role of a moderator. Studies have found that young children actively search for emotional information from their caregivers, and they use this information to appraise uncertain situations. 23 For example, Horton and Riddell 24 found that young children were more likely to study their parents' faces when getting an injection. If the parent expressed fear prior to the injection, the children also displayed greater distress on their faces.25,26 Children seem particularly prone to using parents' responses to guide their own behavior when they encounter ambiguity or experience a sense of uncertainty. By observing the parent in a particular situation, the child acquires information about that situation and about the consequences of specific actions in that situation. 27 Usually, if one shares similar experiences in pain, mirror matching occurs, and automatic resonance to another's affective state occurs. Mirror matching triggers automatic resonance to other's affective states, allowing implicit sharing of affect and empathy.28,29
Since parents may not have shared similar experiences to those of their sick children, they may find it difficult to maintain their composure and provide parental modeling in such a situation. Children's coping strategies are challenged under such uncertainty because they have no model and no strong empathetic resonance that exists between the parent and the child. The lack of direct experience may cause parents to perceive the pain their child is suffering from a different perspective from the child. Studies have shown that those who lack experience tend to overestimate or underestimate the pain of others. According to Singer, 30 lacking specific painful experiences and the emotions that come from those experiences make it difficult to empathize with someone else's pain directly. The ability to acknowledge their child's pain fully may depend on a higher level inferential process, such as “perspective taking,” which provides an alternative means for understanding another's pain and emotions in a more reflective way.31–33
Children also cope with fear by recalling how adults responded to a similar situation or by looking to adults and learning by parental modeling. 34 Children often adapt to stimuli and constitute a protective response even if the situation seems incomprehensible or uncontrollable. Research by Muris et al. 35 examined the relationship between the fearfulness of the mother and child. They found a significant positive relationship in which the children of mothers who often expressed their fears exhibited the highest levels of fear, children of mothers who never expressed their fears had the lowest levels of fear, and children of mothers who occasionally expressed fear fell somewhere in between. These findings are also supported by the broad literature on familial patterns in anxiety disorders. 36 In a similar study of children's fear of dental work, Milgrom et al. 37 found that parental modeling was one of the major predictors for children's anxiety. Results seem to imply some converging evidence for the role of modeling in the development of children's fear and anxiety.
Complementary therapy using robot companions as social agents significantly reduced the pain experienced by patients in the “together with parent” condition but not in the “alone” condition. Robotic companions also reduced the patient's negative emotional traits in the “together with parent” condition. For parents, just observing their children engage alone with the robot significantly reduced empathetic pain and decreased negative emotional traits in parents. Parents in the “together with parent” condition also experienced a significant reduction in empathetic pain and a significant difference in both negative (decreased) and positive (increased) emotional traits. In both conditions, the robot was used as a social agent to generate perspective taking through a shared common experience, and it seemed to enhance the parent's ability to empathize directly with her child. However, the two conditions differed at the level at which parents fully acknowledged their children's pain. Parents in the “together with parent” condition accurately acknowledged their children's level of pain, while parents in the “alone” condition underestimated the level of their children's pain. The inability to acknowledge their children's pain accurately may explain the negative correlation found between patients and parents on the anxiety questionnaire. In contrast, in the “together with parent” condition, when the parent's pain level decreased, so did the patient's pain level. Similarly, when the parent's negative emotions decreased, so did the patient's negative emotions. These results suggested that parental modeling had taken effect through the robotic interaction, and the children were able to use robot-assisted therapy as a way to cope with their own pain and emotional anxiety.
This study was a first attempt to see if robots could be used for facilitating social interactions, perspective taking, modeling, and learning coping skills. One limitation of our study was that there were no male pediatric patients or caregivers included. For future work, the plan is to conduct a large-scale study across multiple hospital wards (not limited to pain management). It will be interesting to see whether similar findings can be found with male pediatric patients and their caregivers, as well as adult patients. Another planned study will explore different variants of robots (e.g., other animal robots, humanoid robots) to see if there are any differences. The findings will have implications on how to design effective social robots for complementary therapy.
Animal and humanoid robots are also being designed for children in the long term hope that biologically inspired robots may eventually serve as pets and become sources of comfort and learning. Children, however, differ from adults in many ways, and relatively little research exists on how children interpret these robots, or how such advanced technologies can assist children in their learning and development. This type of research has some practical importance because the findings can tell us whether it is possible to use advanced technologies to get children to treat robots in similar ways to live pets or peers. It also has some theoretical importance because it can clarify how children come to understand artifacts. Many hope to see robots fulfill multiple roles in our lives (e.g., helpers for senior assisted living, social companions, and learning partners), and currently researchers are making exciting headway in exploring how specific features of robots when combined with specific interactive scenarios can facilitate meaningful and affective engagement. 38
The study demonstrated that engaging in robot-assisted therapy together with the patient helped the parent's perspective taking, thereby triggering strong empathetic resonance and parental modeling to bolster the patient's coping skills. The parent's ability to acknowledge the patient's pain accurately through robot-assisted therapy seemed to reduce pain and emotional anxiety.
Footnotes
Acknowledgments
The author would like to thank the participants of the study, and is grateful for all the support from her collaborators at National Institute of Advanced Industrial Science and Technology (AIST), and Stanford University, Lucile Packard Children's Hospital. Any opinions, findings, and conclusions or recommendations expressed in this material are those of the author and do not necessarily reflect the views of the collaborators.
Author Disclosure Statement
No competing financial interests exist.