
Abstract
Abstract
Individuals frequently use the Internet to search for medical information. However, for some individuals, searching for medical information on the Internet is associated with an exacerbation of health anxiety. Researchers have termed this phenomenon as cyberchondria. The present research sought to shed further light onto the phenomenology of cyberchondria. In particular, the moderating effect of intolerance of uncertainty (IU) on the relationship between the frequency of Internet searches for medical information and health anxiety was examined using a large sample of medically healthy community adults located in the United States (N=512). The purported moderating effect of IU was supported. More specifically, the relationship between the frequency of Internet searches for medical information and health anxiety grew increasingly stronger as IU increased. This moderating effect of IU was not attributable to general distress. These results suggest that IU is important for better understanding the exacerbation of health anxiety in response to Internet searches for medical information. Conceptual and therapeutic implications of these results are discussed.
Introduction
Researchers propose that reviewing medical information on the Internet is a safety behavior in which individuals attempt to gain reassurance that nothing is medically wrong.3,4 Researchers conceptualize safety behaviors associated with health anxiety as attempts to reduce discomfort surrounding uncertainty about medical problems. 6 Moreover, and pursuant to the present research, Caita-Zufferey et al. 7 found that reducing uncertainty is a core motive for searching for medical information on the Internet. Tolin et al. 8 asserted that individuals who have an intolerance of uncertainty (IU), which represents a dispositional fear of the unknown, 9 find uncertainty highly distressing and engage in safety behaviors (e.g., checking behavior) to reduce such distress.a
However, searching for medical information on the Internet has the potential to lead to greater levels of uncertainty and therefore exacerbate health anxiety for individuals with high IU. For example, multiple medical possibilities, some of which are catastrophic in nature, are typically presented in response to Internet searches of medical concerns. 2 Individuals with high IU find ambiguous situations highly distressing 10 and respond to perceived threats with elevated anxiety. 11 Further, the tendency to form catastrophic interpretations of ambiguous health information is only related to health anxiety at high IU. 12 Based on these considerations, individuals with high IU might be expected to experience increased health anxiety as a result of searching for medical information on the Internet (i.e., cyberchondria).
If this possibility is tenable, IU should moderate the relationship between the frequency of Internet searches for medical information and health anxiety. The present research examined this purported moderating effect of IU. Health anxiety was operationalized as global levels of health anxiety, as well as health anxiety experienced in response to Internet searches for medical information. Of note, some research has cast doubt on the relative importance of IU to health anxiety, with Boelen and Carleton 13 finding that the relation between IU and health anxiety was rendered nonsignificant after accounting for general distress. As such, general distress was controlled for in the present analyses to ensure observed effects were not attributable to overlap with this variable. Based on prior studies investigating the moderating role of IU on phenomena relevant to health anxiety, 12 it was predicted that the relation between the frequency of Internet searches for medical information and health anxiety would grow increasingly stronger as IU increased.
Finding IU to moderate the relation between Internet searches for medical information and health anxiety would allow for a better understanding of when cyberchondria might occur. Results consistent with predictions might also have important implications for the treatment of health anxiety. For example, safety behaviors are a core target of treatment for health anxiety.5,14 Finding IU to moderate the relation between the frequency of Internet searches for medical information and health anxiety might highlight the importance of directly targeting IU when seeking to reduce the engagement in safety behaviors for health anxious individuals. As noted by Deacon and Abramowitz, 15 intervention strategies that directly target IU are not routinely implemented into existing health anxiety treatments.
Materials and Methods
Participants
The sample consisted of 512 medically healthy adults. The mean age of the sample was 33.4 years (SD=12.1). Respondents primarily self-identified as female (55.3%), having received at least a 2 year college degree (59.0%), working at least 20 hours per week (52.8%), and as currently unmarried (66.7%). In terms of racial/ethnic identification, 78.7% of respondents self-identified as Caucasian, 6.5% as Asian, 6.3% as African-American, 4.1% as Hispanic, 2.3% as bi- or multiracial, 1.1% as Native American, and 1% as of “other” race/ethnicity.b
Measures
Intolerance of Uncertainty Scale-12 item Version (IUS-12) 16
The IUS-12 is a 12-item version of the original 27-item Intolerance of Uncertainty Scale (IUS) 17 and assesses IU (e.g., “I always want to know what the future has in store for me”) on a 5-point scale (ranging from 1 to 5). Although research indicates that the IUS-12 can be used as a multidimensional scale, 16 no predictions were made as to the differential performance of the separate IUS-12 scales. Thus, the total scale was used in the present research. The IUS-12 has demonstrated good psychometric properties, including total scale convergence of 0.96 with the 27-item IUS. 16 The IUS-12 demonstrated good internal consistency in the present study (Cronbach's α=0.93).
Short Health Anxiety Inventory (SHAI) 18
The SHAI is an 18-item measure that assesses health anxiety independent of actual physical health status (e.g., “I spend most of my time worrying about my health”). Responses are given on a 4-point scale (ranging from 0 to 3), with response choices varying based on the question. Following the recommendations of Alberts et al., 19 only 14 of the SHAI items that directly assess health anxiety were used in the present research. The SHAI has shown a strong convergent correlation (r=0.63) with another self-report measure of health anxiety. 20 The SHAI demonstrated good internal consistency in the present study (α=0.92).
Health anxiety as a result of Internet searches for medical information
Following prior research, 4 health anxiety as a result of searching for medical information on the Internet was assessed using a single item (i.e., “What impact does searching for health information online have on your level of anxiety about your health?”). This item was rated using a 5-point scale (ranging from 1 to 5). The response options included “greatly reduces my anxiety,” “somewhat reduces my anxiety,” “has no impact on my anxiety,” “somewhat increases my anxiety,” and “greatly increases my anxiety.”
Frequency of Internet searches for medical information
Following prior research,3,4 the frequency of Internet searches for medical information was assessed using a single item (i.e., “Approximately how frequently do you search online for health information?”). This item was rated using a 7-point scale (ranging from 0 to 6). The response options included “never,” “less than once a month,” “once a month,” “once a week,” “2–4 times per week,” “daily,” and “several times a day.”
Positive and Negative Affect Schedule (PANAS) 21
The PANAS asks respondents to indicate to what extent single word descriptors (e.g., “distressed,” “scared”) capture how they felt on a 5-point scale (ranging from 1 to 5). The negative affect (NA) scale of the PANAS—the PANAS scale of interest in the present study—consists of 10 items. This scale correlates moderately to strongly with other indices of general distress (r=0.51–0.74). 21 PANAS-NA demonstrated good internal consistency in the present study (α=0.92).
Procedure
Participants were recruited using Amazon's Mechanical Turk (MTurk), an Internet-based platform that allows individuals to request the completion of jobs (e.g., survey completion) for monetary compensation. Respondents completing surveys through MTurk have been found to produce high quality data and tend to be more demographically diverse than either standard Internet samples or American undergraduate samples. 22
The present research was approved by the local institutional review board. Recruitment was limited to MTurk workers over 18 years of age and located in the United States. All participants reported that they had not been diagnosed with a medical condition by a doctor. This methodology was used to ensure physical health minimally contributed to observed levels of health anxiety. Participants were required to provide electronic consent, and there was no penalty for withdrawing from the study. Upon completion of the study, participants were debriefed and paid in full. Compensation was $1, an amount consistent with the compensation given to MTurk workers completing prior studies of similar length. 22
Data analytic strategy
Aiken and West's 23 recommendations for testing continuous interaction effects were used in the present research. First, the Internet searching frequency item and IUS-12 were mean centered. These two mean centered predictors were entered simultaneously into Step 1, and their interactive effect (calculated as the product of the mean centered predictors) was entered into Step 2 of a regression model. The SHAI was the criterion in one regression model, and the item assessing health anxiety in response to Internet searching was the criterion in the other regression model.
Significant interactions were further examined using graphs and simple effects (following Aiken and West 23 ). Two simple regression equations were constructed (using +1 SD from the IUS-12 mean) for each model to depict the interaction effect. To plot these equations, two values of the Internet searching frequency item (+1 SD from the item mean) then were substituted into the equations. Significance of the simple slopes of these regression equations were tested at both low (−1 SD) and high (+1 SD) IUS-12 values to examine relations between Internet searching frequency and health anxiety at different levels of IU.
Results
Internet searching, IU, and health anxiety
Descriptive statistics and zero-order correlations among the study variables are presented in Table 1. The 58 participants who reported “never” searching for medical information on the Internet were excluded from analyses when examining this criterion (i.e., health anxiety as a result of searching for medical information on the Internet). As expected, all of the study variables significantly correlated (p<0.01). Regression results examining the moderating impact of IU indicated that both Frequency of Internet Searches (b=2.12, partial r=0.38) and IUS-12 (b=0.30, partial r=0.46) were significant predictors of SHAI scores in Step 1 (R2=0.39) of the regression model (p<.01). As predicted, the Frequency of Internet Searches×IUS-12 interaction (b=0.08, partial r=0.15) explained additional significant unique variance (ΔR2=0.02, p<0.01) in SHAI scores in Step 2. This interactive effect (b=0.06, partial r=0.13) continued to explain significant unique variance (ΔR2=0.01, p<0.01) in SHAI scores after accounting for general distress (PANAS-NA: b=0.27, partial r=0.34, p<0.01). Simple effects of the interaction are depicted in Figure 1. Simple effects revealed that the relationship between Frequency of Internet Searches and SHAI were significant at both high (b=2.60, partial r=0.40, p<0.01) and low (b=1.13, partial r=0.14, p<0.01) levels of the IUS-12.

Moderating effect of intolerance of uncertainty (IU=Intolerance of Uncertainty Scale-12-item version) on the relation between frequency of Internet searches for medical information and global health anxiety (SHAI=Short Health Anxiety Inventory).
Note. N=512. aN=454 (sample restricted to individuals who reported searching for medical information on the Internet). All r values significant at p<0.01 (two-tailed).
In the second regression model, both Frequency of Internet Searches (b=0.17, partial r=0.15) and IUS-12 (b=0.03, partial r=0.23) were significant predictors of Health Anxiety in Response to Internet Searches scores in Step 1 (R2=0.11) of the regression model (p<0.01). As predicted, the Frequency of Internet Searches×IUS-12 interaction (b=0.02, partial r=0.15) explained additional significant unique variance (ΔR2=0.02, p<0.01) in Health Anxiety in Response to Internet Searches scores in Step 2. This interactive effect (b=0.02, partial r=0.14) continued to explain significant unique variance (ΔR2=0.02, p<0.01) in Health Anxiety in Response to Internet Searches scores after accounting for general distress (PANAS-NA: b=0.04, partial r=0.23, p<0.01). Simple effects of the interaction are depicted in Figure 2. Simple effects revealed that the relationship between Frequency of Internet Searches and Health Anxiety in Response to Internet Searches were significant at high (b=0.27, partial r=0.21, p<0.01), but not low (b=−0.06, partial r=−.03, not significant), levels of the IUS-12.
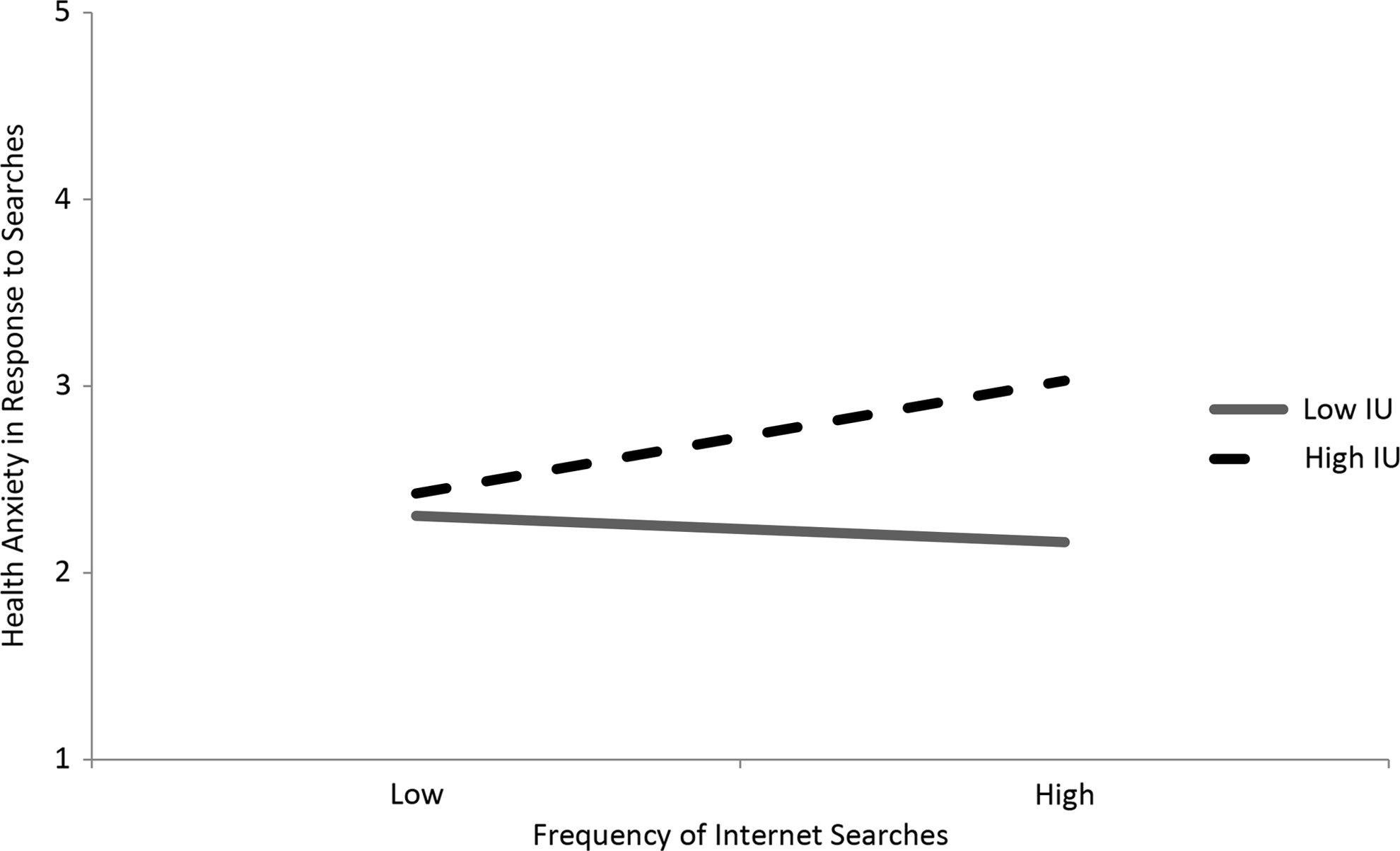
Moderating effect of intolerance of uncertainty (IU=Intolerance of Uncertainty Scale-12-item version) on the relation between frequency of Internet searches for medical information and health anxiety in response to Internet searches.
Discussion
Individuals often search for medical information on the Internet. For some individuals, though, this behavior exacerbates health anxiety, a phenomenon termed cyberchondria. 5 To date, little is known about under what conditions individuals experience cyberchondria. The present research helped fill this gap in the literature, and found that IU moderated the impact of searching for medical information on the Internet on health anxiety. Specifically, the relationship between the frequency of searching for medical information on the Internet and health anxiety grew increasingly stronger as IU increased. This moderating impact of IU was not attributable to general distress. Overall, these results suggest that individuals who have difficulty tolerating uncertainty are especially likely to experience cyberchondria.
As described, an individual who searches for medical information on the Internet will likely be presented with multiple explanations for symptoms, some of which might be catastrophic explanations. 2 The present results indicate that individuals with high IU are especially likely to experience health anxiety in response to such Internet searches (i.e., cyberchondria). One tenable reason for this finding is that individuals with high IU experience heightened levels of anxiety when faced with multiple possibilities. 8 The anxiety-provoking nature of being presented with multiple explanations of medical concerns for individuals with high IU might relate to the perceived probability and cost estimates of potentially suffering from a serious medical problem. For example, IU is associated with the tendency to form catastrophic health appraisals in response to ambiguous health information. 12 IU has also been found to be associated with heightened cost estimates surrounding negative outcomes. 24 Although this explanation remains to be empirically tested, when presented with multiple explanations for symptoms, individuals with IU might be especially likely to catastrophize about the possibility of having a serious health concern and perceive such a possibility as especially costly. Such catastrophizing might lead to repeated attempts to gain certainty about one's medical status (e.g., use of safety behaviors). These attempts to gain certainty in turn likely exacerbate health anxiety.
As noted, although safety behaviors are a central target within interventions for health anxiety,5,14 IU is not routinely targeted within health anxiety interventions. 15 However, researchers have described some intervention strategies potentially useful for reducing IU. For example, Abramowitz and Braddock 14 described cognitive strategies for increasing tolerance for uncertainty, in which clients learn to accept that a definitive explanation for ambiguous body sensations and symptoms is not possible. Moreover, Tolin et al. 8 described the possible use of behavioral strategies to reduce IU (e.g., exposing individuals to uncertain situations without the use of safety behaviors). Through such exercises, an individual can habituate to the anxiety surrounding feelings of uncertainty and better tolerate uncertain situations.
The above findings and considerations should be considered with the following limitations in mind. First, the use of self-report measures as the sole method of assessment might have inflated observed relations among the study variables. However, correlated measurement error—which might be expected with monomethod assessment—does not appear to produce spurious interactions; rather, it may attenuate them. 25 The assessment limitation is therefore not likely responsible for the observed significant interaction. Second, the cross-sectional and correlational nature of these data precludes causal conclusions. In particular, these data are unable to speak as to whether the interactive effect between frequency of searching for medical information on the Internet and IU causally impacts levels of cyberchondria. It will be important for future research to extend these results using experimental and longitudinal designs to understand causes of cyberchondria better. Third, following prior research,3,4 single item indicators were used to assess for the frequency of Internet searches for medical information and health anxiety experienced in response to these searches. Although single item indicators are appropriate when the construct is sufficiently narrow, 26 it will be important for future research to develop measures that more comprehensively assess these two constructs. Fourth, the observed interaction explained only modest variance in health anxiety. Statistical constraints on the magnitude of effect sizes of interactions from nonexperimental designs are well documented. 27 Moreover, the variance accounted for by the interaction reflects meaningful information (>1%) 25 and the magnitude of the observed interactive effect of IU on health anxiety in the present research was consistent with the size of the moderating impact of IU found in prior studies. 12 Finally, although use of a sample unselected based upon levels of health anxiety is consistent with the dimensional (i.e., nontaxonic) nature of health anxiety,28,29 generalization of these results would be supported via replication in samples with a larger number of individuals scoring on the higher end of the distribution of health anxiety scores.
Limitations notwithstanding, the present results indicate that IU is important for better understanding the relation between safety behaviors and health anxiety. Specifically, searching for medical information on the Internet appears especially likely to lead to health anxiety (i.e., cyberchondria) for individuals with high IU. These results indicate that IU is important for better understanding health anxiety and cyberchondria—a conclusion that might ultimately lead to increased attention to IU within health anxiety interventions.
Notes
a. Some researchers consider uncertainty to be an essential component of anxiety, 9 which could raise concerns as to the overlap between IU and anxiety symptoms. However, extant data suggest that IU and anxiety symptoms (e.g., worry) are distinct. 30 Although no known published study has examined the distinctiveness of IU from health anxiety per se, measures of these two constructs appear to assess largely unique content. For example, the Short Health Anxiety Inventory (SHAI) 18 predominantly assesses for worry about health. 31 Moreover, existing theoretical models treat IU and health anxiety as distinct constructs, 6 and the magnitude of correlations between measures of these two constructs does not suggest redundancy. 13 For these reasons, IU and health anxiety were considered meaningfully distinct enough to warrant the present investigation.
b. The moderating effect of IU was still evidenced when accounting for age and gender.
Footnotes
Author Disclosure Statement
No competing financial interests exist.