
Abstract
Abstract
Burnout is a globally increasing illness, and as a result, many forms of burnout therapy have arisen. The use of digital games can be psychotherapeutically effective because they can transform exercises that are by themselves unattractive into intrinsically motivated action. This pilot study aims to test whether a specially designed game contributes to patients learning desired behavior and achieving other specific therapeutic goals in an online cognitive–behavioral therapy (CBT)-based burnout treatment context. In total, 101 participants took part in the experiment, under four conditions: (a) Game+Therapy, (b) Therapy Only, (c) Game Only, and (d) No Game+No Therapy. Pre- and postmeasures were taken online. Results showed that the two therapy conditions (Game+Therapy and Therapy Only) showed a greater decrease in complaints and disengagement, and a stronger increase in coping skills than the nontherapy conditions (Game Only and No Game+No Therapy). As expected, the Game+Therapy condition outperformed the Therapy Only condition on combined improvement measures of burnout symptoms. However, analyses of individual measures showed no effects. It can be cautiously concluded that the therapeutic digital game may be a useful tool when embedded in a therapeutic burnout treatment program and is probably more efficient than CBT, as it is used in current practice.
Introduction
B
Burnout has been defined as “the occurrence of emotional exhaustion, unusual fatigue, a cynical or detached working attitude and a feeling of decreasing competence.” 6 (p14) The Maslach Burnout Inventory (MBI) is the most commonly used self-report index, measuring three factors: emotional exhaustion, depersonalization, and decreasing personal accomplishment.7,8 In another recently proposed index, the latter factor was omitted. 9 Burnout has a three-stage etiology: (a) imbalance of job demands and energy resources, (b) precursive symptoms, and (c) burnout syndrome. 10 Precursive symptoms include stress,11–15 depression,11,12,15–17 and anxiety12,15,16,18–20 They tend to persist after the second stage.
Among the treatments for burnout syndrome, 21 relaxation, stress management, and cognitive–behavioral therapy (CBT) have proven effective and are broadly used. 11 CBT was found to be effective for the specific burnout-related problems of stress, 22 unexplained fatigue, 23 depression, 24 and anxiety disorder. 25 CBT hinges on the insight that psychological complaints are based on automatized behavior and cognition that can be altered through learning. 26 CBT aims to cure patients by training them to cope with stress. Favorable cognitive and behavioral habits are learnt, such as recognizing negative thoughts and setting personal boundaries.11,22
Burnout therapy is increasingly administered online. Online platforms include e-mail, e-chat, Web sites, video conferencing, and mobile applications, either as (guided) self-help therapy or as actual psychotherapy. 27 The Amsterdam-based firm Interapy was the first certified agency worldwide to offer a complete online burnout CBT program. Use is made of e-mail and a Web site for correspondence between the patient and the therapist. Figure 1 describes how the program functions. The Interapy program is an effective and easily accessible program. 12 This study investigates whether the program could be further improved through the use of serious games.
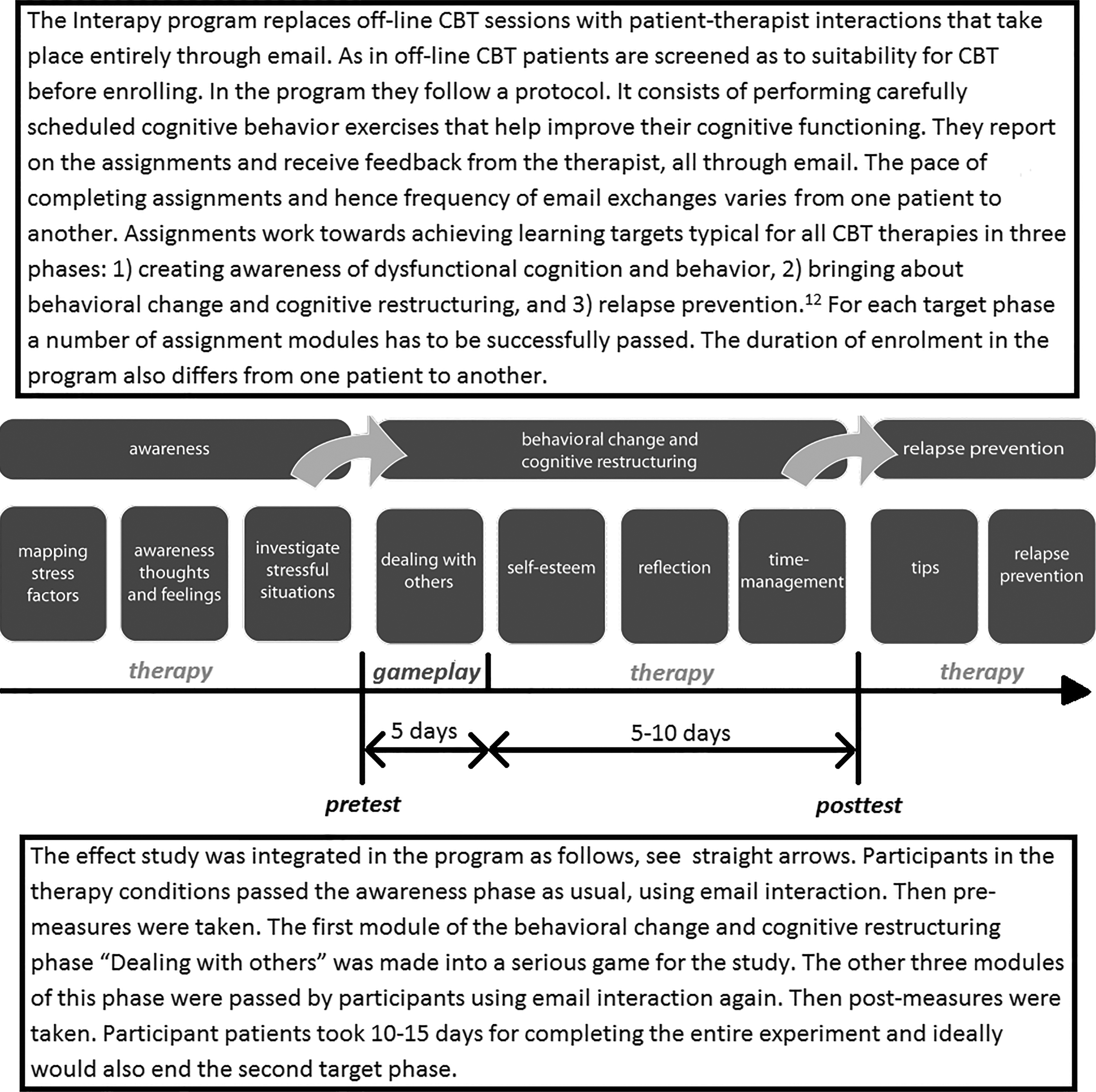
The Interapy burnout program, 12 including protocol for participants in the Game+Therapy condition.
Some positive outcomes of serious gaming have been found in a number of fields.28–31 Serious games are not primarily designed for entertainment, but for purposes such as education, training, therapy, or behavioral change. 32 Research on the effects of psychotherapeutic games is quite recent. Yet, support has been reported of beneficial effects in the treatment of a variety of complaints, including depression, divorce trauma, autism, and phobias.33–45 This article reports a pilot study testing the incremental value in terms of user motivation and treatment effectiveness of “gamifying” an existing online CBT-based burnout module.
The psychotherapeutic effectiveness of games originates in their capability of transforming exercises that are in themselves unattractive into intrinsically motivated action. Playing games is consciously experienced as enjoyable, while, at the same time, players are also honing their skills and capacities, even though they are unaware of doing so.46,47 The game experience elements responsible for users' engagement in what is an exercise include challenge48,49 and flow. 50 Appropriate game challenges are neither too difficult nor too easy to meet. Optimal challenges make for an exceptionally pleasurable state of immersion in activity referred to as flow.50–53 This experiential state requires a perfect balance between game challenges and user skills.53,54 Appropriate games link flow to two ends. First, optimal challenge and flow boost players' self-esteem because not-too-easy successes are experienced and ascribed to the self. Second, their (cognitive) behavioral repertoire is expanded with new responses, which in turn boosts self-esteem, 52 as demonstrated in players of therapeutic games.54–56
Gamification and the Persuasive Game Design model
This study aims to test whether a game specially designed to present users with carefully planned challenges and flow experiences contributes to patients learning desired behavior in an online CBT-based burnout treatment context. The design philosophy is gamification based on existing psychotherapy, enriching the proven practice of burnout CBT with games as an added tool for the therapist. The Persuasive Game Design model (Fig. 2) provides the framework for the game's design. Motivating game elements, such as challenges, first transport the player into a game world where equivalents of real world tasks are carried out. Persuasive games can be so structured as to achieve transfer of effects from the experienced game world to the real world. 48 In the present case, transfer effects would result in real world skills reducing burnout symptoms.
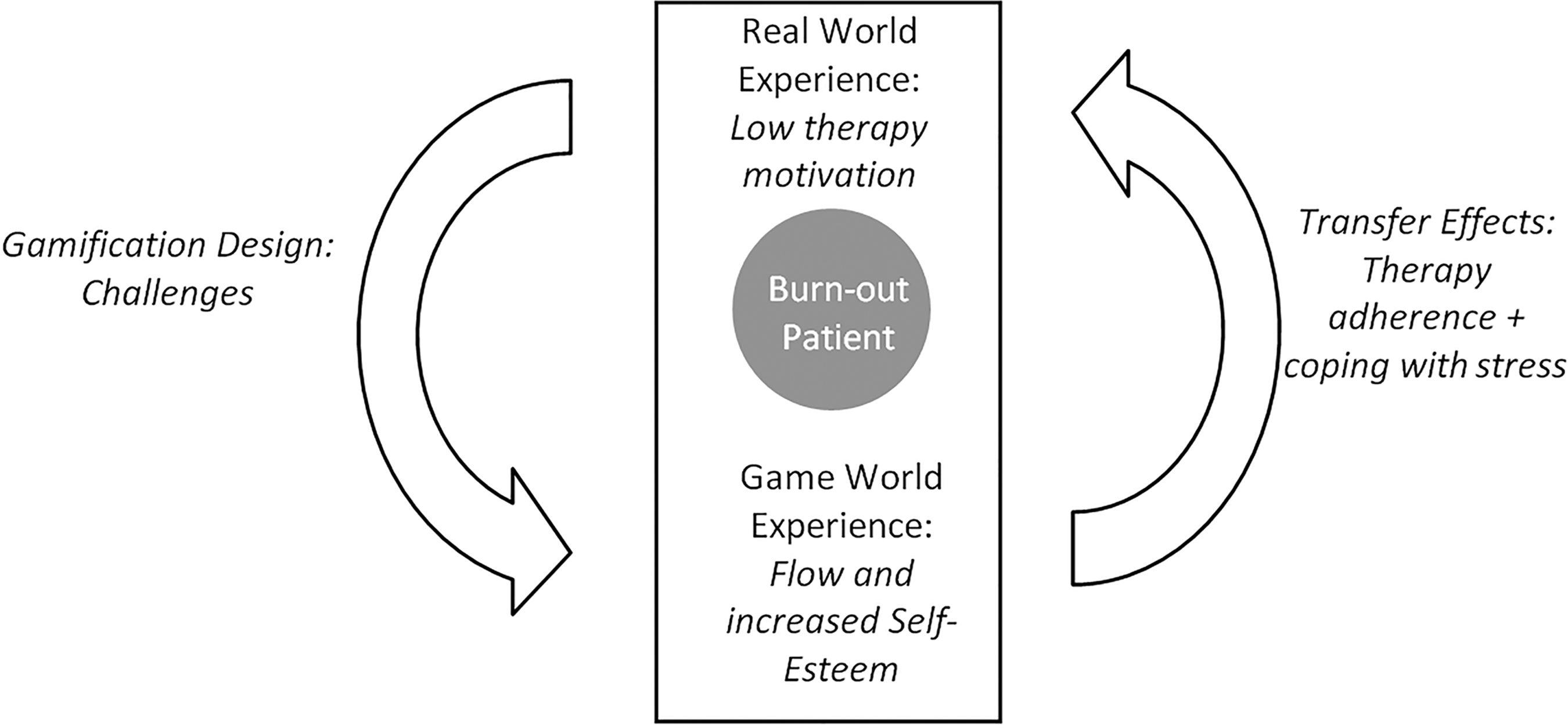
Application of the Persuasive Game Design model on burnout therapy. 59
Research expectations and hypotheses
The reported experiment had a two factor design: therapy versus no therapy and gaming versus nongaming. As the game was designed to enrich current therapy, it was anticipated that therapy plus game would outperform therapy without it. However, as a successful therapy was gamified, it was expected that the game without therapy would be less effective than therapy without the game. In contrast, using the game without therapy was expected to have significant but less than optimal effects. Finally, there was a control condition where patients received no treatment at all.
The tested hypothesis, then, is that the treatment's effectiveness would increase over the experimental conditions in the following order: (a) no therapy or game (control), (b) game without therapy, (c) therapy without game, and (d) therapy including game.
Method
Participants
The study was embedded in the online Interapy burnout treatment program (Fig. 1). The experiment enrolled 101 people, 85 of whom completed the entire procedure. All patients had symptoms of burnout, and 76% of the patients were medically diagnosed as being burnout patients. The ages of participants ranged between 24 and 63 years old, with an average of 40 years (SD=9.09); 78% had achieved higher education, and 51% were male.
Design and procedures
The study is a quasi-experiment, with a 2×2 pretest–posttest mixed design and conditions Game Only (GO, n=27), Game+Therapy (GT, n=17), Therapy Only (TO, n=20), and No Game+No Therapy (NGNT, n=21). Experimental manipulations came into effect right after the awareness phase (Fig. 1). In TO and GT conditions, premeasures were taken before the awareness phase; in the remaining conditions, this was done upon participants' enrolment in the study. Postmeasures were taken 10–15 days after the premeasure when TO and GT participants were at the end of the behavioral change and cognitive restructuring phase. These participants received enjoyment questionnaires upon completing the game.
Participants in the GT condition were recruited from another cohort than those in the TO condition. Due to a lack of patients, it was not possible to run four groups at once. For this reason, data were initially collected for GT, TO, and NGNT conditions. Due to changes in the program management, the TO condition could only be run 18 months later, effectively rendering the study into a quasi-experiment. Participants to GT and TO conditions were Interapy burnout patients, who were invited by their therapist. Participants to GO and NGNT conditions were recruited from two online burnout forums and randomly assigned. Ethical procedures of the certified therapy institute were strictly followed. All participants signed a consent form before taking part. Participants could win a book in return for their participation. The researcher was aware of the assigned condition of each patient, whereas patients and therapists were not.
Experimental material: the game
Assignments that were part of the original therapy module formed the basis of the levels of the game. In the gamification process, six general game elements were applied to increase the players' engagement and enjoyment of the game world (see Table 1).
The module Dealing with Others aims to train patients in dealing assertively with job colleagues and entertaining positive thoughts about themselves or their social environment. Abstract stylization of the game world reduced the challenge set by the first level. Later levels increased the challenge by requiring new behaviors in more settings, consolidation of positive thoughts, and a positive mind-set. Positive feedback from the game reinforced positive thinking, also lowering anxiety and depression and contributing to self-esteem, ultimately improving the player's capability to deal with others in the real world. Figure 3 shows a description of the therapeutic game. Patients played the game online, and there was no supervision from the therapists.
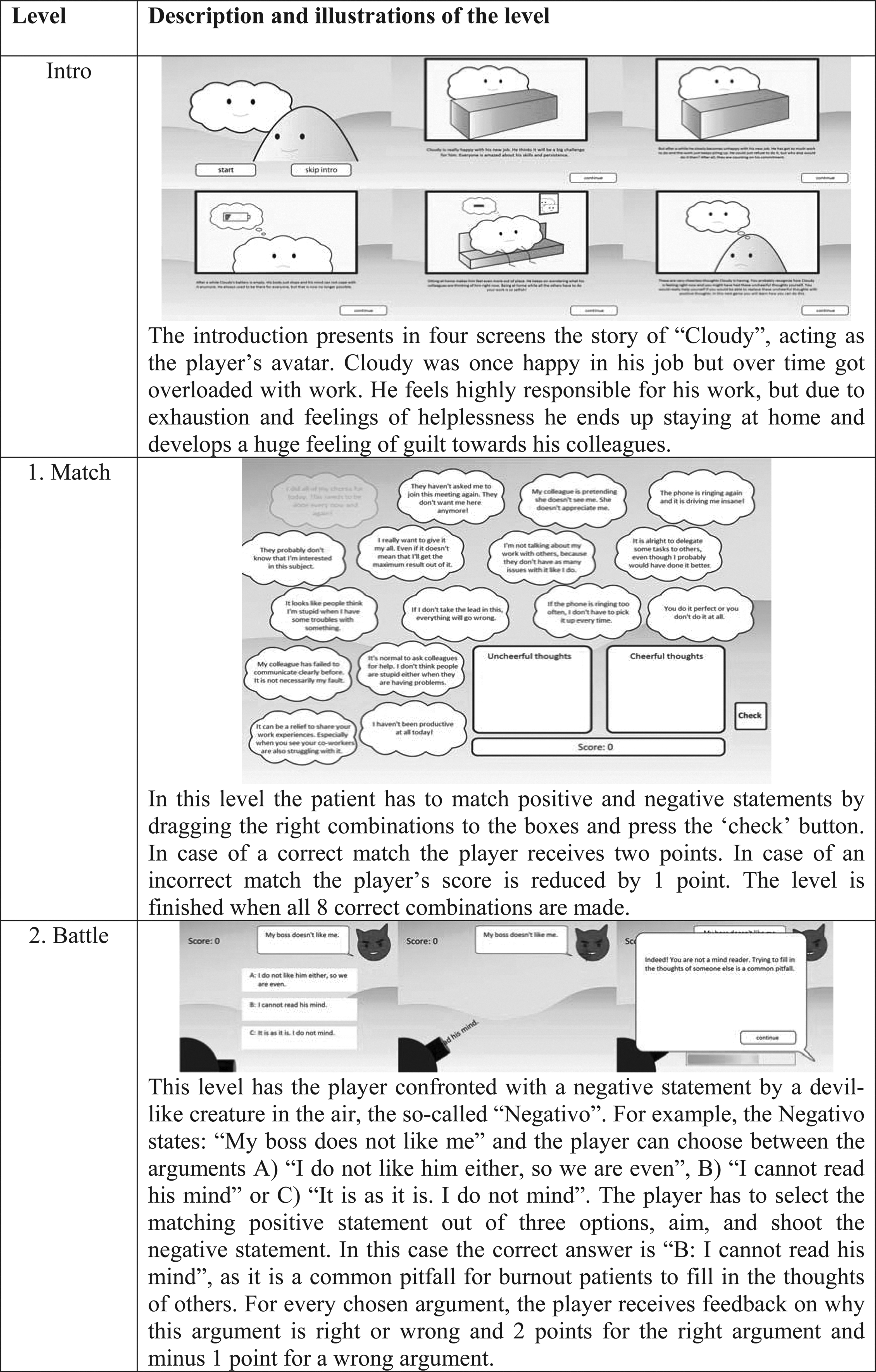
Description of the game.
Dependent variables
Pre- and postmeasures included the following variables: (a) (precursive) burnout symptoms, (b) self-esteem, (c) coping skills, and (in the GO and GT conditions) (d) game enjoyment. Burnout symptoms are defined as symptoms affecting body, mood, and thoughts and consist of depression, anxiety, stress, and disengagement. The first three complaints were measured by items from the Depression Anxiety Stress Scale that uses 21 variables with a 7-point rating scale. 57 It should be noted that depression, anxiety, and stress are considered by therapists as precursive symptoms—early symptoms exhibited by burnout patients in the process of developing the syndrome. Disengagement is defined as distancing oneself from one's work and experiencing negative attitudes toward it. 10 It was measured by eight items on a 7-point Likert scale from the Oldenburg Burnout Inventory.10,58
Self-esteem is defined as a feeling of confidence in one's competence. It was measured by a 7-point Likert item from the Single Item Self Esteem (SISE) scale. 59 Coping skills involve setting of personal boundaries, positive self-image thinking, and restraining perfectionism. These three variables are standard measures of progress in Interapy's burnout program and are derived from validated instruments such as the Depression Anxiety Stress Scale and the Maslach Burnout Inventory. 12 Each were measured by five option multiple choice questions that were used as a test variable to see if the patient learned the desired behavior.
The experience of enjoyment while playing the game was measured only in the TG and GO conditions, using 7-point rating scales: likeable, funny, interesting, exciting, challenging, and useful. Flow was measured by three 7-point scales for challenge, immersion, and autonomy from the EGameFlow scale. 60
Control variables were gender, age, education, Internet usage, game usage, game attitude, and game completion.
Results
Treatment effects
Table 2 lists the results of pre- and posttest of precursive symptoms and of disengagement.
GT, Game+Therapy; TO, Therapy Only; GO, Game Only; NGNT, No Game+No Therapy.
Precursive symptoms of burnout—depression, anxiety, and stress—were combined into one measure (α=0.76). A multivariate analysis of covariance (ANCOVA) of combined complaints and disengagement, with treatment conditions as the between-subjects factor and pre–posttest as the within-subjects factor, was performed with gender, age, and education as covariates. Main effects of pre–posttest, F(1, 78)=5.17, p<0.05, and treatment conditions, F(3, 82)=6.15, p=0.001, were found to indicate that levels of precursive symptoms and disengagement across pre- and posttest differed from one condition to another. An interaction effect between the pretest and the posttest and treatment conditions was detected, F(3, 82)=7.29, p<0.001, η2p=0.210, observed power=0.980.
Precursive symptoms
A main effect of pre–posttest was seen, F(1, 82)=9.97, p<0.005),a as well as a main effect in the treatment condition, F(3, 82)=2.86, p<0.05, indicating that the levels of precursive symptoms across pre- and posttest differed from one condition to another. Post hoc tests showed a significant difference between therapy and nontherapy conditions. However, it was found that the difference between playing the game and not playing the game was not significant. The effect for pre–posttest disappeared when controlling for age, gender, and education, Fpre–posttest(3, 78)=2.55, p=n.s.
An interaction effect between pre–posttest and treatment conditions was found, F(3, 78)=8.59, p<0.001, η2p=0.248. Precursive symptoms exhibited a decreasing trend for the GT, TO, and GO conditions, while the NGNT condition exhibited an increasing trend (Fig. 4). A repeated measures analysis of variance with only GT and TO conditions showed a significant interaction between pre–posttest and condition factors, F(1, 43)=7.15, p<0.05, η2p=0.152; the steeper decrease of complaints in the GT compared to the TO condition was reliable.
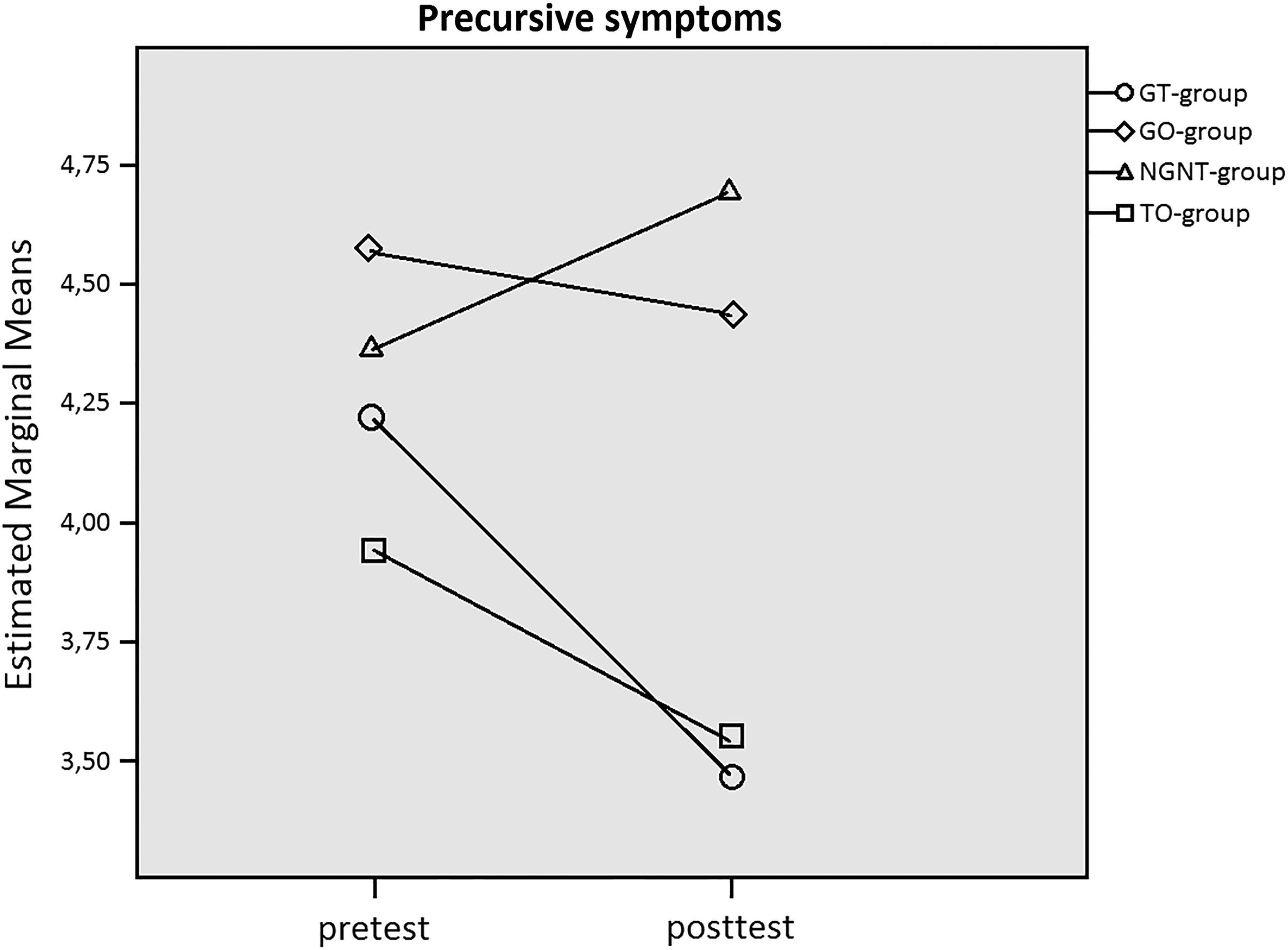
Plots for interaction between pre–posttest and treatment condition. Estimated marginal means for precursive symptoms.
Disengagement
Disengagement scores differed between the pretest and the posttest, and point out a main effect for pre–posttest, Fpre–posttest(3, 78)=7.17, p<0.001). However, no main effect was found for treatment condition, meaning that treatment conditions did not differ as to disengagement level, Fcondition (1, 78)=0.314, p=n.s. Post hoc tests again showed significant differences between the therapy and nontherapy conditions, but not between game and no game ones. No interaction was obtained between pre–posttest and treatment condition (p=0.18).
Separate multivariate analyses of variance for depression, anxiety, stress, and disengagement showed differences between treatment conditions and between pre- and posttest, but no interaction effect of the two factors.
Coping skill improvement and self-esteem
A main effect of pre–posttest for coping skill improvement, F(1, 81)=31.60, p<0.001, was found. Here, the treatment condition also had a main effect, F(3, 81)=3.96, p<0.05, while an interaction effect between pre–posttest and treatment conditions was present as well, F(3, 81)=4.96, p<0.005, η2p=0.155. Post hoc tests for complaints and disengagement pointed out similar results. However, this time there was no difference between the TO condition and the GO condition. Finally, self-esteem was found to be stable from pre- to posttest and invariant across treatment conditions.
The role of enjoyment and flow
Descriptive statistics for the experience of the game as a whole and for separate levels can be found in Table 3. A between subjects ANCOVA showed no differences in enjoyment of the game between GO and GT conditions, F(1,43)=1.99, p=n.s.
In order to check the assumption that flow causes enjoyment, a regression analysis was performed on joint data of GT and GO conditions with flow, game behavior, game attitude, gender, age, and education as predictors.b Flow predicted enjoyment (β=0.868, p<0.001), as did age (β=–0.188, p<0.01). The effects of game enjoyment on improvement were explored (Table 4). A combined measure for game enjoyment did not predict any of the three reductions in complaints. However, enjoyment did predict improvement of coping skills, while skill improvement in turn predicted decrease of stress and depression symptoms.
Bold indicates significant results.
Discussion
Findings
This pilot study aimed to test whether a therapeutic digital game is an efficient and suitable tool to aid patients in achieving therapeutic goals in an online CBT-based burnout treatment environment. As predicted, the two therapy conditions (GT and TO) showed a higher decrease of precursive complaints and disengagement as well as a stronger increase of coping skills than the nontherapy conditions (GO and NGNT). As also expected, the GT condition outperformed the TO condition on improvement measures of precursive symptoms (taken as a combination of disengagement, depression, anxiety, and stress). However, analyses of separate measures did not reveal differential decreases across treatment conditions. Finally, skill improvement was more pronounced in the two therapy conditions, but no more so in the GT than the TO condition.
Differences in progress between therapeutic and nontherapeutic conditions can be interpreted to mean that participating in a CBT-based burnout program results in a reduction of the (precursive) burnout symptoms—depression, anxiety, stress, and disengagement—superior to not participating in such a program. In addition, it can be concluded that the therapeutic digital game may be an effective tool when embedded in a therapeutic burnout treatment program and is more effective than CBT alone as it is used in the current practice of Interapy. Caution is needed, however, because significantly better progress was found on the combined measures only. More importantly, the game as a standalone burnout treatment is not as successful as participating in a burnout treatment program. This lends support to a gamification approach that takes existing therapeutic practice as its starting point. That approach also contributed to the ecological validity of the results because measures could be used that have served as treatment outcomes for more than a decade.c Major insights acquired in the therapeutic contribution of game play include (a) that experiencing the flow of playing the game boosted enjoyment and hence learning motivation, and (b) that enjoying the game indirectly targets burnout by facilitating acquisition of skills for coping with its symptoms.
Related work and future research
In the last decade, research on computerized CBT (cCBT) has been plentiful. Most studies imply that digitizing CBT in one way or another has great potential.61–64 Also, as mentioned earlier, many games and “playful interventions” have been developed for therapeutic purposes.33–45 However, the use of games as a tool for cCBT is quite uncommon. In fact, only one study of a game fully integrated into a CBT surrounding was found. 65 This study found high usability and acceptance among therapists and patients of a game under development, while the present study tested treatment outcomes of a novel game integrated into actual therapy. More research should go toward the exploration of “gamified CBT” (gCBT), a term introduced now on the fly.
In further research, additional therapy modules may be gamified, possibly enhancing the present game's potential. The design is on the right track; witness the finding that enjoyment is positively associated with practicing skills. Another improvement might be to grant the therapist a role in the currently unsupervised game, in order to reinforce desirable behavior in combination with the game's feedback.
Limitations
A major setback to this study as a one module treatment manipulation is that it can only capture changes in a limited number of outcome variables, leaving out, for example, emotional exhaustion symptoms and growth of self-esteem, which could not be established in any of the therapy conditions. This requires a longitudinal design across subsequent CBT modules.
Other shortcomings include:
• As is common in clinical treatment effect studies, assignment to conditions could not be completely random. Differences between conditions prior to treatment prevented direct comparison of postmeasures. The number of patients willing to participate was low. The number of patients in the GT condition (n=17) in particular may have reduced power to detect differences in comparison to the TO condition. • The TO condition was carried out almost 18 months after the other conditions. This may have resulted in historical bias. • Of all the patients, 76% were medically diagnosed as burnout patients. This statistic could only be established at the point of pretest, after the conditions were already assigned. In spite of burnout patients being randomly assigned, they were not equally divided across the conditions. • The two therapy conditions may have developed treatment sensitization66,67 with unknown consequences.
The results of this study cannot be generalized to all burnout types and severities, and current game levels and situations may not fit with different treatment modules. Tailoring the game toward the specifics of other stressors than used here is a direction for future research to explore.
Conclusion
This study showed that people who experience the burnout symptoms of depression, anxiety, stress, and disengagement can be treated at least as effectively—and probably more effectively—when the therapist deploys a specially designed digital game compared with conventional therapy in a CBT-based burnout treatment program. It was found that experiencing flow and enjoyment, due to playing a properly designed therapeutic game, may ultimately benefit recovery from burnout symptoms and complaints. Thus, the research underlines the promise of gamifying mental health practices for improved patient experience.
Notes
a. For all repeated measures analyses of variance, a GLM procedure (MANOVA) was used in SPSS.
b. The adjusted R2 for this model was 0.789.
c. In addition to this, solid Cotan (Dutch commission of test affairs) scores were administered to the test scales that form the basis of the treatment.
Footnotes
Author Disclosure Statement
Sam van Tienhoven, Helle Sinkbaek, and Bart A.L. Schrieken are employees of Interapy and receive a regular salary from Interapy according to their labor contract. Alfred Lange is the founder of Interapy. When Interapy was sold to five mental health organizations in 2011, the financial relationship between Alfred Lange and Interapy ended. No other competing financial interests exist.