
Abstract
Abstract
This study aimed to apply virtual body swapping through mental rehearsal for patients with complex regional pain syndrome (CRPS) and to investigate whether it is applicable to them. Ten patients who met the diagnostic criterion for CRPS type 1 were randomly assigned to either the treatment or control group. All participants were asked to watch the virtual body swapping training video clip with a head mounted display. The treatment group was additionally asked to assume a posture similar to the body on the screen and rehearse the movements mentally, as if the body presented on the screen was their body. No difference between the groups was found for pain intensity, however, the treatment group showed significantly more improvement in body perception disturbance (BPD) after the treatment than the control group. Even if the presented study is a preliminary one, the above results suggest that virtual body swapping through mental rehearsal is applicable for patients with CRPS and may be useful for improving BPD. The limitations of the study and the future investigations needed to provide clearer clinical suggestions are presented and discussed.
Introduction
C
Mirror therapy is a representative treatment that reflects the principle of neural rehabilitation. Mirror therapy, which was originally used for phantom limb pain patients, has been introduced to manage pain and body perception disturbance (BPD) for patients with CRPS.12,13 In mirror therapy, imaginary movement of the affected limb, which is actually a reflection of the patient's intact limb in a mirror, alleviates the patient's pain by correcting conflicts between visual feedback and proprioceptive representations of the affected limb. 14 Concurrent with previous studies, some researchers who have applied mirror therapy to patients with CRPS have found that mirror therapy is effective for relieving pain and restoring disturbed body perception.15–17 However, mirror therapy appears to have limitations in that to be adopted for patients with CRPS, at least one limb should be intact. Patients with CRPS, however, may have an affected body part without a counterpart, such as the head, neck, or other body part, or the patient may have both limbs affected.
Therefore, inducing an illusionary body perception for the body instead of a single counterpart may overcome the limitations of mirror therapy. Body swapping is a way of evoking the perceptual illusion that a virtual body is perceived as his/her own body.18,19 The illusion of body swapping can be induced as body ownership is shifted from the actual body to a virtual body by watching the virtual body moving or being touched while synchronous movement or tactile stimulation is performed.20–22 Despite its potential implications, body swapping in the clinical setting, to our knowledge, has not been studied yet because even light tactile stimulation or movement can induce pain for patients with CRPS. For a treatment program for patients with CRPS to be applicable, it should (a) be available for the whole body part and limbs that are counterpart and (b) induce a low level of pain so as not to make the treatment session by itself aversive.
Our previous study opened the possibility of applying the virtual body swapping for patients with CRPS by employing mental rehearsal. Mentally rehearsing body movement without moving the actual body while watching virtual body moves in healthy participants has been found to evoke the illusion of virtual body swapping as much as physical rehearsal did. 23 This finding can be explained by the psycho-neuromuscular theory, which postulates that mental rehearsal activates a network of neural pathways required for movements so that imagining movements means actually strengthening neural pathways of physical skill.24,25 Given this, two clinical psychologists specializing in pain confirmed that virtual body swapping through mental rehearsal would be an appropriate way to evoke a body swapping illusion for patients with CRPS as it does not require any touches or gross muscular movements inducing pain.
This study aimed to apply virtual body swapping to patients with CRPS and to investigate whether it is applicable to them. As the first study to apply virtual body swapping to patients with CRPS, it is necessary to ascertain that the virtual body swapping is applicable in a small sample of patients with various pain sites. Given the findings of prior studies, we applied virtual body swapping to patients with CRPS and expected that the virtual body swapping illusion through mental rehearsal would reduce pain intensity and BPD in patients with CRPS (Hypothesis; H1).
Methods
Participants
Ten patients with CRPS type 1 were recruited from a tertiary university pain center in Seoul, Korea. The inclusion criteria for the present study fulfilled the diagnostic criteria for CRPS type 1 according to the International Association for the Study of Pain and pain doctors confirmed that the participants meet the criteria. Accordingly, the criteria included the presence of a noxious event unaccompanied by nerve lesion; continued pain, allodynia, or hyperalgesia; the region of pain suffers from edema, changes in skin blood flow, or pseudo motor activity; and the exclusion of other diagnoses.26(p330) Pain sites of each patients were various for the purpose of this study (entire body=4, more than two limbs=4, lower limb=1, upper limb=1). Patients were randomly assigned to either the treatment or control group. All participants were male and had at least high school education. The mean age of the sample was 39.30 years (SD=10.99) and the median duration of pain was 52 months (range 33–120 months). The two groups were not significantly different in age [t(8)=−1.59, p=0.15] or duration of pain [t(8)=−0.98, p=0.55].
Measurements
Pain intensity was measured on an 11-point Likert scale ranging from 0 (no pain) to 10 (severe pain). The higher the score, the more intense the pain experienced by the patient at that moment.
The modified Body Perception Disturbance Questionnaire (BPDQ) 27 was used, which consists of nine items, such as sense of disownership, lack of attention to the limb, distorted mental visualization, impaired limb position sense, dislike, and different perception of size, shape, weight, pressure, or temperature of the impaired limb. Each item was rated on an 11-point scale ranging from 0 (not at all) to 10 (very likely). A sum total score was used in the analysis (from 0 to 90), with a higher score indicating greater BPD. Cronbach's alpha for the modified BPDQ in the present study was 0.73.
A single item of the virtual body swapping illusion asks to what extent participants perceived the virtual body's movement as being their own body's movement was created for this study and measured on a 7-point Likert scale ranging from 1 (not at all) to 7 (very much). The higher the score was, the more successful the virtual body swapping experienced.
Material and training program
The virtual body swapping training video for patients with CRPS was developed and has been found to successfully evoke virtual body swapping illusion in healthy participants. 25 The 3 minute and 20 second long video clip was filmed from the first person perspective and consisted of four physical movements. The first person perspective would help patients to feel as if they observed their body when they watch video, and four physical movements were ergonomically natural from the view (making fists and opening up the fingers, bending and unbending the elbows, bending the ankles forward and backward, and bending and unbending the legs). The video was presented using a head mounted display (HMD, VR2000; Virtual Realities, Ltd.; Fig. 1) in a dim light to help patients with CRPS be immersed in the training session by blocking other sensory information. Total training sessions was designed not to exceed 10 minutes as it has been known that training longer than 10 minutes may cause fatigue and difficulty in concentration. 27 The training program was delivered by one specialist in pain and two assistants (trained graduate students).

Experimental procedure. The video was presented twice with one minute of short break.
Procedure
Participants were asked to complete informed consent form and demographic information questionnaires. Participants also responded to a pain intensity question and completed the modified BPDQ to be used as baseline data. Subsequently, all participants were asked to lie down on the sofa and watch the experimental video clip with HMD. Participants in the treatment group were additionally asked to assume a posture similar to that of the body on the screen and rehearse the movements mentally, as if the body presented on the display was their own body. In contrast, participants in the control group were not asked to perform these last two tasks while watching the video clip, to rule out an alternative explanation of the experimental results (i.e., watching the video clip itself may influence pain intensity and BPD). The experimental video clip was played twice with a 1-minute break given between viewings. The participants were then asked to respond to the pain intensity question and the virtual body swapping question and to complete the BPDQ. As a final step, all participants were debriefed on the experiment and compensated for their participation. The procedure is described in Figure 1.
Statistical analysis
One-way analysis of covariance (ANCOVA) using pretreatment condition (pain intensity and BPD) as covariates was conducted to analyze differences between the groups in post-treatment pain intensity and BPD scores. Pretreatment pain intensity and BPD were controlled in each analysis to reduce the variance of the baseline, respectively. The bootstrapping method was used to increase the robustness of small-sample analyses. 28 In the present set of analyses, parameter estimates were based on 1,000 bootstrap samples with 95% confidence intervals. An independent t test was used to investigate the difference in virtual body swapping scores between the two groups. SPSS 17.0 for windows was used for these analyses.
Results
Pain intensity and BPD
One-way ANCOVA for post-treatment pain intensity and BPD, using pretreatment pain intensity and BPD as covariates was conducted. Bootstrapped descriptive statistics are described in Table 1. There was no significant difference between the groups in pain intensity, F(1, 7)=0.05, p=0.81. For BPD, the result showed a significant difference between the groups, F(1, 8)=16.22, p=0.01, ηp2=0.70. These results indicate that the treatment group reported less BPD after treatment than did the control group (Fig. 2).
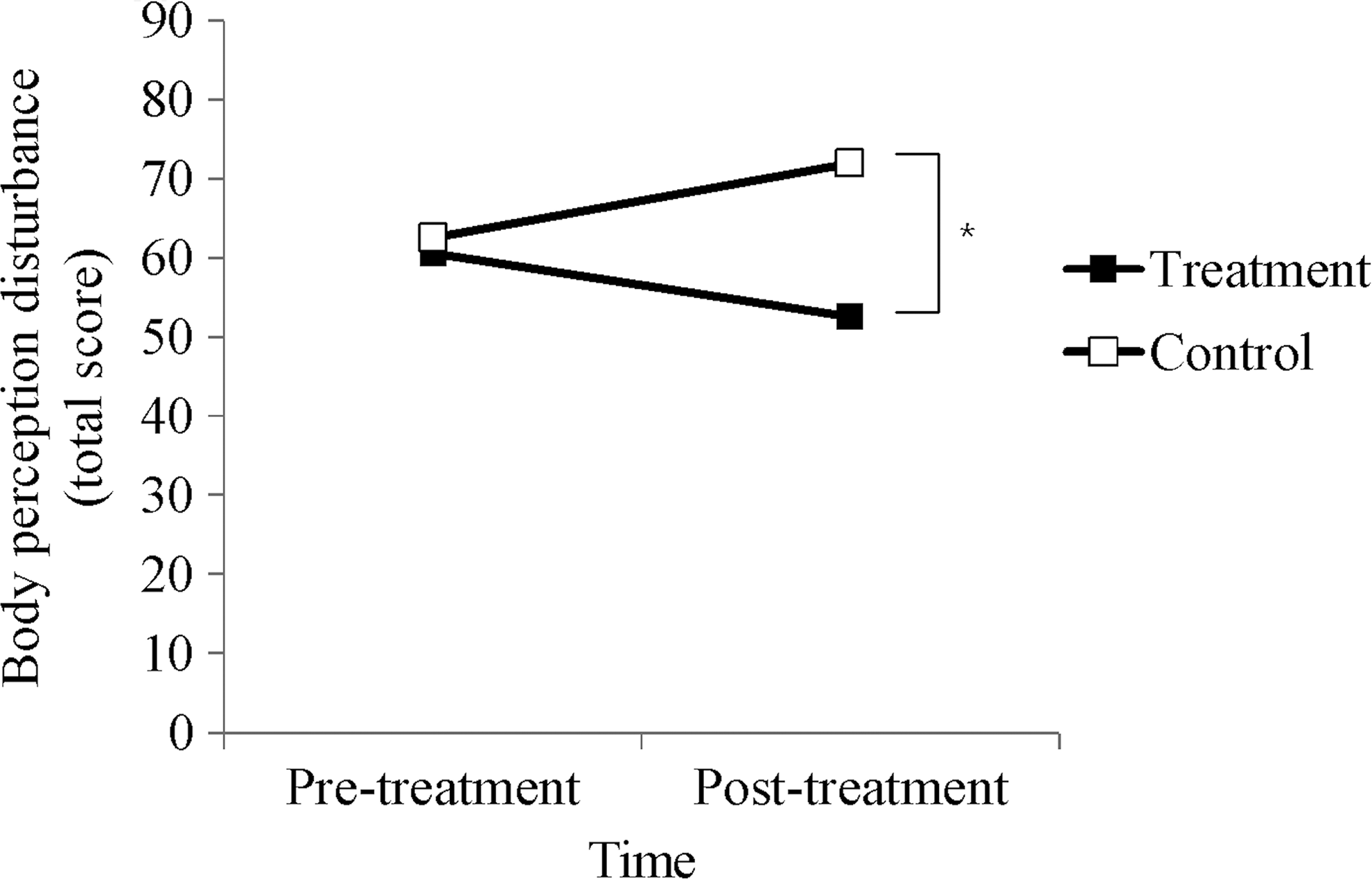
Body perception disturbance scores for treatment and control groups with time *p<0.05.
Virtual body swapping illusion
An independent t test was conducted to compare virtual body swapping illusion between the treatment and control group. A significant difference in virtual body swapping scores between the treatment and control group was found, t(8)=2.40, p=0.04, indicating that the treatment group experienced greater virtual body swapping illusion than did the control group.
Discussion
The present study aimed to apply virtual body swapping to patients with CRPS and to investigate its treatment effects on pain intensity and BPD. Patients with CRPS seemed to accommodate themselves in the treatment session well and they reported that the training program did not induce aversive pain. In addition, the training program evoked illusionary body perception. As a consequence, the treatment group showed more significant improvement in BPD after the treatment than the control group. However, no difference between the groups was found for pain intensity.
The technique of virtual body swapping therapy on BPD is consistent with novel therapies such as mirror therapy and motor imagery with respect to normalizing sensory-motor cortical representation by manipulating corrective visual information input.29,30 Functional brain imaging studies have demonstrated that representation of the affected limb is enlarged or reduced on sensory-motor cortices, and a correlation between corrective cortical reorganization and pain reduction has been found.31,32 These results imply that BPD correlates with the abnormal change in body schema and that restoring body schema can benefit BPD. Body schema can be altered because our body representation is a complex combination of vision, somesthesis, and motor feedback rather than a simple registration of body location.33,34 Therefore, BPD can be induced when appropriate visual, somesthetic, or motor feedback is not given when moving the body. 35 In the present study, normal body and normal movement are projected onto the patients with CRPS as corrective visual information, while the patients mentally rehearse the movement to provide cognitive and motor input. As mental rehearsal has been used to enhance functional recovery of patients with physical disabilities, 36 it seems promising that virtual body swapping through mental rehearsal could improve physical function of patients with CRPS.
Despite the fact that the virtual body swapping through mental rehearsal was helpful in improving BPD, there was no significant group difference in post-treatment pain intensity. This finding may reflect that single-session treatment is not sufficient to relieve pain intensity. There are incoherent results regarding how many sessions are necessary for treatment using corrective visual feedback, such as mirror visual feedback and augmented reality, to achieve effective pain reduction. Sato et al. 37 reported that even single-session treatment could reduce pain intensity in some patients, but most researchers preferred multiple-session treatment, from one session per week for several weeks to daily basic intense training.13,32,37 Otherwise, our treatment requires preparatory staging before actual virtual body swapping is applied. Because a mismatch between motor intention and proprioceptive feedback causes pain in many pathological chronic pain conditions including CRPS,38,39 even inducing movement intention by virtual body swapping could elicit pain. In this regard, Moseley8,32 suggested and proved the efficiency of an additional training phase before mirror visual feedback to restore body scheme with laterality training and to acclimate to following movement using motor imagery.
The results of this study have important clinical implications for patients with CRPS. Above all, to our knowledge, this study is the first attempt to apply virtual body swapping through mental rehearsal for patients with CRPS. Other treatments using illusionary body perception have been limited because traditional techniques require at least one intact limb or accompanying pain, while virtual body swapping through mental rehearsal extended the clinical venue of CRPS beyond these limitations. Second, most clinical approaches to CRPS have focused on pain reduction. However, this research targeted BPD and pain as one of the main symptom of CRPS and suggested a promising treatment. Moreover, the virtual body swapping is a mechanism-based treatment that aims to normalize a distorted body scheme and resolve conflict between neural networks rather than to transiently relieve pain.
Notwithstanding the above implications, some limitations remain. First of all, the small male-specific sample was utilized as a preliminary study to explore the applicability of a novel treatment program; thus alternatively, bootstrapping method was used in the present study. Bootstrapping method has been known to be useful in solving distribution problem and small sample size analysis as it estimates statistics in prospective big sample from observed data. 28 Nevertheless in further research, a larger sample size with a balanced gender ratio is required to confirm the results of this study. Second, we relied on a single item to measure the virtual body swapping illusion, which may not accurately reflect it. Thus, further research needs to employ more reliable measurements such as a multiple-item measure and brain imaging. Third, the treatment was conducted only once without any preparatory stage. Although there was improvement in BPD in one treatment session, this does not constitute conclusive evidence that one session is enough. In addition to this limitation, the baseline was measured only once and this occurred just before the treatment. Additionally, a followup to determine any long-lasting effects was not conducted. In further research, the baseline should be measured several times before the initial treatment session to obtain a stable baseline, and a followup is necessary to determine the sustainability of the effect after the treatment is terminated.
The result of the present study has demonstrated that the virtual body swapping through mental rehearsal can be useful for improving BPD in patients with CRPS. This finding can be especially beneficial for patients who have difficult body conditions and have been unable to benefit from previous visual feedback therapies because either both limbs are affected or the affected body part has no counterpart. Further studies in a larger and various samples are necessary to establish the virtual body swapping through mental rehearsal as a clinical training program for CRPS.
Footnotes
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2012R1A1A2008624) and the Chung-Ang University Excellent Student Scholarship in 2014.
Author Disclosure Statement
No competing financial interests exist.