
Abstract
Abstract
Pain symptoms have been addressed with a variety of therapeutic measures in the past, but as we look to the future, we begin encountering new options for patient care and individual health and well-being. Recent studies indicate that computer-generated graphic environments—virtual reality (VR)—can offer effective cognitive distractions for individuals suffering from pain arising from a variety of physical and psychological illnesses. Studies also indicate the effectiveness of VR for both chronic and acute pain conditions. Future possibilities for VR to address pain-related concerns include such diverse groups as military personnel, space exploration teams, the general labor force, and our ever increasing elderly population. VR also shows promise to help in such areas as drug abuse, at-home treatments, and athletic injuries.
Background
A
Pain requires cognitive attention. 5 Since humans have a limited attentional capability, 6 a computer-generated simulation of three-dimensional environments that can be interacted with in a seemingly realistic manner—virtual reality (VR)—is capable of transporting an individual into an alternate reality without physically leaving their current environment. 7 VR has been found to reduce performance on divided attention tasks, 8 and patients have less attentional capacity to focus on incoming signals from pain receptors as they shift their focus to interaction with the virtual environment (VE).
VEs can also be used to train patients on preventative and rehabilitative procedures. 9 When used in combination with electrophysiological state-sensing devices such as electroencephalograph (EEG), electrocardiograph (ECG), electromyogram (EMG), and other technology, rich patient biofeedback data can be observed. Commercially available handheld devices and peripheral gaming accessories such as Razer Hydra, Leap Motion 3D controller, Myo armband, and the Virtuix Omni treadmill (to name a few) can be used to incorporate dynamic control mechanisms into VR simulations. The release of the Oculus Rift Developer's Kit (costing approximately US$275) head-mounted display (HMD) in 2013 shed light on a new era of inexpensive VR visualization systems. Because of the game-like scenarios that can be programmed, several studies have reported that patients actually have “fun” during treatment with VR.10,11
Costing up to US$635 billion each year in medical treatment costs and lost productivity in the United States, 12 US$417 billion in Europe, 13 (chronic) pain management is not as “fun” an issue for policy makers. The World Health Organization (WHO) estimates that 22% of the global population has some degree of chronic pain. 14 Though an increased understanding of biological mechanisms underlying pain symptoms, diagnostic procedures, and therapeutic applications have been explored, current treatments for pain often do not result in the complete alleviation of symptoms. 15
General Overview of Pain Management Therapies
Pain management can be divided into four categories (see Fig. 1).
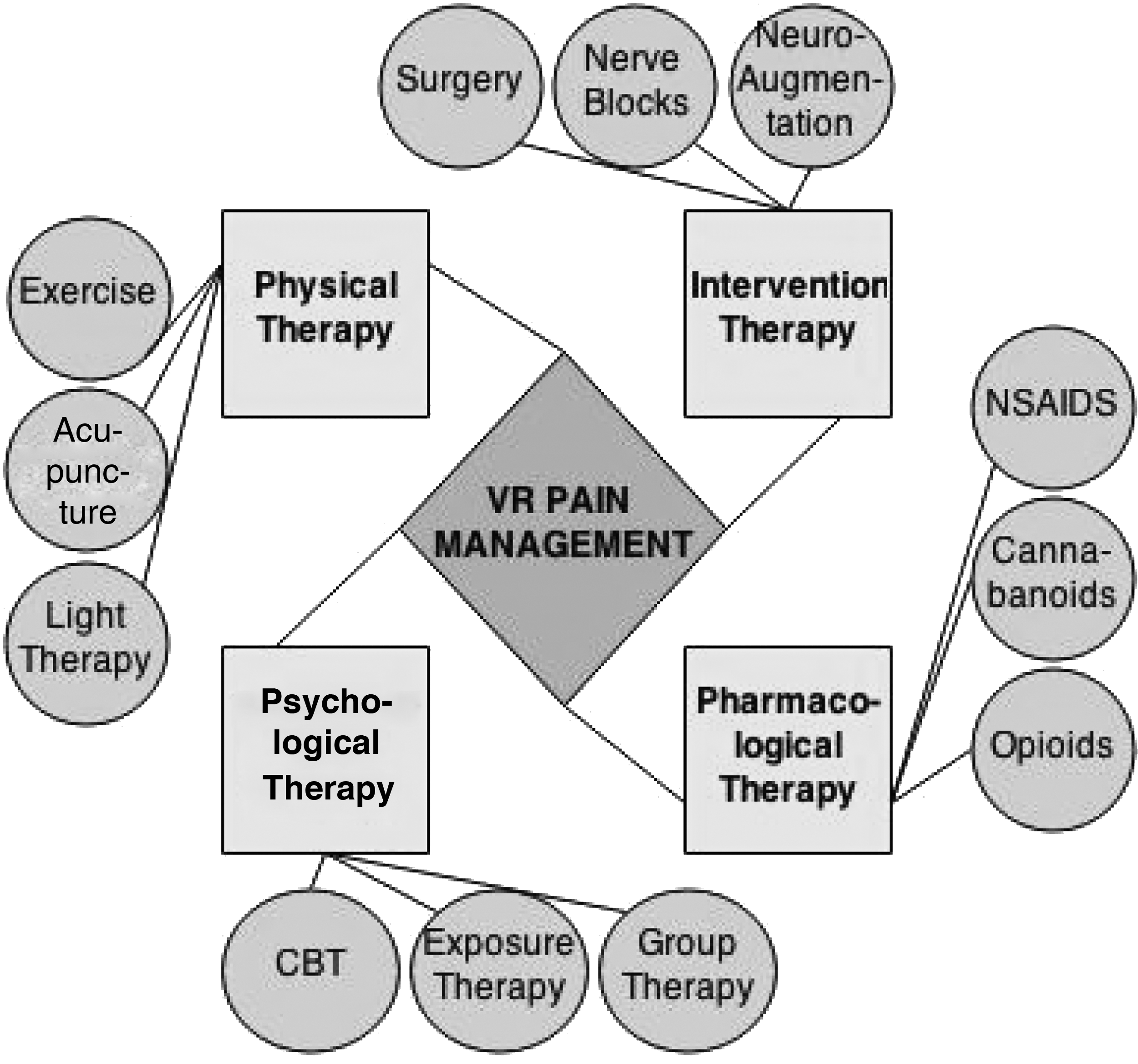
Virtual reality (VR) pain management is an interdisciplinary to therapy designed to attack pain symptoms with an omnidirectional approach.
1. Physiotherapy (physical therapy). The practice of using acupuncture, thermal agents, light therapy, electrotherapy, therapeutic exercise, and some behavior therapy all fall under the category of physiotherapy, which is the treatment of pain by promotion of mobility, functional ability, and routine physical intervention.
2. Psychotherapy (psychological therapy). Problems addressed by psychotherapy are centered on the mental well-being of patients. Techniques involve exploration of thoughts, feelings, and behavior for the purpose of achieving higher levels of functionality and quality of life. Cognitive Behavior Therapy (CBT) teaches patients to analyze and restructure their thought processes while becoming more aware and in control of physiological factors that correlate with mental state—factors such as heart rate, respiration, and so on.
3. Pharmacotherapy (pharmacological therapy). The oral administration of medicinal drugs to relieve pain symptoms is known as pharmacotherapy. WHO guidelines elicit a “pain ladder” for the consumption of pharmacological analgesics for patients experiencing severe pain that cannot be addressed solely with nonmedicinal therapy. 16 The ladder starts with nonopioid drugs such as cannabinoids, paracetamol, dipyrone, nonsteroidal anti-inflammatory drugs (NSAIDs), or COX-2 inhibitors. If pain is not considerably addressed using nonopioids, further progression could require consumption of a mild opioid such as codeine phosphate, dextroproxyphene, or tramadol in conjunction with nonopioids. If pain persists, or the patient is experiencing onset of sudden severe pain symptoms, strong opioids such as morphine, diamorphine, fentanyl, buprenorphine, oxymorphine, oxycodone, or hydromorphone can be issued in conjunction with nonopioids. In patients experiencing neuropathic pain, tricylic antidepressants, class I antiarrhythmics, and anticonvulants are commonly issued to relieve pain symptoms.
4. Intervention therapy. The use of interventional applications to diagnose or locate the patient's source of pain or provide relief is known as intervention therapy. Treatments include injection therapy, surgical intervention, nerve blocks, neuroaugmentation, implantable devices or drug delivery systems, and direct brain stimulation (to name a few). Interventional procedures are most commonly used in combination with standard analgesic methods to reduce opioid side effects and to achieve a better analgesic efficiency.
Room for Improvement
In a general Western healthcare model, patients who experience symptoms of pain must consult a primary care specialist with the hope of obtaining a diagnosis and curative treatment. When such a treatment is unavailable, these patients “expect” a prescription for analgesic medication to relieve their symptoms. Some of these medications might relieve acute pain in the short term, but their utility for treating long-term chronic pain can be controversial. Studies suggest only 32% of patients placed on long-term opioids 17 and 50% placed on antidepressants 18 experience a pain reduction. In addition to an ambiguous success rate, a sample of orally consumed pharmacological drugs can produce a substance dependency in patients. 19 A 2010 U.S. Department of Health and Human Services Nation Survey on Drug Use and Health (NSDUH) reported that approximately 1.7 million people had a pain reliever dependency. 20 Side effects such as mental illness or even noneffectiveness increase pain management opportunity costs and likelihood of unwanted results. Extreme caution must be taken when issuing stronger medicinal drugs, since they oft come with side effects that can impede patient progress if appropriate considerations are not acknowledged.
In 2011, the Health Ministry of New South Wales, Australia, reported the following issues associated with the current model of care for pain management: an overdependence on pharmacotherapy, lack of services approaching pain problems using biopsychosocial approaches, lack of timely access to existing services, an increasing demand for pain management particularly in populations suffering chronic pains as a result of surviving conditions that are associated with or lead to persistent pain, and a lack of targeted services for clients experiencing pain who have differing needs. 21 Having taken these issues into consideration, we observe how VR therapy can be utilized as a low-cost intervention for a variety of pain-related symptoms.
VR Intervention as a Pain Management Technique
VR is a technology that has emerged as an affordable solution for pain management therapy, proven effective in helping patients cope with pain arising from numerous ailments, being acute or chronic. Table 1 displays a number of recent (2012–2014) publications that show the efficacy of VR in the treatment of a variety of pain symptoms.
VR exposes patients to computer-generated sights and sounds, creating visual and auditory stimulus that would otherwise be presented through the physical environment. This method of intervention provides either distraction or training to patients suffering pain symptoms. Distraction therapy has been applied in clinical practice for decades; the foundation of logic backing the technique is based on the assumption that there exist psychological elements in the perception of pain. It is thought that the more attention someone pays to harmful stimulus, the more intense the realization of the pain. Thus, VEs are used to distract patients from ongoing treatments in a seamless fashion, so as to cause minimal amount of actual pain. Just like many other intervention therapies, VR intervention is being used in combination with other analgesic strategies such as training to attack pain symptoms with an omnidirectional approach (Fig. 1).
VR and physiotherapy
Wii Fit from Nintendo® (and other videogames) has shown that peripheral devices can be used to interact with games with new meaning. Game players balance themselves on the Wii Fit™ board, and sensor data are used as a control mechanism in the game environment. One study showed significant improvements in dynamic balance, functional mobility, and a reduced risk for falling in elderly patients when playing Wii Fit™. 22 Another study, focused on the link between elderly diabetic patients and injuries due to falling, concluded that VR has the potential to train patients in balance, strength, and gait so as to reduce the risk of falling. 23 For additional analysis on performance, neuromuscular movements can be monitored using electromyography (EMG). Several studies have shown that when this biofeedback is delivered through a display, sound, or haptic signal, it can serve as a correctional mechanism for the patient and as a monitoring mechanism for the therapist. 24 VR displays can integrate biofeedback notifications into simulations just as games might use status bars, numerical displays, and written or spoken notifications. Quite like videogames, in fact, VEs are interacted with through a variety of human–computer interaction (HCI) factors, which gives therapists the option of incorporating environment control mechanisms that rely on handheld and peripheral gaming accessories requiring mobility. An example of such a mechanism was used earlier, when we mentioned the Wii Fit board. Another example is the Virtuix Omni (omnidirectional) treadmill, which allows users to “walk in all directions, while standing in one spot,” and enables researchers/therapists to expose patients to VEs that must be navigated through by walking. Numerous studies have shown the effect of treadmill training on rehabilitative populations. 25 It is only recently that interdisciplinary researchers/therapists have affordable, commercially available tools to utilize to create more engaging and motivating physical therapy environments.
VR represents an opportunity to both enrich and intensify the experience patients have when receiving physiotherapy. The dramatically interactive nature of VR requires patients to become more involved in the therapy process and can significantly improve both compliance and therapeutic results. During physiotherapy, the main impediment to progress is often pain. VR can help overcome this pain so patients may more rapidly proceed through the therapeutic hierarchy.
VR and psychotherapy
A 17-country study examined the incidence of mental disorders among people with comorbid single or multiple pain conditions. Results indicated that mental disorders followed a linear pattern, with the lowest rates found among individuals with no pain, intermediate rates among those with one pain symptom, and highest rates among those experiencing multiple pain symptoms. 26 Psychological factors are highly correlated with pain; depression, anxiety, and posttraumatic stress disorder (PTSD) are frequent byproducts of traumatic physical injury and chronic pain. 27 VR used within a CBT model can train patients on shifting attention away from pain or stress-inducing thoughts. 28 Self-management (SM) is an action taken by the patient to manage or minimize the impact of pain. 29 Along with guided in-clinic therapy, patients have the opportunity to heal with at-home mobile interfaces like those that have been used in numerous studies to monitor and assist patients in SM over long periods of time. 30 VR can provide a mobile experience that is programmable and useful for targeting patients with special needs. 31
VR exposure therapy targets anxiety disorders in patients with pain symptoms by exposing them to stimuli that trigger unwanted psychophysiological behaviors and training them to condition their psychophysiological responses accordingly. Low-cost EEG systems can be used to monitor real-time brain activity during mobile and immobile tasks in VR. 32 This adds another dimension of analysis for monitoring patients with psychological problems because emotional correlates can be drawn from reading spatio-temporal source dynamics and event potentials during different tasks. 33
VR and pharmacotherapy
Patients can use VR as an adjunct to pharmaceutical drugs for an increased analgesic efficiency. A study, focused on burn pain reduction in adolescent populations undergoing wound dressing, found that patients experienced a significant reduction in pain scores and dosage of Entonix with VR as opposed to otherwise. 34 The combined usage of VR and pharmaceutical drugs has also been utilized in treating by-products of trauma, such as PTSD, with no recorded evidence of negative side effects in the well-being of the patient. 35 The ingestion of pharmaceutical drugs can activate primary physiological systems. VR treatment acknowledges these changes and offers methods for promoting activation of systems otherwise unacknowledged by drug treatment.
VR and other interventional therapies
Attention to acute pain during interventional treatments can be repressed with the use of VR devices.36,37 A pilot study conducted on VR distraction at the dentist found that when designing these interfaces, special attention had to be paid for different patient and therapist domains. For example, devices interfering with the work of the dentist could cause a disturbance during the procedure, and devices that were not engaging enough could fail to distract patients. 38
Future Implications
Approximately US$14.6 billion over the next 10 years has been allocated by the 2014 U.S. Executive Budget to “implement innovative policies to train new health care providers and ensure that the future health care workforce is prepared to deliver high-quality and efficient health care services.” 39
Below, we explore areas and populations that may benefit from the incorporation of VR into existing training and treatment protocols (Fig. 2).
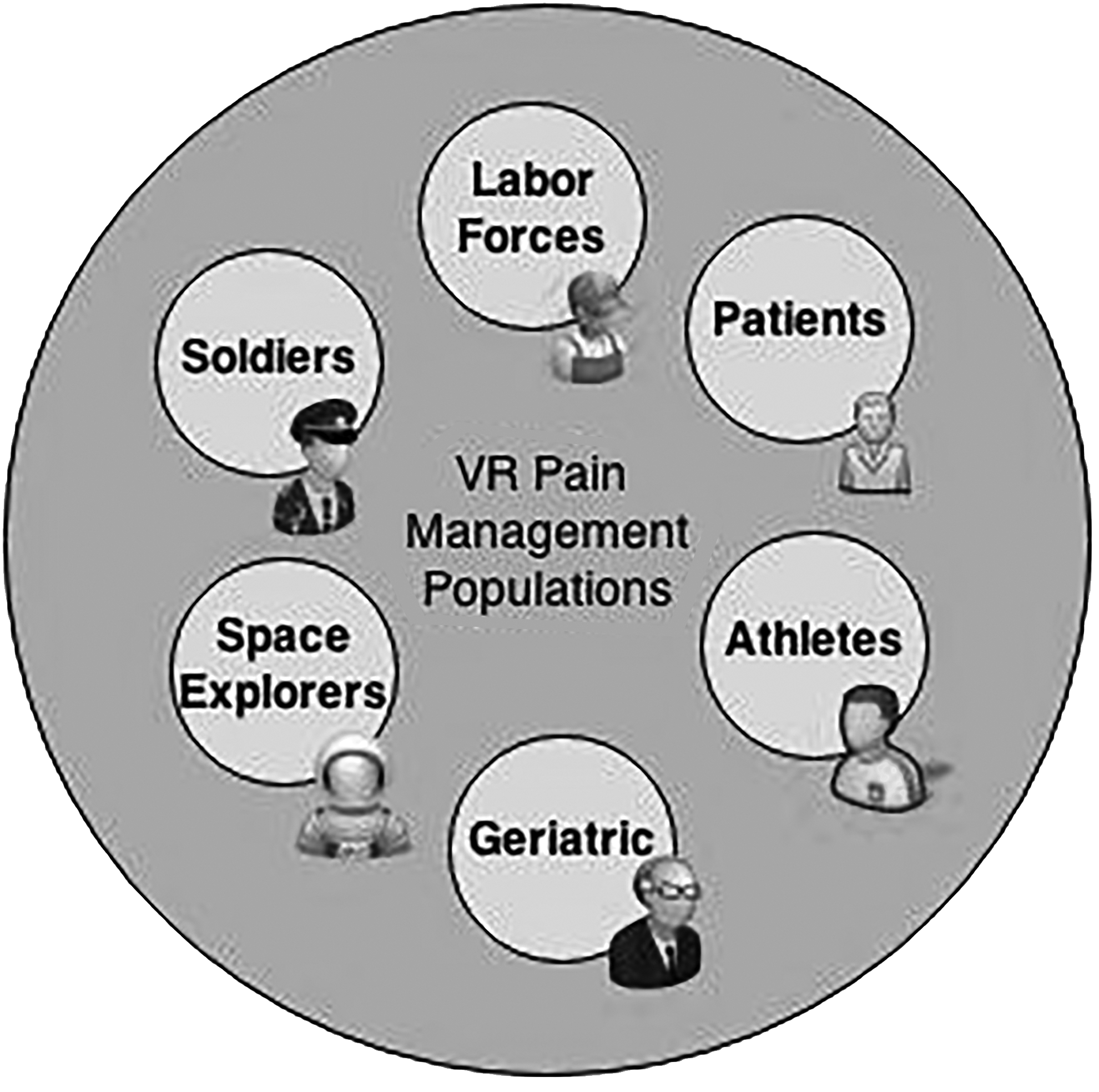
Areas and populations that could benefit with interdisciplinary incorporation of VR.
Military populations
Military personnel exposed to traumatic incidents have a high risk for developing PTSD. Incidents may result in injuries such as severed limbs, traumatic brain injury (TBI), and other acute and chronic pain conditions. Treatment typically requires administration of opioid drugs. Studies have shown that these drugs may induce a high dependency in patients, thus the need to investigate new methods for providing efficient pain relief to veterans. 28 One area of investigation is phantom limb pain, and VR applications are being studied to investigate advancing treatments for this syndrome further. 40 There has been a significant amount of work in applying VR therapies to wounded warriors,28,41–44 and room for improvement still remains. The U.S. Department of Veteran's Affairs was provided $56 billion (from the 2014 Executive Budget) for war veteran healthcare services, which “include innovative programs to educate and support veterans' caregivers, enhance veteran's access to care through telehealth technologies, and support equitable, high-quality care for women veterans in an appropriate and safe environment.” 45
Space exploration
Difficulties associated with illness and injury have accounted for more space exploration failures than any other technical or environment reason. 46 There is room for incorporating VR into space exploration as a countermeasure to deal with the threat of traumatic incidences occurring during extravehicular activity, onset of neuropathic pain during missions, and other pain-inducing incidents. Low back pain in microgravity is one of the most common problems experienced by astronauts. 47 A portable wireless VR solution for back pain telemonitoring has been previously explored to meet similar application requirements. 48 Opportunities such as these provide reason for the two interdisciplinary fields to marry so they can potentially produce a synergy.
Geriatric populations
Injury prevention in elderly populations continues to be an issue, as one out of three adults aged 65 or older falls each year. Falls are the leading cause of both fatal and nonfatal injuries. Arthritis is another big issue among geriatric populations, costing the United States up to US$128 billion per year in medical costs and lost productivity.48,49 Approximately 50 million adults are affected with some form of arthritis. The U.S. Center for Disease Control and Prevention was provided approximately US$14 million from the president's 2014 Executive Budget to expand and disseminate evidence-based programs for the treatment of arthritis. 50 The European Commission also adopted the European Innovative Partnership on Active and Healthy Ageing initiative with the goal to add 2 years to the average healthy lifespan of Europeans by 2020. 51 With resources such as these, we expect to see significant advances in the implementation of VR devices with geriatric populations experiencing pain symptoms in the future.
Pain due to cancer and other chronic injuries
VR has been used in the treatment of illnesses that often result in chronic pain. Yet there remains a need for further exploration of VR treatment methods used in conjunction with traditional analgesics to relieve pain symptoms in these populations. Because pain is not monomorphic, patients can develop intolerance to treatments. This ushers in the use of VR where medication cannot go. VR simulations can be programmed to change in response to patient pain, dialing up the “dosage” as more relief is needed, and dialing down the “dosage” as less is necessary. This ability to control the CyberDose
Occupational injuries
On average, up to 12 people die every day due to occupational injury and illness. In 2012, out of 3,945 U.S. worker fatalities in the private industry, 775 (19.6%) were in construction. Leading causes for worker deaths on construction sites were falls, followed by object impalement, and electrocution. 52 VR techniques can be implemented to train labor force on preventative techniques to reduce the number of fatalities and injuries in the workspace. In addition, the millions of injuries that occur each year in the workplace can be effectively treated using VR to guide both cognitive and physical rehabilitation.
Drug abuse
The National Institute for Drug Abuse has begun a research program to examine the intersection of pain treatment with the abuse of and addiction to opioid medications. Goals are centered on developing alternative pain management solutions (such as VR) with reduced addiction potential, and elucidating risk or protective factors associated with opioid abuse and addiction.
Safe at-home treatments
The National Institute for Health's 8th Pain Symposium in 2012 was primarily focused on exploring self-management techniques for pain management. 53 VR applications are promising for the advancement of at-home medical services because they enable mobility, remote patient monitoring, and treatment specialization capabilities. Much work still needs to be done to quantify the benefits of using topical agents and other safe self-applied techniques such as VR for at-home pain management purposes.
Athletic injuries
Accidents that occur during athletic activity can cause injuries in the form of sprains, knee injuries, swollen muscles, fractures, dislocations, and more. According to the U.S. Consumer Product Safety Commission's National Electronic Injury Surveillance System, more than 1.9 million individuals were treated for a sports-related injury in an emergency medical facility. 54 VR can be incorporated during athletic conditioning to prevent injury, and during rehabilitation as a vehicle on the road to recovery.
Conclusions
The use of VR to treat pain and manage patients with a variety of medical conditions has been well established. VR distraction is effective during medical and surgical procedures, acute pain, chronic pain, pain with rehabilitation, chronic pain of cancer, diabetic neuropathic pain, and related conditions such as pruritus. The technique is safe and effective and has been used on patients with migraine headaches. The often relaxing and stress-reducing capabilities of virtual environments demonstrate wide applicability in behavioral medicine and patients with psychophysiological disorders. These disorders, such as functional abdominal pain, muscle sprain, fibromyalgia and neuropathic pain, and postherpetic neuralgia, are very common in primary care practices. There is significant national and international attention focused on pain management in the occupational and clinical settings.
Table 2 describes some of the funding mechanisms available and those funding agencies that have made pain research one of their priorities. We encourage readers to take advantage of these and other funding resources to continue research on more effective and innovative pain reduction strategies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.